
Abstract

To the Editor
M, a 39-year-old woman with no previous medical history, presented with progressive non-fluent aphasia (PNFA), apathy and dementia lasting 2 years. Based on an incomplete diagnosis of a depressive syndrome, she was diagnosed with and treated for major depressive disorder (MDD). Her cognitive function exacerbated with progressively impaired speech and increased hesitation. Dementia deterred her from teaching. Later, her condition deteriorated leading to inability to work and care for herself independently; she was dependent entirely on her husband. On initial neuropsychiatric consultation, M displayed reduced verbal output, mostly monosyllabic. Neuropsychiatry Unit Cognitive (NuCOG) assessment demonstrated severe global cognitive impairment with a total score of 35/100. Magnetic resonance imaging (MRI) revealed extensive increased white matter hyperintensities on T2-weighted imaging, primarily surrounding the ventricles and involving the subcortical region of both hemispheres, and it was associated with ex vacuo dilatation of the lateral ventricles and corpus callosum thinning (Figure 1). Total body X-rays did not reveal bone cysts. Owing to a similar condition, M’s mother and both elder sisters died at 40–50 years of age. Her brother, 2 years younger to her, had recently developed dementia. Genetic analysis revealed a previously unreported homozygous variant in intron 3 of the Triggering Receptor Expressed On Myeloid Cells 2 (TREM2) gene c.482 + 1G > A. This substitution is in the highly conserved donor splice site of intron 3 (phyloP: 3.19). To date, this variant has not been described in the Exome Aggregation Consortium, Exome Sequencing Project or the 1000 Genomes Browser.
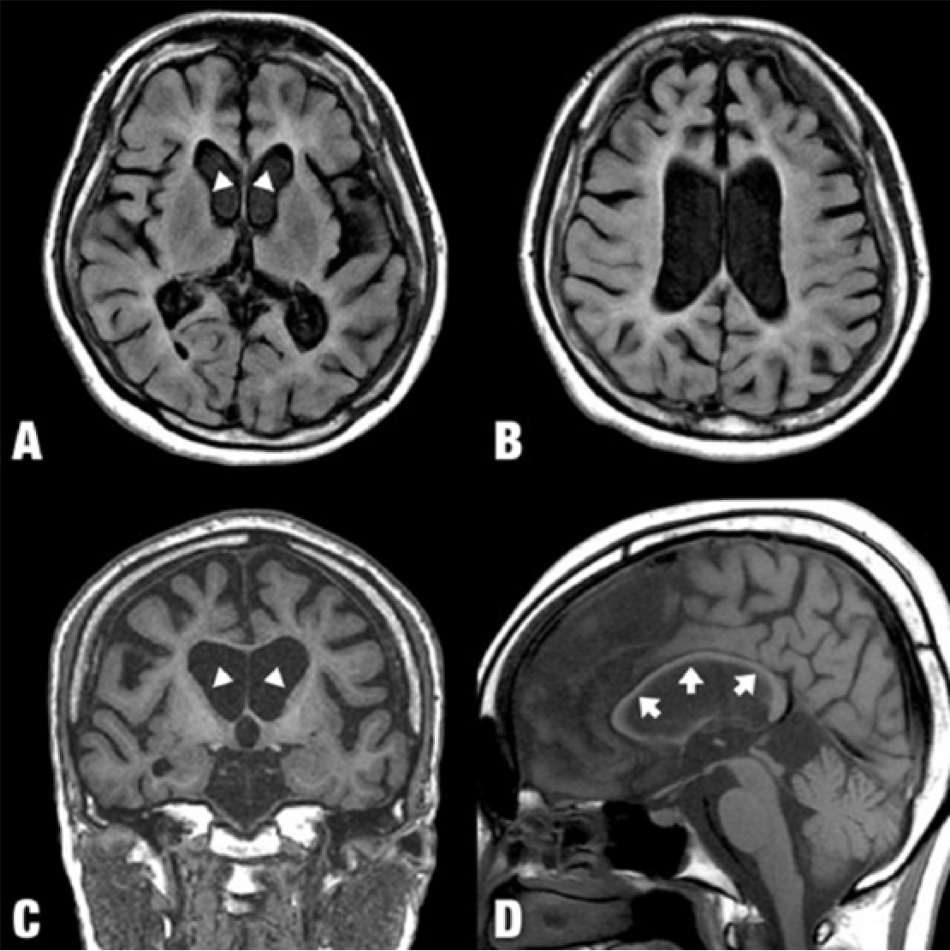
Extensive increased white matter hyperintensities on T2-wieghted imaging, primarily surrounding the ventricles involving the subcortical white matter throughout both hemispheres, best seen on FLAIR (A and B), and it was associated with ex vacuo dilatation of the lateral ventricles, and corpus callosum thinning (arrows). Marked volume loss of the caudate nuclei (arrowheads).
TREM2 mutations have been associated with Nasu-Hakola disease – a rare autosomal recessive disease characterised by early-onset progressive dementia and bone cysts. Three patients with a homozygous TREM2 mutation without bone pathology with behavioural change (apathy, aggressiveness and social withdrawal) and dementia were reported (Guerreiro et al., 2013). In contrast, M did not display neurological deficits, and her clinical findings were similar to those of PNFA (Mesulam, 2003). However, her MRI findings were not consistent with PNFA. TREM2 mutations leading to early-onset dementia without bone cyst formation have so far been reported only in a single Lebanese family (Chouery et al., 2008) and three Turkish families (Guerreiro et al., 2013). M’s is the first such reported case in Asia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Written consent has been obtained from M’s husband for reporting this case.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.