
Abstract
Objective:
Evidence regarding the role of risk factors in the longitudinal course of suicidal ideation among young adolescents is lacking. We aimed to assess the effects of a range of risk factors, including obesity, academic performance, child–parent relationship, physical maltreatment, and depressive symptoms, on the development of suicidal ideation in young adolescents.
Methods:
A school cohort of seventh and eighth graders was followed for 1 year and differences in the risk factors distributions were examined between depressed and non-depressed adolescents. We further examined risk factors for newly developed suicidal ideation and persistent suicidal ideation in the groups of adolescents based on the presence of suicidal ideation at baseline.
Results:
A total of 1710 young adolescents were recruited, among whom 8.2% were categorised as having clinically significant depression. For depressed adolescents, being obese was associated with a three-fold increased risk of having suicidal ideation. For non-depressed adolescents, physical maltreatment, a feeling of not being cared about and sub-threshold depressive symptoms were the risk factors. The latter two remained robust in predicting newly developed suicidal ideation.
Conclusion:
The current study may shed light on the differential strategies to address suicidal thoughts in depressed and non-depressed adolescents. We emphasise the importance of recognition and management of sub-threshold depressive symptoms and the relevance of obesity, physical maltreatment and a feeling of not being cared about to suicide prevention programmes in early adolescence.
Introduction
Suicide is one of the leading causes of death among youths worldwide. Around 9.7% of adolescents have attempted suicide, and an additional 29.9% have had suicidal thoughts at some point in their lives (Evans et al., 2005). In Taiwan, suicide is the fourth leading cause of death in adolescents aged 15–19 (Ministry of Health and Welfare, 2015). Despite the effectiveness of school-based suicide prevention programmes (Wasserman et al., 2015), concerns have remained over the potential harm of large-scale screening of suicidal behaviours. To target resources for the student populations at the highest risk, screening for mental health problems, such as depression, disruptive behaviour disorders and alcohol/or substance abuse (Liu et al., 2014; Peltzer and Pengpid, 2015), is comparably feasible. Apart from mental illnesses, difficulties in child–parent relationships, including perceived low levels of parental caring, a history of childhood sexual or physical maltreatment, and exposure to recent stressful life events, are also risk factors for suicidal behaviours in adolescents (Carter et al., 2009; Zubrick et al., 2016).
Although suicidal ideation and other suicidal behaviours are both related to suicide, a growing body of research has distinguished risk factors predicting suicidal ideation from those that predict suicide attempts (Klonsky et al., 2016). For instance, the associations between certain mental disorders and suicide attempts may be mostly due to the disorders predicting the development of suicidal ideation, and therefore, when limiting analyses to individuals with suicidal ideation, mental disorders become very weak predictors of suicide attempts (Klonsky et al., 2016). Among those studies on risk factors of suicidal ideation, headache has been reported to have a positive association with ideation (Wang et al., 2007, 2009). A set of novel factors – the body mass index (BMI) and its related constructs, including perceived overweight and body image dissatisfaction – has been researched into their relationships with suicidal ideation; being overweight is shown to be associated with increased suicidal ideation in adolescents (Kim, 2009; Kim et al., 2009; Kim and Lee, 2010).
With advances in our understanding of those risk factors, we may be able to increase the effectiveness of suicide prevention programmes in adolescents. However, most prior results have been from Western societies, while certain risk factors can be culture-bound: for instance, academic pressure may be a risk factor influencing suicidal behaviours in Asian adolescents (Kang et al., 2015; Li et al., 2012; Richardson et al., 2005). Additionally, very few prospective studies have simultaneously taken into consideration child–parent relationship and the adolescent’s own psychopathology. Therefore, the current study aims to elucidate longitudinal risk factors of suicidal ideation in a school-based cohort of seventh- and eighth-grade students in Taiwan. The examined factors include BMI, academic performance, physical maltreatment, stressful life events, depressive symptoms and family dynamics with a focus on the child–parent relationship. We hypothesise that risk factors may differ by presence of depression. The primary aim is to explore the differential risk factor distributions between the adolescents with positive screens for depression and those with negative screening results. The secondary aim is to examine risk factors associated with newly developed suicidal ideation in those who have neither depression nor suicidal ideation at baseline, as well as risk factors for persistent suicidal ideation in those with suicidal ideation at baseline.
Materials and methods
Setting
The study was based on a survey aimed at exploring the relationships among family dynamics, headache, and a set of mood, sleep and behavioural problems in adolescent students in Taiwan (Wang et al., 2009). The first survey took place in the three public middle schools in Taitung County in 2005. The seventh and eighth graders at these schools were the sample population which accounted for 46% of the adolescents aged 13–14 years in Taitung County who attended middle schools at that time and could be regarded as a community-based sample. We recruited all the seventh graders at S middle school and all the seventh and eighth graders at T and C middle schools in 2005, and annually followed up on this cohort while they were in middle schools (Grades 7–9). We continued to recruit all the seventh graders at T and C middle schools in 2006 and 2007. In the current study, we only analysed data for the adolescents who were recruited in the first survey. Body weight and height were measured at baseline and at follow-up. The students answered the survey questionnaires in class by themselves with the help from teachers and school nurses both at baseline and at follow-up. The detailed sampling methods were described elsewhere (Lu et al., 2013). The Institutional Review Board of the Kaohsiung Medical University reviewed the medical ethics of the study (KMUH-IRB-950090). Parental consents were received before the surveys took place, and the Education Department of the Taitung County Government approved the study before it commenced.
Questionnaires
Sociodemographic data such as age, gender, grade and household economic status;
Academic performance, categorised into class rank 1–5, 6–10, 11–15, 16–20, 21–25, 26–30 and after 30, among the students in his or her class;
Family dynamics, including the perceived child–parent relationship, the feeling of being cared about and the perceived parental expectations about his or her achievement;
Stressful life events in the preceding year, including loss of his or her own physical health, financial difficulty of the family, conflicts between parents and child–parent conflicts;
Reported presence of physical maltreatment, defined by a positive response to the question ‘Are you being physically abused (by the seniors/parents in the family)’?;
Presence of suicidal ideation in the past month, defined by a positive response to the question ‘I think about killing myself’.
A validated headache questionnaire for adolescents was used for headache diagnoses with some modifications based on the International Classification of Headache Disorders, Second Edition (Lu et al., 2000; Wang et al., 2009).
A validated depression questionnaire – the Adolescent Depression Inventory – was used to survey depressive symptoms during the past month. This 31-item questionnaire had a high internal consistency of 0.86 and test–retest reliability of 0.76, with a score ⩾19 being defined as clinically significant depression (Huang and Hsu, 2003; Wang et al., 2009).
Data analysis
Sociodemographic data, family dynamics, stressful life events, and other risk factors were first described and compared based on the adolescent’s screening result for depression at baseline. Continuous variables were compared using Student’s t-tests, whereas categorical variables were compared via chi-squared test. At the 1-year follow-up, a positive response to the question ‘I think about killing myself’ was the main outcome measure in this study. To identify characteristics predictive of suicidal ideation at the 1-year follow-up, logistic regressions were performed with suicidal ideation as the dependent factor, and independent factors included gender, grade, BMI category, academic performance, household socioeconomic status, family dynamics variables (unhappy parental marriage, feeling of not being cared about, poor child–parent relationship and parental expectation), reported physical maltreatment, recent psychosocial stressors (financial distress, conflicts between parents, loss of physical health and child–parent conflicts) and baseline depressive symptom score. Values of variance inflation factor and tolerance were checked for collinearity diagnostics with categorical variables being transformed into dummy variables. Hosmer and Lemeshow Test was used to test the goodness of fit in the models.
Given that a substantial proportion of non-depressed adolescents at baseline might later develop suicidal ideation, subgroup analyses were conducted to examine whether the risk factors distributions differed based on the presence of depression at baseline. To further shed light on the course of suicidal ideation in non-depressed adolescents, a subset of seventh graders with negative screens for depression at baseline were followed for an additional year and suicidal ideation was re-assessed at the 2-year follow-up to test whether the risk factors persisted after 2 years. Sensitivity analyses were also conducted to explore risk factors for newly developed suicidal ideation in youth who presented with neither depression nor suicidal ideation at baseline, as well as risk factors to persistent suicidal ideation in youth who already had suicidal ideation at baseline. All statistical analyses were performed via SPSS version 17.0 (Chicago, IL, USA). Alpha level was set at 0.05 (p-value) for statistical significance.
Results
The study recruited 1710 young adolescents in the current analyses, among whom 49.6% were boys. The mean age was 13.28 years (standard deviation = 0.57 years). The cultural backgrounds for the adolescents were Hoklo Taiwanese (62.6%), Taiwanese aborigines (15.4%), Mainlanders (5.8%), Hakka (11.6%) and others. According to the standard of 13-year-old BMI of Taiwanese adolescents (Health Promotion Administration Ministry of Health and Welfare, 2013), 3.3% of the adolescents were categorised as underweight (BMI of 15.7 or under), 64.2% were within normal range (BMI of 15.7–21.9), 14.5% were overweight (males: BMI of 21.9–24.5; females: BMI of 21.9–24.3) and 18.1% were obese (males: BMI of 24.5 or above; females: BMI of 24.3 or above). At baseline, 8.2% of the adolescents were considered as having clinically significant depression; 4.4% reported having experienced physical maltreatment from their parents or other seniors in the family. Those with positive screens for depression differed from the non-depressed students in gender, grade, class rank, household economic status, physical maltreatment, depressive symptom score and a number of family dynamics and stressful life events. Of the depressed adolescents, 50% had suicidal ideation at baseline, and only 4.8% of non-depressed adolescents had suicidal ideation (Table 1).
Comparison of baseline characteristics between depressed and non-depressed adolescents.
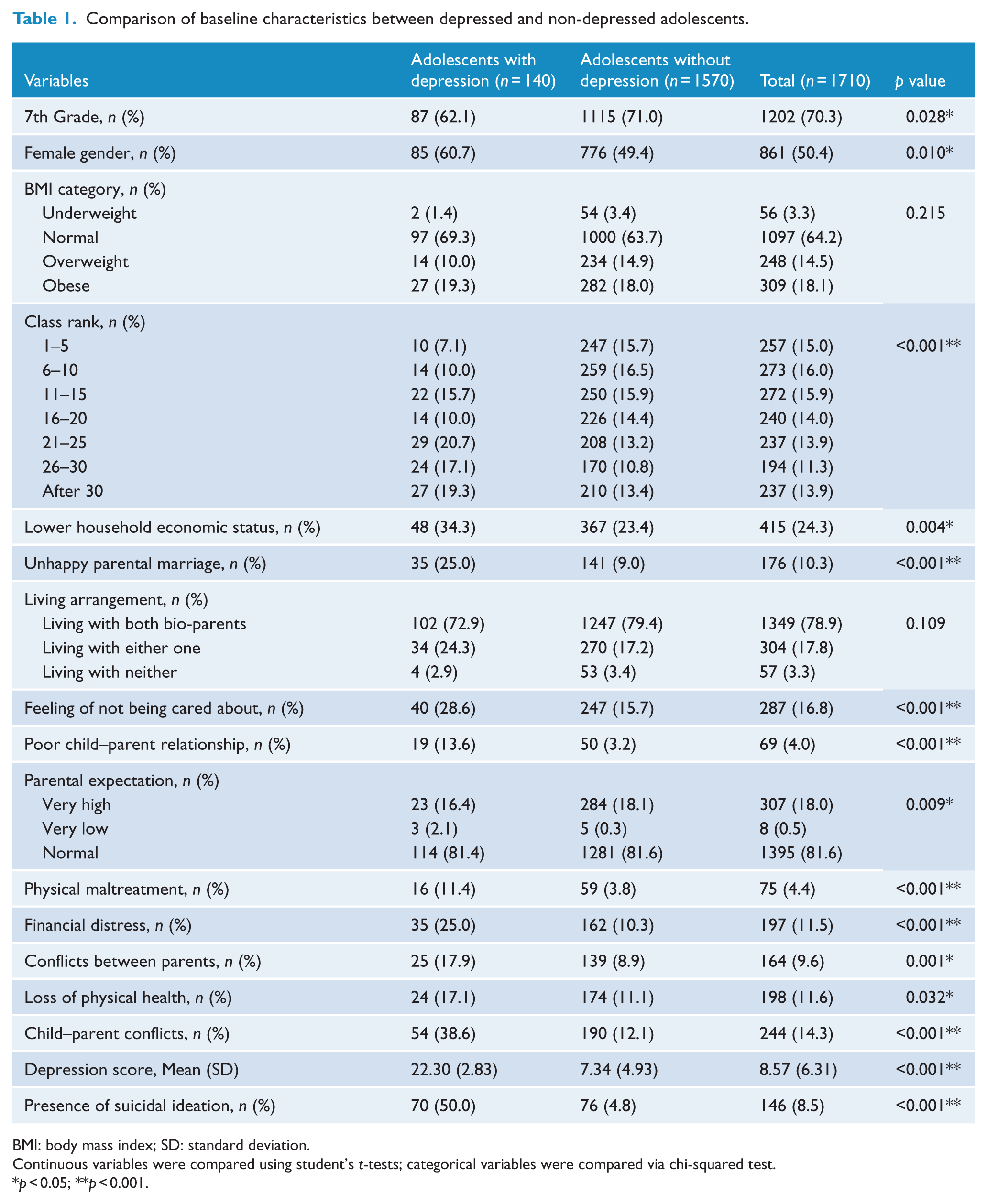
BMI: body mass index; SD: standard deviation.
Continuous variables were compared using student’s t-tests; categorical variables were compared via chi-squared test.
p < 0.05; **p < 0.001.
Presence of any type of headache was first included in the regression model but yielded insignificant findings. Removal of headache-related variables did not result in substantial changes in the coefficients, and headache-related variables were not included in the final analyses. The variance inflation factor and tolerance values for the regression models were within acceptable ranges. In the subgroup analyses based on screening result for depression, being obese was associated with an over three-fold increased risk of having suicidal ideation at the 1-year follow-up (odds ratio [OR] = 3.23, 95% confidence interval [CI] = [1.15, 9.09]) among the adolescents with positive screens (Table 2). For those with negative screens for depression, physical maltreatment (OR = 2.50, 95% CI = [1.08, 5.75]), sub-threshold depressive symptoms (OR = 1.17, 95% CI = [1.11, 1.24]) and a feeling of not being cared about (OR = 2.13, 95% CI = [1.19, 3.81]) were the identified risk factors (Table 3). In a subset of adolescents with negative screens for depression who received follow-up for an additional year (n = 530), sub-threshold depressive symptom score at baseline remained robust as a risk factor to predict suicidal ideation at the 2-year follow-up (OR = 1.10, 95% CI = [1.01, 1.20]).
Factors predicting suicidal ideation at the 1-year follow-up in adolescents with positive screens for depression (n = 140).
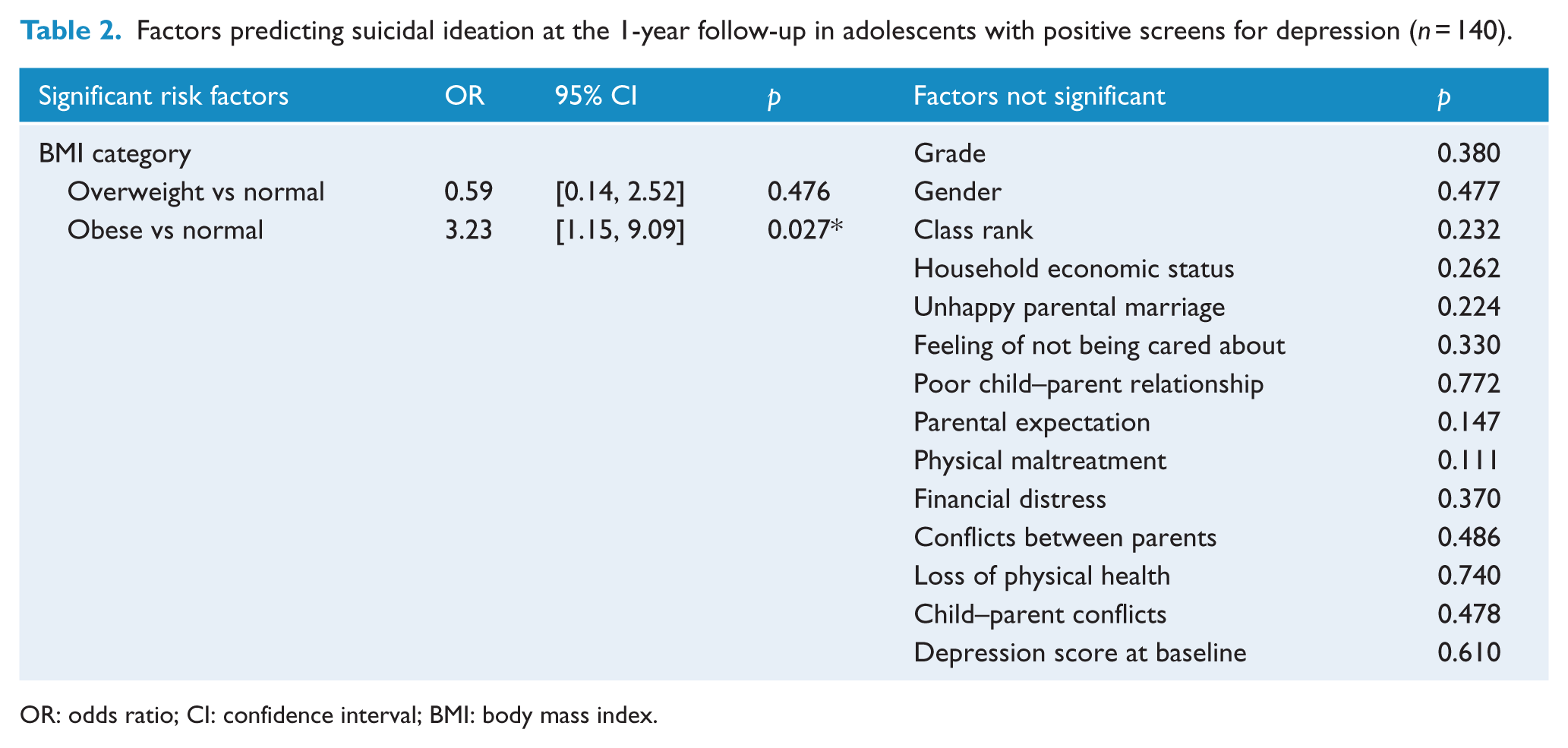
OR: odds ratio; CI: confidence interval; BMI: body mass index.
Factors predicting suicidal ideation at the 1-year follow-up in adolescents with negative screens for depression (n = 1570).
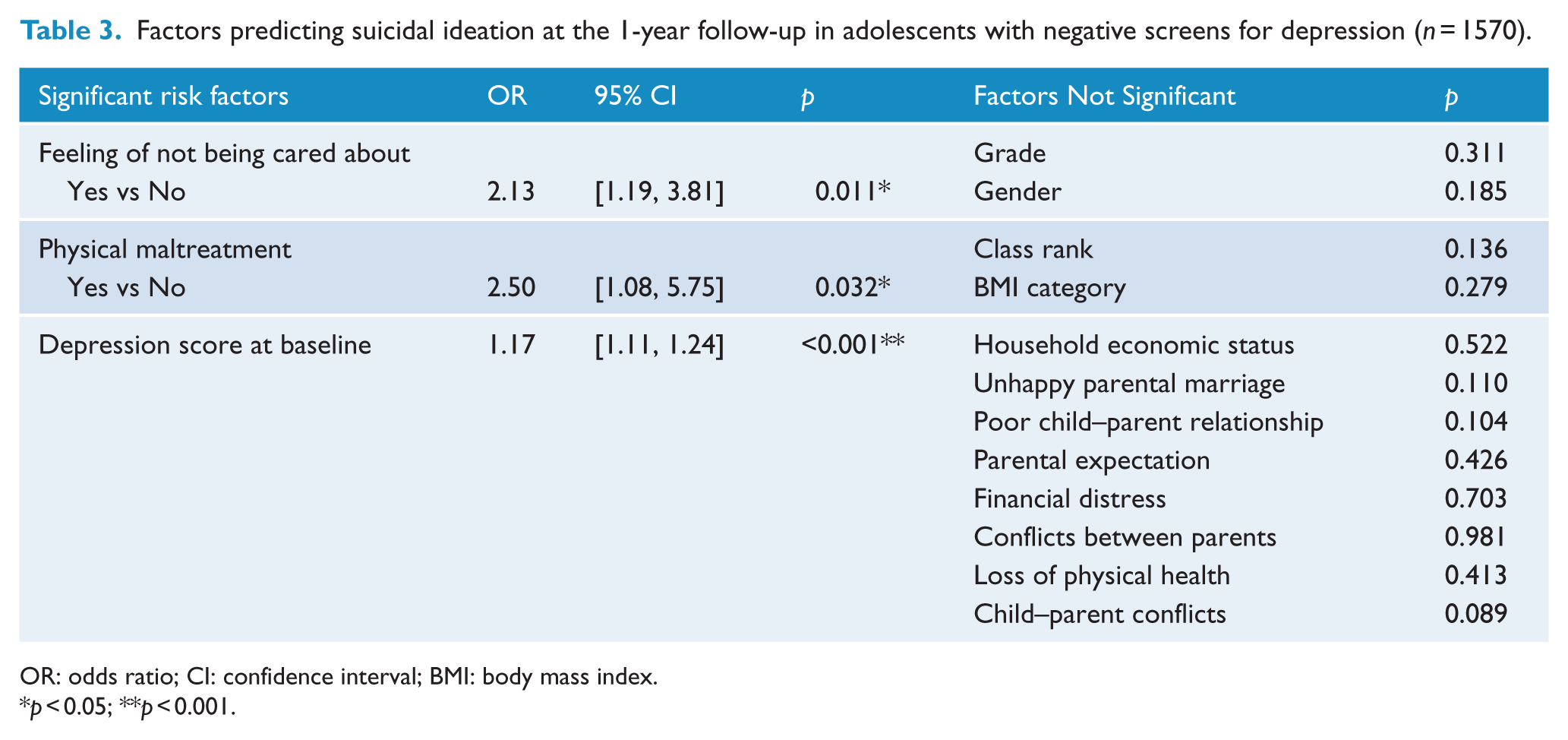
OR: odds ratio; CI: confidence interval; BMI: body mass index.
p < 0.05; **p < 0.001.
With regards to sensitivity analyses, no variables were found to predict persistent suicidal ideation at follow-up in those who had suicidal ideation at baseline. On the other hand, obesity, sub-threshold depressive symptoms and a perceived feeling of not being cared about were the risk factors for newly developed suicidal ideation at follow-up among those who had neither depression nor suicidal ideation at baseline (Table 4).
Factors predicting newly developed suicidal ideation at the 1-year follow-up in those who had neither depression nor suicidal ideation at baseline (n = 1494).
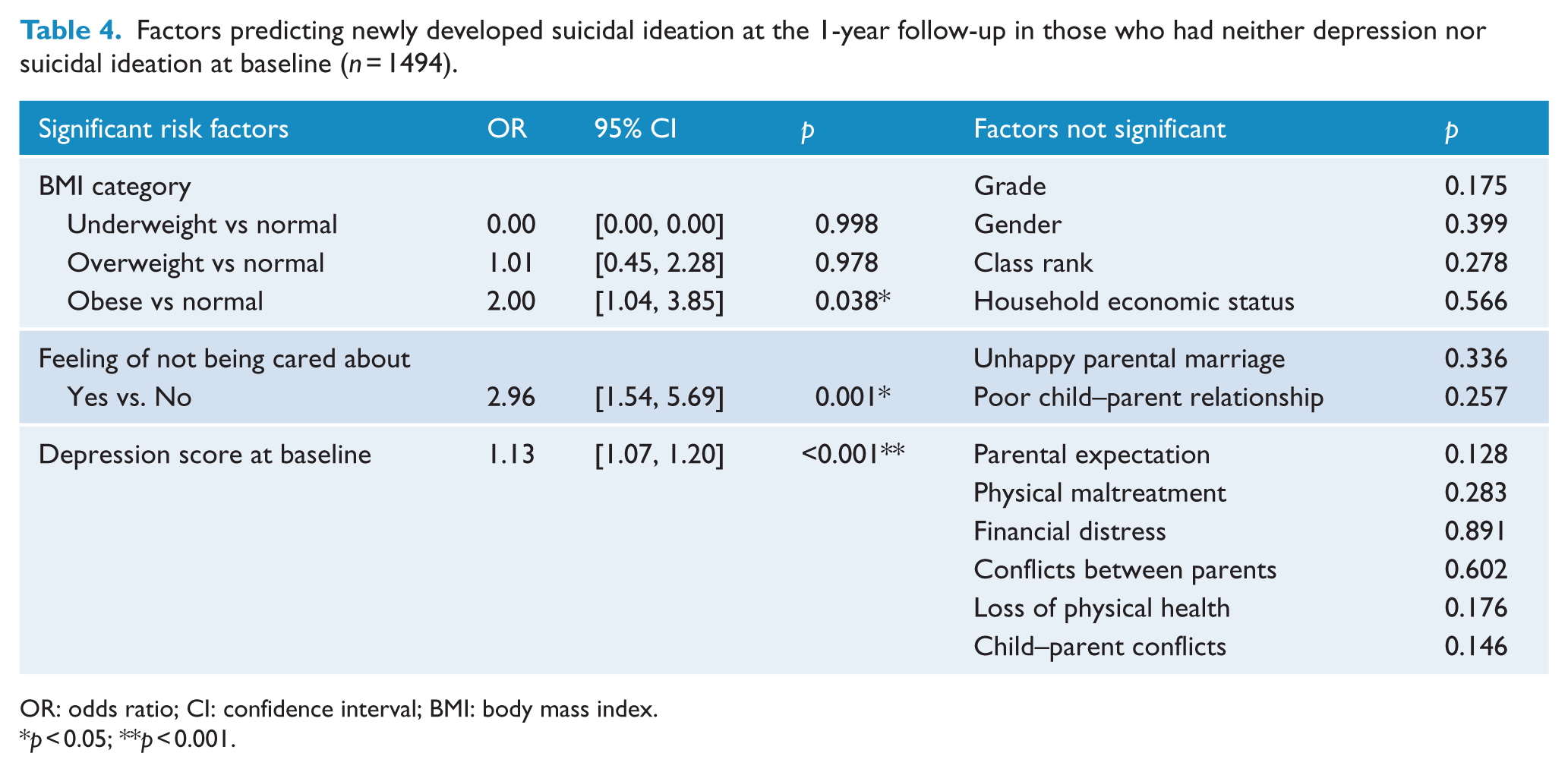
OR: odds ratio; CI: confidence interval; BMI: body mass index.
p < 0.05; **p < 0.001.
Discussion
In this community-representative sample of young adolescents in Taiwan, obesity, physical maltreatment and child–parent relationship are the identified risk factors predicting suicidal ideation in the following year. Additionally, for those without clinically significant depression at baseline, sub-threshold depressive symptom score remains a significant explaining factor for suicidal ideation at both the 1-year and 2-year follow-up. The strengths of the current analysis include the high follow-up rate, and availability of both data on child–parent relationships and a wide range of psychosocial stressors.
We reported that obesity was associated with an over three-fold increased risk of suicidal ideation after 1 year in the current community-representative sample of adolescents with depression (OR = 3.23, 95% CI = [1.15, 9.09]). In the further sensitivity analysis, obesity remained as a risk factor for newly developed suicidal ideation (OR = 2.00, 95% CI = [1.04, 3.85]). Despite the existence of opposing findings which indicate an inverse association between BMI and completed suicide, using predominantly male and Caucasian adult cohorts (Perera et al., 2015), the current results are more in accordance with prior findings based on samples with mental illnesses. For instance, bipolar disorder patients with a lifetime suicide attempt have been reported to have higher mean BMI than those without (Schaffer et al., 2015). Besides, obese adolescents may be common targets of peer victimisation (Bucchianeri et al., 2013), and the pathway from victimisation to depression may be stronger for obese adolescents, with self-concept for physical appearance being the mediator of the link (Adams and Bukowski, 2008). Although being overweight is shown to be associated with increased suicidal ideation, a number of studies in adolescents have also suggested that weight-related attitudes (Kim and Lee, 2010), body weight perceptions (Kim et al., 2009; Lee and Seo, 2013) and body image dissatisfactions (Kim, 2009) are more significant contributors to suicidal ideation than actual BMI. In line with those prior studies, the association between being obese and suicidal ideation in the current study may be related to the process in which victimisation reinforces the negative self-concept for physical appearance and this in turn predicts increases in depression and suicidal ideation. Future efforts to reduce weight-related discrimination and peer victimisation may be warranted in school-based suicide prevention programmes.
Consistent with prior research (Carli et al., 2014), around 8% of the young adolescents had positive screens for depression in this study. Of those depressed adolescents, 50% reported having suicidal ideation at that time, which suggested a high correlation between positive screens for depression and presence of suicidal ideation. For the whole cohort, every point increase in the baseline depressive symptom score was associated with a 15.8% increase in the risk of having suicidal ideation after 1 year. Even for those without clinically significant depression, sub-threshold depressive symptom score was a risk factor for suicidal ideation at the 1-year follow-up, which remained robust in predicting newly developed suicidal ideation. For a subset of students with negative screens for depression, sub-threshold depressive symptoms were found to be the most significant factor predicting suicidal ideation at the 2-year follow-up. In this respect, the current results highlight the importance of early recognition and management of the adolescent’s sub-threshold depressive symptoms to reduce the development of future suicidal ideation.
With an around three-fold increased risk of newly developed suicidal ideation after 1 year (OR = 2.96, 95% CI = [1.54, 5.69]), the current study recognises that a perceived feeling of not being cared about by parents can be a warning sign to identify the at-risk youths with negative screens for depression. Similarly, a recent study has shown that beyond the adolescent’s psychopathology, the perceived child–parent relationships such as ‘parents do not understand my problems’ and ‘parents do not pay attention to me’ are the most significant explaining factors for self-injurious behaviours (Brunner et al., 2014). Perceptions of parental support may be more important than peer support in understanding suicidal behaviours in adolescents (Miller et al., 2015). In a study based on trajectory analyses, family support is shown to be crucial in predicting suicide risk in adolescents in the following several years (Adrian et al., 2016). Among all the examined factors addressing child–parent relationships in this study, a reported feeling of not being cared about is the most significant factor associated with suicidal ideation, even after controlling for sub-threshold depressive symptoms, which can be considered a focus in the future work to improve child–parent relationship in young adolescents.
The relationships between physical maltreatment and a variety of psychosocial and behavioural problems such as suicidal behaviours (Hadland et al., 2015; Lee et al., 2012; McKenna and Gillen, 2016) have been well documented. We found in the present study that physical maltreatment was associated with increased risk of suicidal ideation after 1 year in non-depressed adolescents (OR = 2.50, 95% CI = [1.08, 5.75]). However, physical maltreatment did not predict an increased risk of newly developed suicidal ideation at follow-up for those who had neither depression nor suicidal ideation in the sensitivity analysis. Although speculative, the ‘diathesis-stress model’ may provide a framework for understanding the above findings as well as how early life adverse experiences such as physical maltreatment contribute to suicide vulnerability (Brodsky, 2016). For instance, the existing literature has suggested a ‘gene-by-environment interaction’ between certain genotypes and childhood maltreatment in the prediction of major depression (Beach et al., 2010) and aggression (Weder et al., 2009), both highly relevant to the development of suicidal behaviours. Probably, to select a group of adolescents who have neither depression nor suicidal ideation – even when some of them have already experienced physical maltreatment – may indirectly select a subgroup of adolescents who are less likely to be affected by physical maltreatment in terms of developing suicidal ideation.
Strengths, limitations, and conclusion
In light of the current results, we emphasise the importance of recognising sub-threshold depressive symptoms, strategies to improve family connectedness, and reform of socio-educational system to reduce weight-related discrimination. The strengths of the current study include a large sample of non-referred student population, longitudinal design, and availability of data on BMI, academic performance, physical maltreatment, family dynamics and child–parent relationships. Use of self-reported questionnaires is one of the limitations. Only physical maltreatment is examined, whereas data on sexual/emotional abuse or school bullying are not available. Although academic pressure has been reported as one major source of stress and risk factor for suicidal behaviours in Asian adolescents (Chiou et al., 2006; Kang et al., 2015; Li et al., 2012), we do not find significant associations between academic performance and suicidal ideation in the current study which may be partly attributed to the limitations in the adopted measure for academic performance. Instead of using objective academic reports, the measure relies on student’s own report on his or her rank of academic performance in class. Use of a single item to measure suicidal ideation is one of the major limitations in this study. Besides, only suicidal ideation in the past month (but not lifetime suicidal ideation) is measured. The data of the adolescents are from the first survey that took place in 2005; therefore, the age of data is also a limitation. As psychosocial variables are likely inter-related, multicollinearity needs to be carefully examined in future studies with similar designs. Given that cultural influences need to be considered when interpreting the associations between suicide and its related psychosocial or behavioural factors, caution should be exercised in extrapolating the results into other populations with distinctive cultural backgrounds.
In conclusion, the current study may shed some light on the potential suicide prevention strategies in young adolescents, mainly through screening of depression, management of both clinically significant depression and sub-threshold depressive symptoms, as well as interventions to improve the child–parent relationship with a focus on the feeling of not being cared about. Reform of socio-educational system to destigmatise weight-related discrimination is also warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported in part by grants from Taipei Veterans General Hospital (VGHUST105-G7-1-1, V105C-127, V105E9-001-MY2-1 and VTA105-V1-1-1); Ministry of Science and Technology of Taiwan (MOST 104-2314-B-010-015-MY2, MOST 104-2314-B-418-003 and MOST 103-2321-B-010-017); Ministry of Science and Technology support for the Center for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan (MOST 103-2911-I-008-001); Academia Sinica (Grant No. IBMS-CRC103-P04); Brain Research Center, National Yang-Ming University, Ministry of Health and Welfare, Taiwan (MOHW 103-TDU-B-211-113-003, MOHW 104-TDU-B-211-113-003 and MOHW 105-TDU-B-211-113-003); and a grant from the Ministry of Education, Aim for the Top University Plan. The funding bodies played no role in study design, analysis or interpretation of data in this paper.