
Abstract

Mood stabiliser: a search for meaning
Detailed critiques of the term mood stabiliser were published a decade ago (Goodwin and Malhi, 2007; Malhi and Goodwin, 2007). The aim of these articles was, firstly, to point out that stabilising mood has many components; for example: conferring acute antidepressant and acute anti-manic effects, the long-term maintenance of mood stability and, perhaps the most critical of all, the prevention of future illness (prophylaxis); specifically warding off the recurrence of both depressive and manic episodes. It was emphasised that this ability to ensure the long-term wellness of an individual (i.e. maximising functional recovery and minimising side effects) was the most important ingredient for successfully managing a chronic and debilitating illness, such as bipolar disorder.
The second point was to highlight that, thus far, only lithium has demonstrable efficacy across all of these facets, although its efficacy on acute depressive symptoms is relatively modest and slow, and possibly differs depending upon whether the depressive symptoms constitute a unipolar illness or are part of a bipolar presentation. It is noteworthy however, that in the treatment of recurrent unipolar depression, only lithium has the ability to augment the effects of any antidepressant from any class. Although lithium’s acute antidepressant effect may be relatively meagre, its ability to facilitate the antidepressant effect of another agent is quite potent (Malhi et al., 2015). Furthermore, in the longer-term management of bipolar disorder, lithium is the most efficacious medication for prophylaxis, albeit in a subset of patients that approximate closely to manic-depressive illness. Research since then (e.g., the seminal BALANCE Study, Geddes et al., 2010) has borne this out and shifted the field in favour of lithium use. Hence lithium’s pole position in guidelines has been retained, and its advantage over other agents has been palpably enhanced.
Contemporaneously, whether mood should define bipolar disorder and be given primacy to the extent that it is, has attracted increasing scrutiny. The importance of considering additional domains such as activity and cognition, and assigning these equal salience has spawned the concept of a multidimensional definition of bipolar illness that is not solely reliant on mood as the primary axis of change (Malhi et al., 2016). This richer and deeper perspective allows for a more nuanced and accurate description of mixed states, which have hitherto lacked a secure home within the mood disorders spectrum. The flavouring of mood episodes with mixed features specifiers as advised by DSM-5 fails to provide a reliable and meaningful depiction of real-world mixed states. But such additional refinement and sophistication comes at a price. It conspicuously complicates the definition of mood disorders and makes bespoke treatment a far more ambitious goal. But ultimately, these seeming impediments to gaining clarity about diagnosis and management are psychopathological advances that will usher in deeper understanding of the nature of these illnesses.
In clinical practice, changes in symptoms and signs that reside on these additional axes can be accurately described and measured just as we measure fluctuations in mood, and can be used alongside our existing parameters to define illness and its response to successful treatment. In other words, the narrow definition of a mood stabiliser that focuses solely on mood per se needs to be broadened to encompass stability of activity and resumption of normal thought processing. An examination of pharmacotherapeutic and psychological interventions along these various domains would allow a more complete understanding of the illness and the potential side-effects of treatments that often limit their use and thereby diminish their effectiveness. This more elaborate approach would also afford the development of more refined and tailored therapies that could provide a more practical rationale for combinations of treatments. For example, agents with actions predominantly on one axis or domain could be referred to as a ‘cognition stabiliser’ or ‘activity stabiliser’. Those that act on more than one domain could then be described as having a combination of actions, for example acting as a ‘mood and cognition stabiliser’. Psychological treatments that presumably target mood and cognition more effectively could then be coupled with pharmacotherapeutic agents that have actions along activity and mood.
Nirvana: a meaningful goal
The term mood stabiliser should be retained because of its widespread familiarity and positive connotations. But at the same time it needs to be defined with greater specificity, such that its components have clinical utility. This is a daunting task but a worthwhile endeavour. The first step is to agree upon a model. We suggest that, alongside mood, cognition and activity should be given equal consideration. The effects of agents that purport to have mood stabilising properties should then be assessed on all of these domains. At the same time, agents that wish to attract the sought-after sobriquet ‘mood stabiliser’ should be able to demonstrate clinical effectiveness and specificity for prophylaxis of mood disorders in addition to any effects that they may possess acutely. Indeed, the latter could be designated as supplementary desirable features but the ability to prevent periods of illness should be stipulated as an essential requirement. These effects are illustrated in Figure 1.
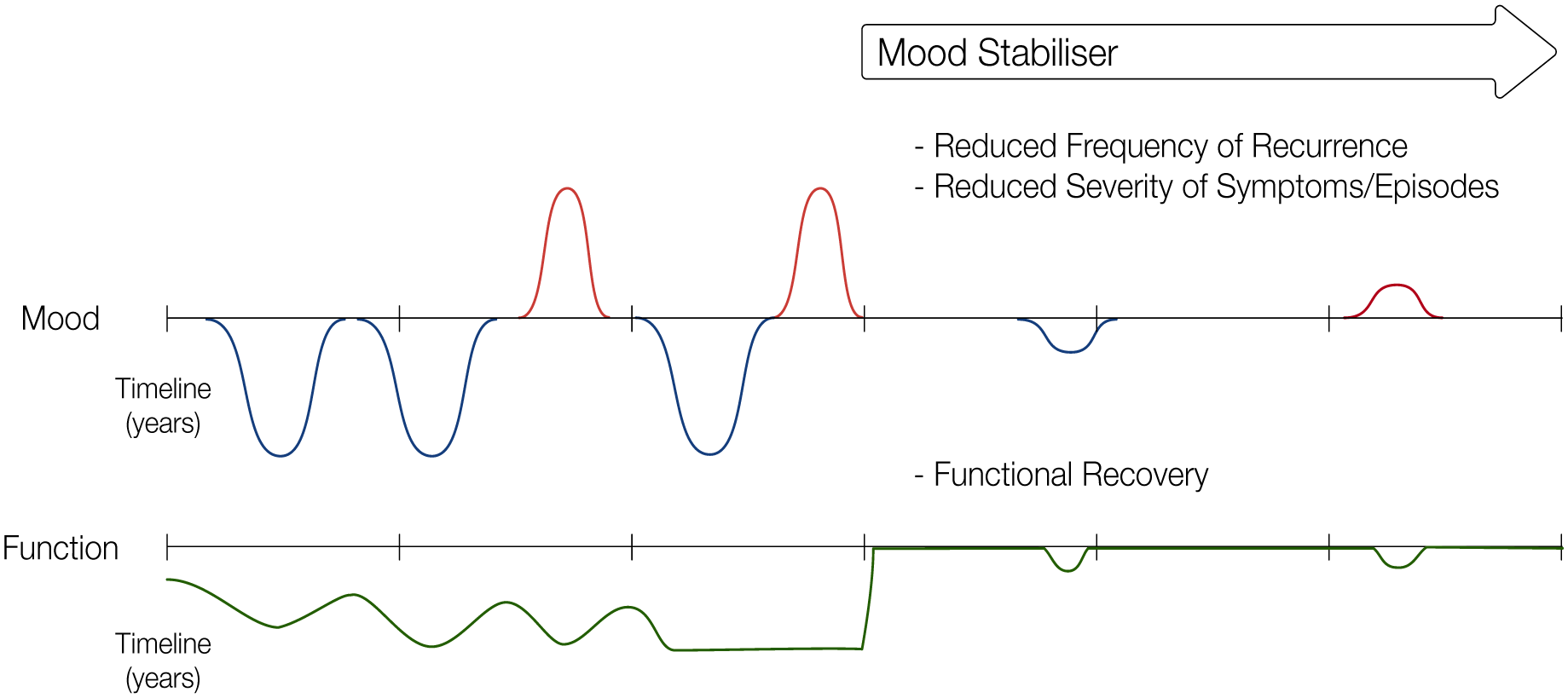
A schematic depicting the key features of an ideal mood stabiliser. An untreated mood disorder persistently cycles over time between depressive episodes and manic episodes, sometimes with brief periods of relative stability. Due to these fluctuations and the little recovery time between episodes, functioning remains generally low, with little improvement in functioning occurring during stable periods. When the disorder is treated with an ideal mood stabiliser, both the frequency of recurrence and severity of symptoms and episodes would be reduced both acutely and over the long term. Accordingly, functioning fully recovers to pre-illness levels. In doing so, an ideal mood stabiliser would achieve generalised prophylaxis, only allowing non-clinically significant breakthrough symptoms and lapses in functioning.
Ultimately, just as nirvana in Buddhist philosophy promises freedom from perpetual suffering, a truly effective mood stabiliser should offer patients with mood disorders freedom from the endless cycling of illness. By better defining the term and investigating the properties of potential treatments we can perhaps envisage a path to enlightenment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.