
Abstract
Background:
Military veterans have higher rates of suicidality and completed suicides compared to the general population. Previous research has demonstrated suicidal behaviour is higher in US combat veterans who are younger, suffer from posttraumatic stress disorder, depression and anxiety and score lower on measures of health. However, research on predictors of suicide for Australian veterans is limited. The aim of this study was to identify significant demographic and psychological differences between veterans with posttraumatic stress disorder who had attempted suicide and those with posttraumatic stress disorder who had not, as well as determine predictors of suicide attempts within an Australian cohort.
Methods:
A retrospective analysis was conducted on 229 ex-service personnel diagnosed with posttraumatic stress disorder who had attended a Military Service Trauma Recovery Day Program as outpatients at Toowong Private Hospital from 2007 to 2014. Patients completed a battery of mental health self-report questionnaires assessing symptoms of posttraumatic stress disorder, alcohol use, anger, depression, anxiety and quality of life. Demographic information and self-reported history of suicide attempts were also recorded.
Results:
Results indicated the average age was significantly lower, and the rates of posttraumatic stress disorder, anger, anxiety and depression symptoms were significantly higher in those veterans with history of a suicide attempt. Multivariate logistic regression analyses indicated posttraumatic stress disorder symptom severity, unemployment or total and permanent incapacity pension status significantly predicted suicide attempt history.
Conclusion:
Among a cohort of Australian veterans with posttraumatic stress disorder, psychopathology severity, unemployment and total and permanent incapacity status are significantly associated with suicidality. This study highlights the importance of early identification of posttraumatic stress disorder and psychopathology, therapeutic and social engagement, and prioritisation of tangible employment options or meaningful and goal-directed activities for veterans deemed unable to work.
Keywords
Introduction
Veterans of combat and peacekeeping missions have higher rates of suicidality (McFarlane et al., 2011), and in the United States, veterans are twice as likely to die from suicide compared to the general population (Kaplan et al., 2007). The Australian Institute of Health and Welfare (AIHW) recently reported that between 2001 and 2014, 292 suicides had occurred among those who had at least 1 day service in the military (AIHW, 2016). Of these, 142 were ex-serving, with the majority being males (272 compared to 20 female deaths; AIHW, 2016). Compared to the general Australian male population, the suicide rates were 13% higher for ex-serving male members (AIHW, 2016). Suicidality has also been examined within the Australian Defence Force (ADF). Of currently serving ADF members, 3.9% have reportedly experienced suicidal ideation in the previous 12 months which is more than double that of the 1.7% reported by the general Australian population (McFarlane et al., 2011). Furthermore, 1.1% of currently serving ADF members reported plans of suicide, compared to 0.4% of the general population (McFarlane et al., 2011). Overall, suicidality has been demonstrated to be significantly higher in the ADF population at 4% versus 1.8% in the general population (McFarlane et al., 2011).
Posttraumatic stress disorder (PTSD) is another condition that has increased prevalence within military populations (McFarlane et al., 2011). PTSD is a severe and chronic psychiatric condition characterised by symptom clusters of re-experiencing, hyper-arousal, avoidance and alterations in cognitions and mood following exposure to one or more traumatic event(s) (American Psychiatric Association, 2013). The ADF reported a 12-month prevalence of 8.3% of currently serving personnel who meet criteria for PTSD, compared to 5.2% of the general Australian population (McFarlane et al., 2011). Within the ex-serving population, the Australian Study of Military Veterans reported rates of PTSD at 16.5% within a sample of 14,000 respondents (Dobson et al., 2012).
There are a number of established risk factors for suicide among the veteran population. PTSD has been shown to increase the risk of suicidal ideation (Guerra et al., 2010; Panagioti et al., 2009; Pietrzak et al., 2010), with even sub-threshold PTSD symptoms conferring a similar risk to that of clinically diagnosed PTSD (Marshall et al., 2001). In addition to PTSD, the presence of other psychiatric illnesses including anxiety disorders (Pfeiffer et al., 2009), substance use disorders (Kang and Bullman, 2008; Waller et al., 1999; Zivin et al., 2007) and depressive disorders (Pietrzak et al., 2010) have shown to contribute to increased suicide risk among veterans. In a sample of US Vietnam veterans with chronic PTSD, the risk of suicidal behaviour was found to be higher in younger Caucasian veterans, as well as those who experienced survivor guilt, experienced inconsistent love from their father and had a tendency to cry (Hyer et al., 1990). Another US veteran study found an increased risk of suicide in those with higher symptoms of PTSD, depression and anxiety, and lower scores on measures of mental health, general health and vitality (Freeman et al., 2000).
Research on suicide among Australian veterans has primarily focused on those who served during the Vietnam era, with history of mental illness, lower intelligence and lower education identified as risk factors (Crane et al., 1997; O’Toole and Cantor, 1995). While the US literature on suicide risk factors among veterans is notable, there are limited Australian studies examining the risk factors for suicide attempts among a diverse veteran sample (i.e. from numerous theatres of war or peacekeeping) that also suffer from PTSD.
The aim of this study was to identify significant demographic and psychological differences between veterans with PTSD who had attempted suicide and those who had not, as well as determine the predictors of suicide attempts within an Australian cohort. In particular, demographic information, PTSD severity, current psychopathology, employment status, length of military service, type of deployments and conflict involvement were examined in the context of suicide attempt history.
Methods
A retrospective cohort analysis was performed on data collected (as part of standard practice) from veterans who attended the Military Service Trauma Recovery Day Program (TRP) as outpatients at Toowong Private Hospital (TPH) from 2007 to 2014. A veteran was defined as anyone who had served in the ADF at any time point. All participants were ex-serving regular ADF personnel who had entitlements through Department of Veteran Affairs (DVA) to access treatment for PTSD. All veterans had been diagnosed with PTSD in the past by their referring doctors and had participated in a 3-hour assessment interview with a psychologist, psychiatrist and social worker from the TRP who confirmed the diagnosis of PTSD and assessed suitability prior to the group commencing. The TRP is a 12-week cognitive behavioural therapy (CBT) group programme. Veterans attend 4 days per week for the first 6 weeks and 2 days per fortnight for the remainder. Relapse prevention sessions are held at 3 and 9 months. Ethics approval for the study was obtained from the Department of Veterans’ Affairs (E012/008) and Griffith University (PSY/17/12/HREC). Written consent was voluntarily gained from participants as per the TRP protocol.
Patient demographic and social data collected included age, education, employment status, marital status and service details (type, years of service and conflict(s)). Conflict and peacekeeping service was categorised according to the Australian War Memorial (2016). Patients also completed a battery of mental health self-report questionnaires which assessed symptoms of PTSD, alcohol use, anger, depression, anxiety and quality of life. Past history of suicide attempts were assessed by asking the patient ‘Have you made a previous attempt on your own life?’ The questionnaires were administered on intake to the TRP, with the exception of the Clinician-Administered PTSD Scale for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (CAPS-IV) which was administered at pre-admission assessment (usually 1 week to 1 month prior to the commencement of the TRP). A brief description of each measure is below.
The CAPS-IV
The CAPS-IV was developed by the US National Centre for PTSD (Blake et al., 1990). It is a 30-item clinician-administered assessment tool containing criteria testing the intensity and frequency of all 17 DSM-IV PTSD symptoms. It has shown good sensitivity (0.84), is highly specific (0.95) and has excellent test–retest and inter-rater reliability (Newman et al., 1996). Participants were administered the ‘Lifetime’ version of the CAPS-IV.
The PTSD Checklist for DSM-IV
The PTSD Checklist (PCL) for DSM-IV (Weathers et al., 1993) is a 17-item self-report questionnaire measuring specific PTSD symptoms within three subscales. It has been demonstrated as valid for use within veteran cohorts (Andrykowski et al., 1998). It has excellent test–retest reliability (0.96) (Weathers et al., 1993) and construct validity (Weathers et al., 2009).
The Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item internationally validated self-reported screening tool, developed by the World Health Organization to assess hazardous and harmful alcohol use (Saunders et al., 1993). Scores range from 0 (no problem) to 40 (high risk), and across a review of research the median sensitivity was 0.86 and specificity was 0.89 (Reinert and Allen, 2002).
Dimensions of Anger Reaction
The Dimensions of Anger Reaction (DAR) is a 7-item self-report measure of anger (Novaco, 1975). Scores range from 0 to 56, with higher scores indicating strong anger reactions. The internal consistency is 0.91 (Forbes et al., 2004).
The Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-report instrument measuring symptoms of anxiety and depression with a maximum score of 21 on each depression and anxiety scale (Zigmond and Snaith, 1983). The subscales have demonstrated strong internal consistency with Cronbach’s alphas of 0.82 and 0.83 for depression and anxiety, respectively (Bjelland et al., 2002).
Brief World Health Organization Quality of Life Instrument
The World Health Organization Quality of Life Instrument-Brief (WHOQOL-BREF) is a 26-item self-report questionnaire measuring quality of life over four domains (physical, psychological, social, and environment). It has demonstrated sound reliability and validity in previous investigations (Skevington et al., 2004).
Statistical analysis
Data analysis was performed using R, version 3.1.3 (R Core Team, 2015). Demographic, social, and psychological data of veterans with PTSD who had not attempted suicide were compared to those who had attempted suicide in the past using unpaired Student’s t-test for continuous variables and Fisher’s exact test for categorical variables. Multivariate logistic regression analysis was then performed to calculate regression coefficients (β) and 95% confidence intervals (CIs) of significantly different variables with attempted suicide as a dependent variable. To allow consideration of multiple statistical testing, only those variables remaining significant at a 10% false discovery rate (FDR; Benjamini and Hochberg, 1995) were included in the regression analysis. Additionally, for the regression analysis, the employment category of ‘other’ was combined with ‘full time’ (the population mode) to ensure adequate numbers in each category. Significance level was set at p < 0.05.
Results
Data were available for 229 veterans, including 227 males (99.1%) and 2 females (0.9%) aged 24–86 years (53.3 ± 13.3). A total of 153 (66.8%) had served exclusively in the army, 38 (16.6%) in the navy and 30 (13.1%) in the air force, with 8 (3.5%) having served in multiple branches. In total, 140 veterans had served in conflicts or operations prior to East Timor, with 62 veterans having served in more recent operations. Of the total cohort, 119 veterans had served in Vietnam, 34 had served in Iraq and/or Afghanistan, 58 had served in peacekeeping or peacemaking operations (e.g. East Timor, Somalia, Rwanda) and 18 did not have active service.
Characteristics of patients by history of suicide attempts are presented in Table 1. Age was significantly lower in those who had attempted suicide, 49.4 ± 14.6 compared to 54.6 ± 12.7 years (p = 0.0210, FDR = 0.0478). Employment status was also significantly different between groups (p = 0.0206, FDR = 0.0478), with fewer full time workers (14.8% vs 26.9%) and more not working/totally and permanently incapacitated (TPI) (61.1% vs 37.7%) in the suicide attempt group. Neither service branch (Army, Navy, Airforce) nor type of missions served (e.g. peacekeeping vs war) showed significant differences between groups; however, there was a significant difference between groups in conflicts served, with more veterans having served in conflicts since and including East Timor (contemporary veterans) in the suicide attempt group. There were no differences in marital status, highest education level achieved or number of years of service.
Characteristics of patients included in the analysis.
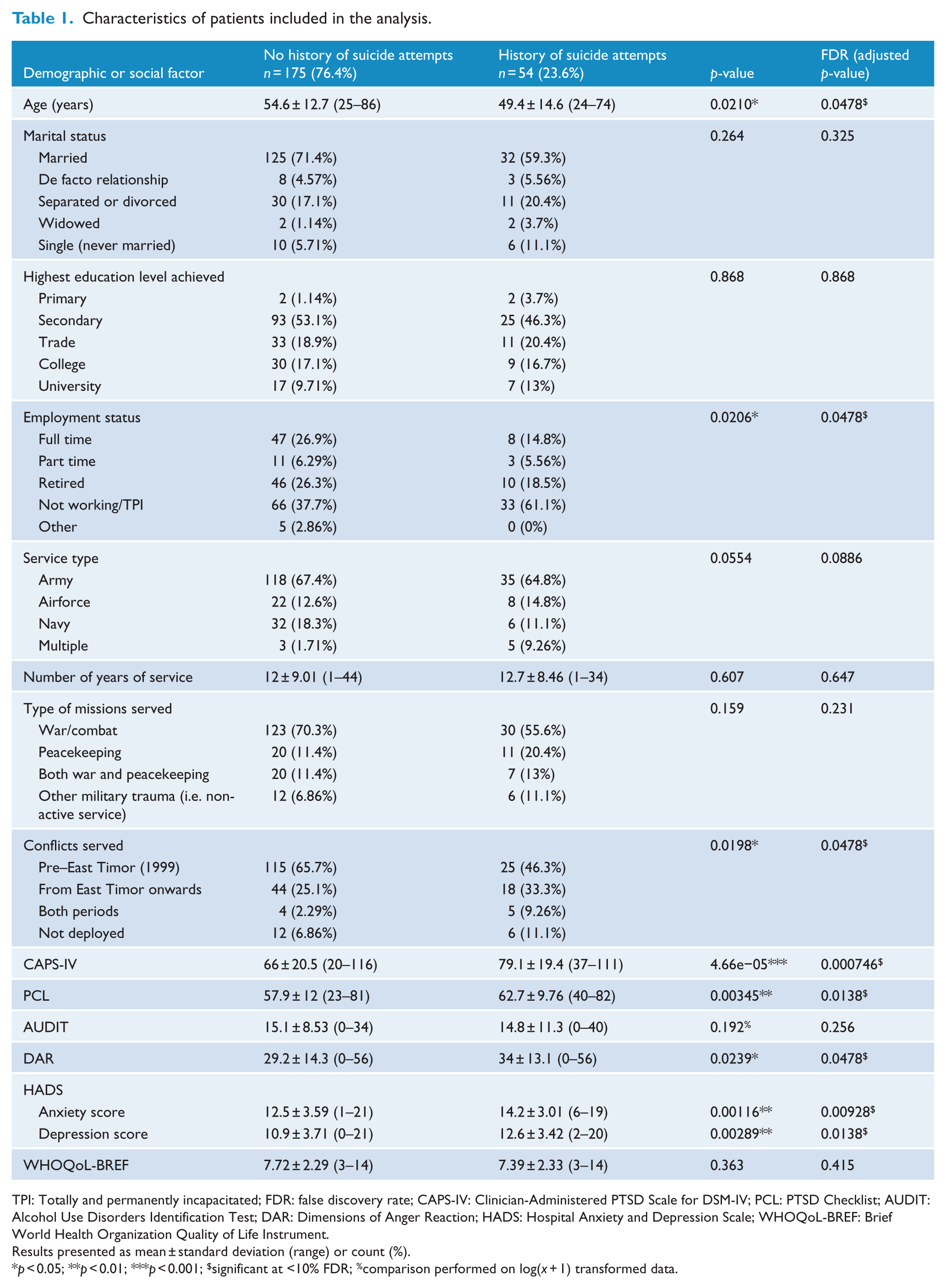
TPI: Totally and permanently incapacitated; FDR: false discovery rate; CAPS-IV: Clinician-Administered PTSD Scale for DSM-IV; PCL: PTSD Checklist; AUDIT: Alcohol Use Disorders Identification Test; DAR: Dimensions of Anger Reaction; HADS: Hospital Anxiety and Depression Scale; WHOQoL-BREF: Brief World Health Organization Quality of Life Instrument.
Results presented as mean ± standard deviation (range) or count (%).
p < 0.05; **p < 0.01; ***p < 0.001; $significant at <10% FDR; %comparison performed on log(x + 1) transformed data.
Of the psychological variables, CAPS-IV, PCL, DAR, and HADS scores were significantly higher in the suicide attempt group (Table 1); all of which remained significant after consideration for multiple testing. There were no significant differences between groups for the AUDIT or WHOQOL-BREF scores.
Results of the multivariate logistic regression analysis are presented in Table 2. CAPS-IV score was significant in the model at p < 0.05, with a 2% (95% CI: [0%, 5%]) increase in risk for every point increase in score (p = 0.03477), as was employment status of not working/TPI, with an increased risk of suicide attempts (odds ratio [OR]: 3.29 and 95% CI: [1.34, 8.08]) (p = 0.00928). It should be noted that although other psychological variables (DAR and HADS scores) were not significant in the model with the inclusion of CAPS-IV, all were significant at p < 0.05 when independently considered in a model with employment status only (results not shown), due to their significant correlation with CAPS-IV score (Figure 1).
Multivariate logistic regression model for risk factors predicting suicide attempts in Australian veterans attending the Military Service Trauma (PTSD) Recovery Day Program as outpatients at Toowong Private Hospital from 2007 to 2014.
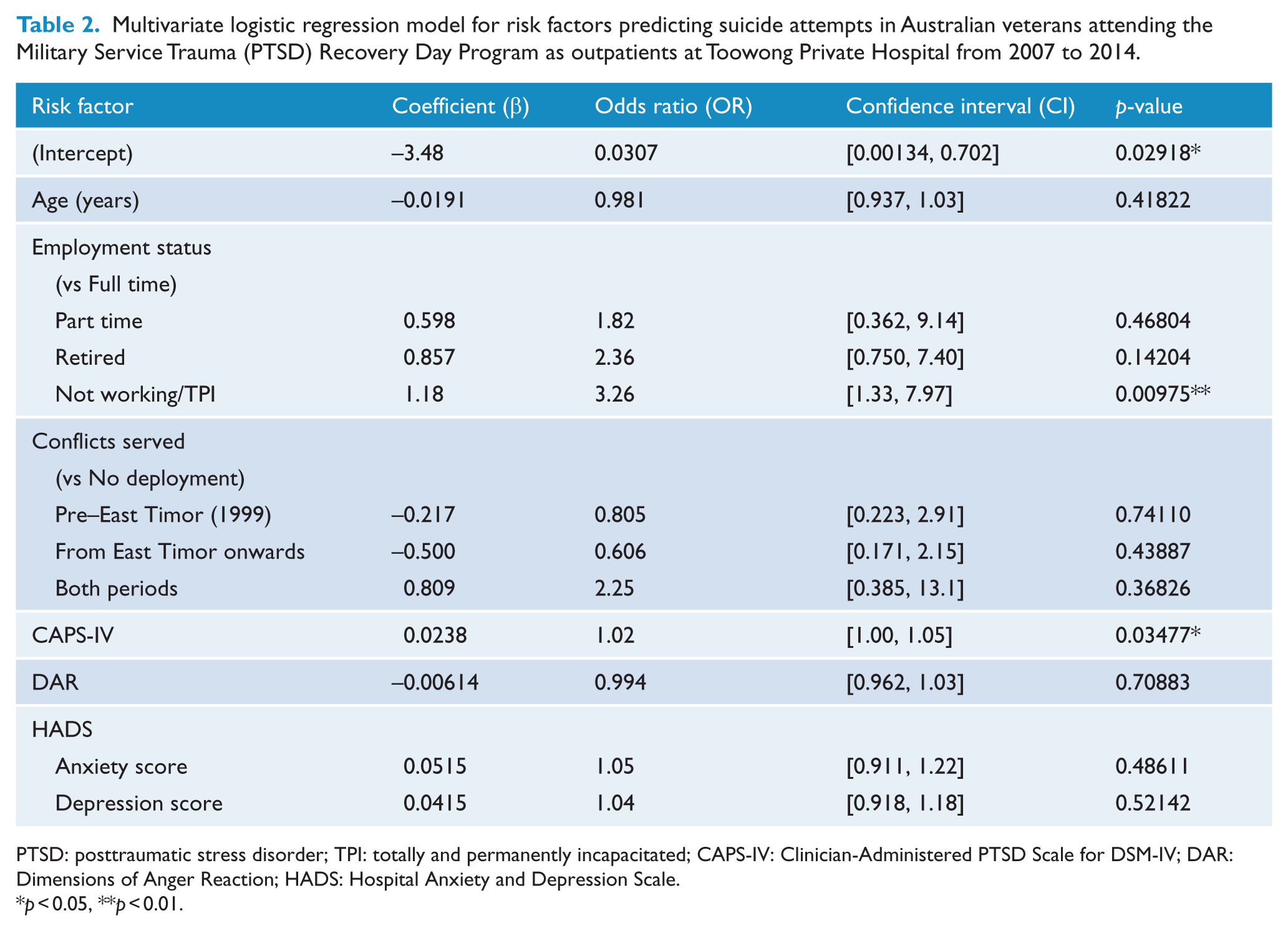
PTSD: posttraumatic stress disorder; TPI: totally and permanently incapacitated; CAPS-IV: Clinician-Administered PTSD Scale for DSM-IV; DAR: Dimensions of Anger Reaction; HADS: Hospital Anxiety and Depression Scale.
p < 0.05, **p < 0.01.
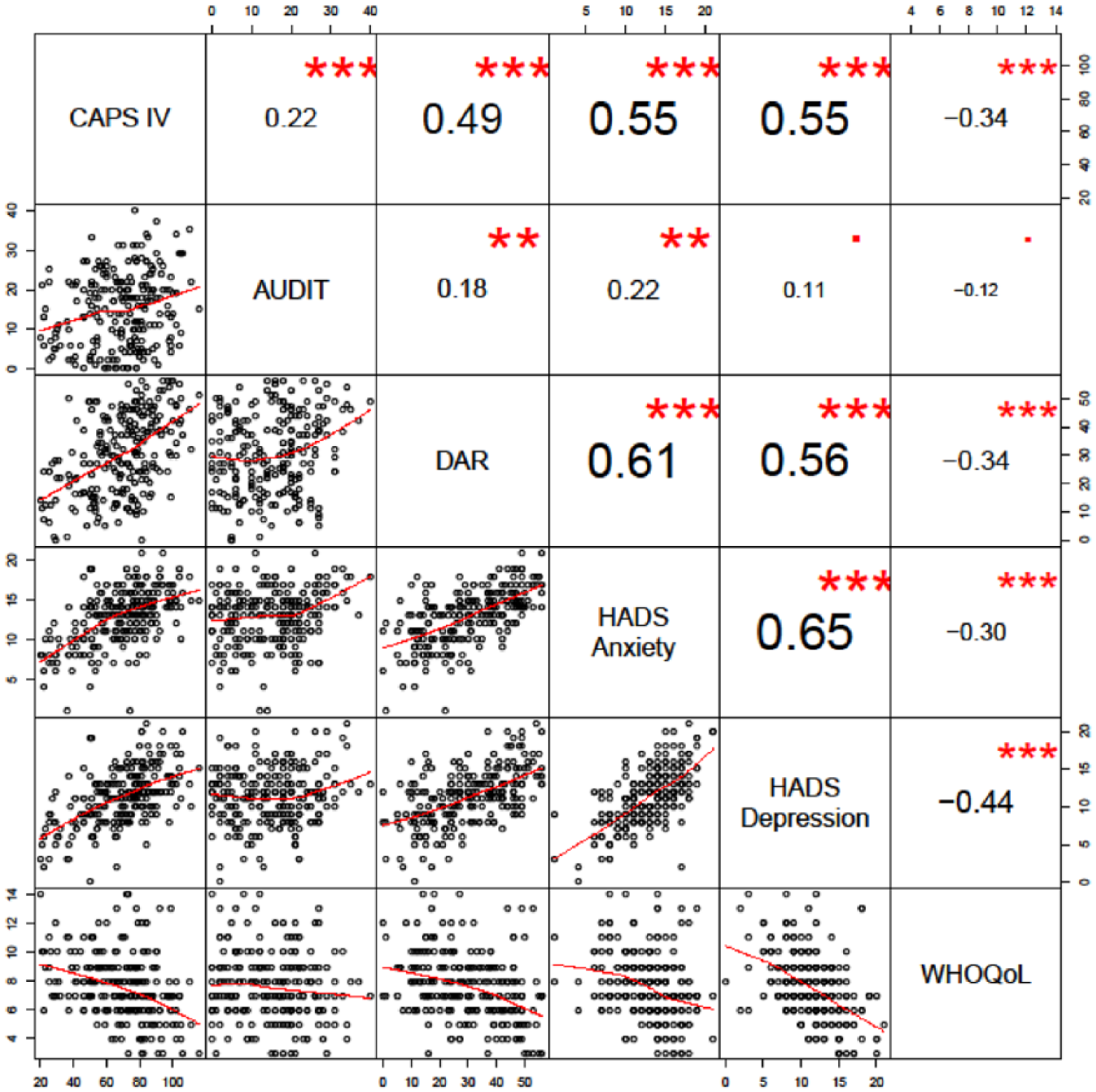
Correlation between psychological variables.
A comparison of psychological factors by not working/TPI and other employment cohorts (working, retired or other) is presented in Table 3. The only difference in addition to CAPS-IV score was HADS anxiety subscale (p = 0.0461); however, both of these only reached nominal significance with consideration of multiple testing.
Comparison of psychological factors between not working/TPI cohort and veterans of other employment status.
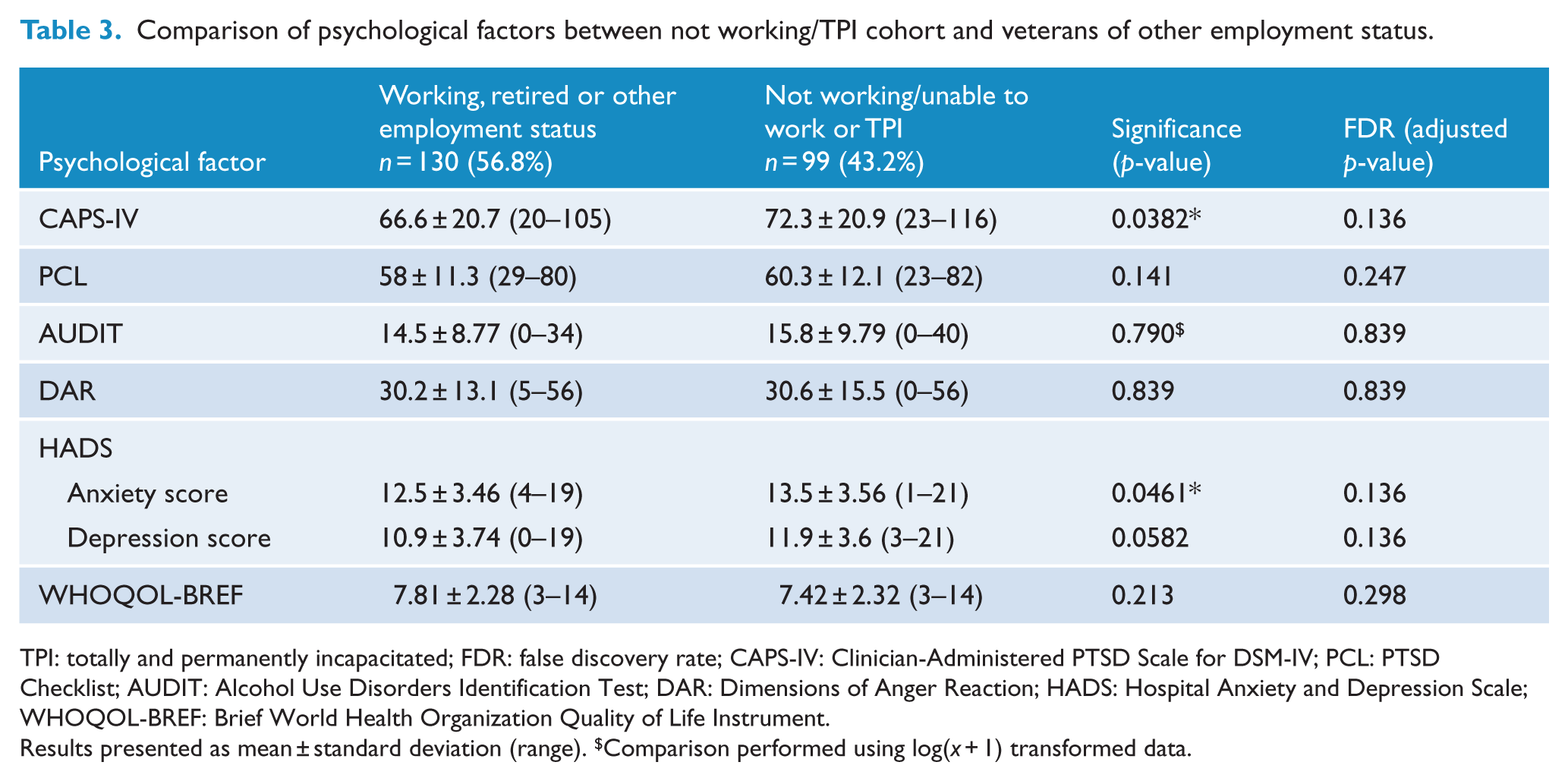
TPI: totally and permanently incapacitated; FDR: false discovery rate; CAPS-IV: Clinician-Administered PTSD Scale for DSM-IV; PCL: PTSD Checklist; AUDIT: Alcohol Use Disorders Identification Test; DAR: Dimensions of Anger Reaction; HADS: Hospital Anxiety and Depression Scale; WHOQOL-BREF: Brief World Health Organization Quality of Life Instrument.
Results presented as mean ± standard deviation (range). $Comparison performed using log(x + 1) transformed data.
Discussion
This study aimed to identify significant demographic and psychological differences between veterans with PTSD who had attempted suicide and those who had not, as well as determine the predictors of suicide attempts within an Australian cohort. Results demonstrated that age, employment status and conflict served (location of combat deployments) significantly differed between veterans with PTSD who had attempted suicide, compared to veterans with PTSD who had not. The average age was significantly lower in the group with a history of a suicide attempt. This finding is consistent with previous research examining suicide among a Vietnam veteran sample in which the risk of suicidal behaviour was found to be higher among the younger veterans within the cohort (Hyer et al., 1990). Given the cross-sectional nature of the current research, a potential explanation for the difference may be the acute presentation of psychopathology in younger veterans as well as survivor bias, that is, veterans who have attempted and completed suicide are not represented in the sample. A further demographic difference in this study was a greater number of veterans deployed to ‘contemporary’ conflicts (including East Timor, Solomon Islands, Afghanistan and Iraq) had attempted suicide in the past. This finding may be explained by the trend that younger age is associated with an increased likelihood of suicide attempts (Hyer et al., 1990).
Demographic results also showed a significantly higher percentage of veterans not working or on TPI within the suicide attempt group. In terms of the psychological differences, as expected, symptoms of PTSD, anger, anxiety and depression were significantly higher among the suicide attempt group also. This is consistent with previous research which has demonstrated similar findings within US combat veteran cohorts (Freeman et al., 2000; Lemaire and Graham, 2011; Pietrzak et al., 2010). For instance, in a US veteran study on correlates of suicidal behaviours, the authors found that unemployment was significantly associated with suicidal ideation, as was a diagnosis of depression, anxiety or PTSD (Blosnich et al., 2016). The relationships between suicide and experiences of anger, anxiety and depression have also been established in previous research. Depression has been shown to be a consistent risk factor for suicidal ideation among veterans (Jakupcak et al., 2009; Pietrzak et al., 2010), while anger has also been linked to suicidality among both veteran and general populations (Hawkins et al., 2014; McKinney et al., 2017). Furthermore, the role of anxiety and agitation as affective states commonly occurring prior to suicidal ideation has been previously established among veteran populations (McClure et al., 2015).
The logistic regression results also demonstrated that PTSD symptom severity (measured by the CAPS-IV) and not working/TPI status were significant predictors of suicide attempt history. For each one point increase in the CAPS, there was a 2% increase in the likelihood of a suicide attempt. To determine the influence of additional psychological risk factors on employment status, a comparison of psychological factors by not working/TPI and other employment cohorts (working, retired or other) demonstrated no significant differences after correcting for multiple testing. This indicates the possibility that an increased risk of suicide in veterans with PTSD who are not working or who are TPI is independent of additional psychological risk factors. These findings suggest that employment may be a protective factor against suicide attempts in veterans with PTSD. However, as data regarding the timing of the suicide attempts were not available, it is uncertain whether the cessation of employment and commencement of TPI status are a result of the suicide attempt (in addition to the PTSD severity) rather than a trigger for it. That said, being part of the workforce has significant benefits to psychological and social wellbeing, including providing structure, social contact, purpose, goal-oriented activity and a role identity (World Health Organization, 2000). For many ex-military personnel transitioning to civilian roles, work provides improved mental health and quality of life (Eisen et al., 2015). Previous research supports the position that unemployment is associated with increased suicide risk, independent of mental illness (Blakely et al., 2003; Classen and Dunn, 2012). Specifically, unemployment has been reported as a risk factor for suicide among civilian populations, with the risk of suicide increasing the longer a person remains unemployed (Classen and Dunn, 2012).
Limitations
Suicide research has always been limited by considerable practical and ethical barriers. The retrospective nature of this research is acknowledged particularly in that data on completed suicides were not captured. It is possible that suicide completers may have different demographic or psychopathological correlates. In addition to study design limitations, the authors were unable to comment on possible contributions from additional suicide risk factors such as recent admissions to hospital and illicit substance use, as well as the possible protective effects of external mental health treatment and psychotropic medications. Furthermore, the determination of TPI by DVA within Australia includes an assessment of physical and psychological injury, with greater severity of pathology resulting in a greater likelihood of TPI status, and as noted above, this suggests the cessation of employment and commencement of TPI status may have been the result of the suicide attempt rather than the potential trigger. Details of TPI assessments and timing of suicide attempts were unavailable, and the influence of physical injury on employment status also could not be determined.
Future research within an Australian cohort should consider these additional factors to further determine a profile of suicide risk among veterans with PTSD and psychological co-morbidities. A specific investigation examining psycho-social outcomes of those deemed TPI by the Australian DVA would also be useful in determining the influence of this on psychological health. With regard to contemporary conflicts, further research is needed to clarify the psychological impact of factors specific to more recent deployments such as peacekeeping roles and rules of engagement, as well as changes in military training, operations or culture.
Conclusion
Among a cohort of Australian veterans with PTSD, those with more severe psychopathology, who served in contemporary conflicts, and who were unemployed or on TPI were significantly more likely to have attempted suicide in the past. Findings demonstrated an individual’s likelihood to attempt suicide increased by 2% per additional point on the CAPS-IV frequency or intensity symptom rating scale. These results highlight the importance of early identification of PTSD, therapeutic and social engagement, and the diligent application of effective treatment modalities. The findings also highlight the importance of prioritising the need for tangible employment options, or meaningful and goal-directed activities in those veterans deemed unable to work, to facilitate socialisation and provide veterans with a sense of continued purpose and worth, potentially reducing suicide risk.
Footnotes
Acknowledgements
The authors with to thank the Australian Centre for Posttraumatic Mental Health (ACPMH) for collaboration in the collection and processing of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Madeline Romaniuk and Sarah McLeay were funded by RSL Queensland under the Veteran Mental Health Initiative at Gallipoli Medical Research Institute.