
Abstract
Objective:
To use expert consensus to inform the development of policy and guidelines for the treatment, management and monitoring of the physical health of people with an enduring psychotic illness.
Method:
The Delphi method was used. A systematic search of websites, books and journal articles was conducted to develop a 416-item survey containing strategies that health professionals should use to treat, manage and monitor the physical health of people with an enduring psychotic illness. Three panels of Australian experts (55 clinicians, 21 carers and 20 consumers) were recruited and independently rated the items over three rounds, with strategies reaching consensus on a priori-defined levels of importance written into the expert consensus statement.
Results:
The participation rate for the clinicians across all three rounds was 65%, with consumers and carers only completing one round due to high endorsement rates. Finally, 386 strategies were endorsed as essential or important by one or all panels. The endorsed strategies provided information on engagement and collaborative partnerships; clinical governance; risk factors, morbidity and mortality in people with enduring psychotic illness; assessment, including initial and follow-up assessments; barriers to care; strategies to improve care of people with enduring psychotic illness; education and training; treatment recommendations; medication side effects; and the role of health professionals.
Conclusion:
The consensus statement is intended to be used by health professionals, people with an enduring psychotic illness and their families and carers. The next step needed is an implementation strategy by the Royal Australian and New Zealand College of Psychiatrists and other stakeholders.
Introduction
The Australian National Mental Health Commission has identified the poor physical health of people with mental illness as one of the major issues for the Australian health care system (National Mental Health Commission, 2012). The reduced life expectancy and ill health of people with mental illness has been termed ‘a national disgrace … [that] … should be a major public health concern’ and ‘an injustice that runs contrary to the United Nations Principles for the Protection of Persons with Mental Illness’ (National Mental Health Commission, 2012: 28). The poor physical health of people with mental illness has also been identified as a priority in recent New Zealand mental health policy (Mental Health Commission, 2012; Ministry of Health, 2012).
Psychotic illness tends to overshadow the clinical awareness of many comorbid physical health risks, most notably smoking rates, alcohol and substance abuse, and a panoply of cardiometabolic risks (Lambert, 2009; Lambert et al., 2003; Stubbs et al., 2015; Vancampfort et al., 2015). Barriers to the recognition and diagnosis of physical health conditions in people with psychosis effectively deny them access to the same standards of care that others in the community would rightfully expect (Kisely et al., 2009; Lawrence et al., 2013). Such barriers are associated with (1) the health care system, (2) health care professionals, (3) patients and (4) their illnesses (Lambert and Newcomer, 2009). The recently published Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical Practice Guideline for Schizophrenia and Related Disorders recognises the serious physical health comorbidity in people with these disorders and includes extensive information on the monitoring and treatment of physical health, with an emphasis on smoking, substance use and cardiometabolic health (Galletly et al., 2016).
A recent meta-analysis of studies assessing the prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders found that the overall rate of metabolic syndrome was 32.5%, with only minor differences according to the different definitions of metabolic syndrome, treatment setting (inpatient vs outpatient) and country of origin, and no appreciable difference between males and females (Mitchell, 2012; Mitchell et al., 2013). Data from the Australian 2010 Survey of High Impact Psychosis (SHIP) revealed that more than three quarters of psychotic patients (with a mean age of 38 years) had abdominal obesity, nearly half were hypertensive, half had abnormal concentrations of low-density lipoprotein cholesterol (LDL-C) and triglycerides (TGs), and one-third had elevated fasting glucose levels (Galletly et al., 2012). Many participants also had potentially modifiable lifestyle risk factors for cardiometabolic disease, including low levels of physical activity and low consumption of fruit and vegetables (Morgan et al., 2014). However, only half of those with self-reported hypertension were taking antihypertensive drugs, and about 40% with hypercholesterolaemia or hyperglycaemia were receiving medication for these conditions. A small number of other Australian surveys have also assessed cardiometabolic risks in people with psychosis. These include a survey of 203 patients with mental disorders (principally schizophrenia and bipolar disorder) attending a public mental health service in Western Australia, which showed that the prevalence of metabolic syndrome was 54% overall, almost double that in the general Australian population (John et al., 2009). A retrospective case record audit of 85 patients aged 16–27 years attending a New South Wales (NSW) community mental health service showed that 55% of males and 42% of females were overweight or obese at a median treatment duration of 8 months. Duration of antipsychotic therapy was associated with higher body mass index (BMI), more than 40% of the total sample had high waist circumference and 45% had metabolic abnormalities (Curtis et al., 2011). The most recent study involved a survey of 60 patients from Melbourne’s Inner-West Area Mental Health Service with a diagnosis of schizophrenia or schizoaffective disorder (Gladigau et al., 2014). Results showed that patients were more likely to smoke, be obese, have dyslipidaemia, have diabetes and the metabolic syndrome compared with the general Australian population.
Of significant concern is the finding that people with a mental illness are significantly more likely to smoke cigarettes than the general population. Just under two-thirds of participants in the SHIP were current smokers (71.1% of males and 58.8% of females), compared to an estimated 16% of the general Australian population (Australian Bureau of Statistics, 2013; Cooper et al., 2012). The use of alcohol and illicit drugs, which also adversely impacts on physical health in general and cardiometabolic risk in particular, is also highly prevalent in this population. SHIP data on lifetime diagnoses showed that 51% of participants had been diagnosed with alcohol abuse/dependence, 51% with cannabis abuse/dependence and 32% with other illicit drug abuse/dependence (Moore et al., 2012). Moreover, these rates had increased substantially since an earlier national survey in 1997–1998.
Mortality rates in people with psychotic illness are higher than those in the general population, with the gap largely attributable to physical illnesses, including circulatory, digestive, endocrine, nervous and respiratory disorders (Brown et al., 2000; Walker et al., 2015). Rates of elevated and premature cardiac mortality are more than twice those of the general population, and it is therefore not surprising that schizophrenia has been described as a life-shortening disease (Babidge et al., 2001; Lambert et al., 2003; Lawrence et al., 2000). Moreover, there is evidence that the gap is widening (Saha et al., 2007).
Purpose of this expert consensus statement
It is anticipated that many physical illnesses which contribute to these deaths could be prevented or treated, if appropriate services and treatments were made accessible for this population group. As there is evidence that physical health problems begin early in the course of psychotic illness, efforts to address these must also begin early (Foley et al., 2013; Foley and Morley, 2011). While there are a number of barriers to adequate care, one key step in the process of improving practice in the area would be clear guidance on the components of treatment, management and monitoring of physical health problems in people with psychotic illness that should be considered core constituents of integrated health care. Such guidance could be used by health professionals, many of whom currently lack the expertise necessary to appropriately treat and monitor physical health problems in people with psychotic illness. Such guidance is also likely to be useful for family members or carers who frequently have responsibility for the care of a person with psychotic illness. This is typically a challenging role, and carers need information and support to empower them to provide appropriate care and to develop better partnerships with service providers.
In order to enable recommendations and decisions to be made about improving the physical health of people with psychotic illness, there is a need to bring together available research evidence and best practice. A number of guidelines in the area of physical health of people with psychotic illness have been produced (see Supplementary Table 1). However, of 18 sets of guidelines found via a systematic search, only 9 reported using a systematic literature search. Moreover, while 13 sets of guidelines used expert opinion in the development process, in only one case did this involve a systematic process designed to minimise potential biases (Bobes-Garcia et al., 2012). Furthermore, only eight sets of guidelines drew on the expertise of health professionals in other areas and only one of the guidelines had input from consumers and carers (RANZCP, 2005). To date, the only available guidelines that give equal weight to the opinions of people with mental illness, carers and clinicians are a recently published set of policy recommendations related to structure/processes of care provision across primary care and mental health specifically tailored to the Dutch health care system (van Hasselt et al., 2015).
There is therefore a need to develop guidance which draws on a range of clinical and consumer and carer expertise using systematic methods that reduce the risk of bias. Formal methods of assessing expert consensus have been used to develop clinical practice guidelines in other health areas, as they provide a way of gathering the views of experts to enable decisions to be made in areas where limited scientific evidence is available (Murphy et al., 1998). They offer the opportunity to involve decision-makers in all relevant sectors and to view practice-based evidence as equally relevant as evidence-based practice (Marmot, 2004). A commonly used consensus method is the Delphi process (Jones and Hunter, 1995; Jorm, 2015). The Delphi method incorporates many of the conditions known to lead to groups of experts making good decisions, including experts making decisions independently, decentralisation of decision-making and a formal method for coordinating and aggregating the group’s expertise (Jorm, 2015). The aim is to use this method to achieve consensus on the most important target domains for the treatment, management and monitoring of the physical health of people with an enduring psychotic illness that might be further developed into operationalised guidelines suitable for implementation by health practitioners, or used by carers and consumers to help direct them to appropriate services. Delphi studies typically use a single panel of professional experts, but in recent years, the method has been used to develop guidelines in the mental health area using expert panels of professionals, consumers and carers, thereby acknowledging that each of these groups has relevant experience to contribute (Berk et al., 2011; Kelly et al., 2008; Langlands et al., 2008). Moreover, this method may facilitate ‘buy-in’ from key stakeholders, thus assisting in dissemination and implementation. In the present project, consumers and carers were included specifically for their expertise in engagement and collaborative partnerships with patients, and in what clinicians should know about the physical health problems of people with enduring psychotic illness. They were not asked to contribute to areas of the expert consensus statement requiring clinical expertise.
Methods
The Delphi method
The Delphi methodology involves consensus building from the ratings of a series of statements by a group of experts (Jones and Hunter, 1995; Jorm, 2015). Statements about treating, managing and monitoring physical health in people with enduring psychotic illness were derived from a search of the lay and scientific literature. For the purposes of this study, the term ‘enduring psychotic illness’ was used to refer to ‘people with recurrent psychoses associated with schizophrenia and other psychotic illnesses’. These strategies were presented to a panel of experts in three sequential rounds and any additional strategies suggested by panel members were included in the subsequent round for all experts to rate. A summary of group ratings was fed back to the panel members after the first two rounds, with panel members able to either change or maintain their ratings. In this way, a list of statements that had substantial consensus in ratings was developed, and those statements with low or conflicting ratings were discarded.
Literature search
A systematic literature search was conducted of websites, books and journal articles for strategies for the screening, assessment, monitoring and management of the physical health of people (aged 18 and over) with enduring psychotic illness. The purpose of this search was to create an initial questionnaire for use by the expert panellists that contained the fullest possible menu of potential strategies. The search consisted of two strategies, one to cover the grey literature (using Google) and the other to cover the scientific and clinical literature (using PubMed). In order to cover the grey literature, the search terms ‘mental health’, ‘physical health’ and ‘metabolic syndrome’ were used to conduct a Google search, in March–April 2013. The first 50 websites (of 176,000 results) listed on Google were thoroughly reviewed. The external links on the websites reviewed were also assessed. An assessment of the subsequent websites beyond the 50 indicated that they were of poor quality and did not contain useful statements. Articles listed on the Collaborative Centre for Cardiometabolic Health in Psychosis website (http://ccchip.com.au/, accessed 6 March 2013) were also searched.
Strategies for screening, assessment, monitoring and management of physical health in people with enduring psychotic illness were obtained from 50 websites (e.g. Mental Illness Fellowship of Australia [MIFA] and the Royal College of Psychiatrists [United Kingdom]), 44 journal articles (e.g. De Hert et al., 2011a; Lambert et al. 2004) and three booklets/factsheets (e.g. Nash M; Physical Health and Well-Being in Mental Health Nursing: Clinical skill for practice 2010; SANE – Mental illness and physical health: the factsheet).
The information gathered from these sources was analysed and written up as individual survey items by a research assistant. This document was presented to a working group comprising the authors (two of whom are practicing psychiatrists, one of whom is a specialist in the area) and a general practitioner with expertise in treating patients with mental disorders, who screened the items to ensure they fitted the definition of strategies that should be used in the treatment, management and monitoring of physical health in people with enduring psychotic illness, were comprehensible, and had a consistent format, while remaining as faithful as possible to the original wording of the information. This resulted in a survey questionnaire containing 297 strategies from journal articles and 258 strategies from the websites. In addition, the questionnaire content was informed by a small number of clinically derived strategies suggested by the working group to fill perceived gaps in content. After several draft surveys, the group produced a list of 416 items that formed the first survey sent to panel members. These survey items were checked against all guidelines identified through the following search, and this did not result in the inclusion of any additional items.
The search of the scientific and clinical literature using PubMed was conducted on 5 December 2014 using the following search terms: (psychosis OR schizophrenia OR schizophrenic OR severe mental illness) AND (physical health OR metabolic OR cardiometabolic OR cardiovascular OR diabetes) AND (guideline OR guidelines OR consensus) with no date limit. The results were filtered to select for articles that were in English and pertaining to humans. The abstracts of the resulting 416 articles were reviewed to determine whether they were likely to be in scope. Articles were regarded as being in scope if they described a clinical practice guideline of the physical health care of persons with a schizophrenic disorder, other psychosis or severe mental illness. This review resulted in 29 articles that were subjected to further review. This process resulted in 18 articles that were in scope and 11 that were out of scope (Bobes et al., 2011; Citrome and Yeomans, 2005; Cohn and Sernyak, 2006; De Hert et al., 2006, 2011b; Dinan, 2004; Goff et al., 2005; Gothefors et al., 2010; Kane et al., 2004; Strasser et al., 2002; van Winkel et al., 2006). A data extraction form was designed by the authors and used by two independent researchers to assess the articles across 18 criteria (see Supplementary Table 1). Subsequently, individual action items were extracted and compared to the strategies outlined in the questionnaire.
Panel formation
There were three separate panels:
Clinicians with professional experience in managing the physical health of people with enduring psychotic illness.
People with enduring psychotic illness, who have experienced physical health issues and who have taken on an advocacy role.
Family members and carers with experience in supporting people with enduring psychotic illness and who have taken on an advocacy role.
Clinicians were recruited through advertisements to members of the RANZCP, the Royal Australian College of General Practitioners, Royal Australian College of Physicians and the Australian College of Rural and Remote Medicine. Their expertise in managing the physical health of people with enduring psychotic illness was assessed based on the information they provided in their expressions of interest, including the setting they worked in, their job title and years of experience. People with enduring psychotic illness who had experienced physical health issues, and family and carers with experience in supporting people with enduring psychotic illness were recruited through expression of interest advertisements in various organisations (e.g. the North East Alliance for Mental Illness [NEAMI] and the Association of Relatives and Friends of the Mentally Ill [ARAFMI], MIFA, beyondblue, Mental Health Consumer and Carer Forum and the Private Mental Health Consumer and Carer Network [PMHCC]). Three people who expressed their interest to participate in the study as clinician panel members did not fit the criteria and were not included.
At least 20 members are necessary for each Delphi panel in order to give reliable results (Jones and Hunter, 1995). In this study, panel membership numbered 96, with 55 clinicians, 21 family members/carers and 20 people with an enduring psychotic illness. In all, 62% of panel members were female (47% of the clinicians, 90% of the carers and 75% of the consumers). Of the family members/carers panel, 13 identified themselves as a carer (close friend or relative) and seven as a family member. One respondent did not provide this information. Of the 55 clinicians on the panel, primary specialties were psychiatry (33), general practice (3) endocrinology (3), cardiology (1), obesity specialist (1), public health medicine (1) and sport and exercise medicine (1). Two respondents identified as physicians and 10 respondents did not provide this information. The median age range was 45–54 years for the clinicians, 55–65 years for the carers and 35–44 years for the consumers.
Questionnaire development and administration
The Round 1 survey was organised into 12 sections (see Supplementary Table 2). Participants were asked to rate each statement, according to whether it should be included in the expert consensus statement, as ‘essential’, ‘important’, ‘unsure’, ‘unimportant’ or ‘do not include’. Respondents were also given the opportunity to suggest additional statements, interventions and strategies that they felt should be included. Where they suggested an item that was within the scope of the expert consensus statement but not already covered, these suggestions were incorporated in the second round survey. Only a subsection of the survey (117 items) was administered to the carer and consumer panels, as it was felt that they would not have the necessary expertise to answer questions that required clinical training and expertise. The clinicians received the whole survey. Panel members completed the questionnaires online using SurveyMonkey® (www.surveymonkey.com).
The study was approved by the Sydney Local Health District (SLHD) Ethics Review Committee (Royal Prince Alfred Hospital).
Statistical analysis
On completion of each round, the survey responses were analysed by obtaining percentages for the clinician, carer and consumer panels for each item. Following a previous Delphi consensus study (Langlands et al., 2008), the following cut-off points were used.
Criteria for accepting an item
If at least 80% of all panels rated an item as essential or important, it was included in the expert consensus statement.
Criteria for re-rating an item
For items rated by all three panels, panel members re-rated an item in the next round if
80% or more of the panel members in one group rated an item as essential or important,
70–79% of panel members in all groups rated an item as either essential or important.
For items rated only by the clinician panel, an item was re-rated in the next round if 70–79% of the clinicians rated it as either essential or important. Items were only eligible to be re-rated on one round.
Criteria for rejecting an item
Any item that did not meet the above conditions was excluded.
Results
Of the 55 clinicians who participated in Round 1, 41 (75%) participated in Round 2 and 36 (65%) participated in Round 3. As all the carers and consumers gave 100% endorsement ratings to all items in Round 1, the Round 2 survey was not administered to these panels. From 159 comments on the first round survey, the working group drafted 14 new items.
See Figure 1 for an overview of the numbers of items that were included, excluded, created and re-rated in each round of the survey. Across three rounds, of the 416 original items and 14 additional items, 386 items (90%) met the criteria specified above for accepting an item.
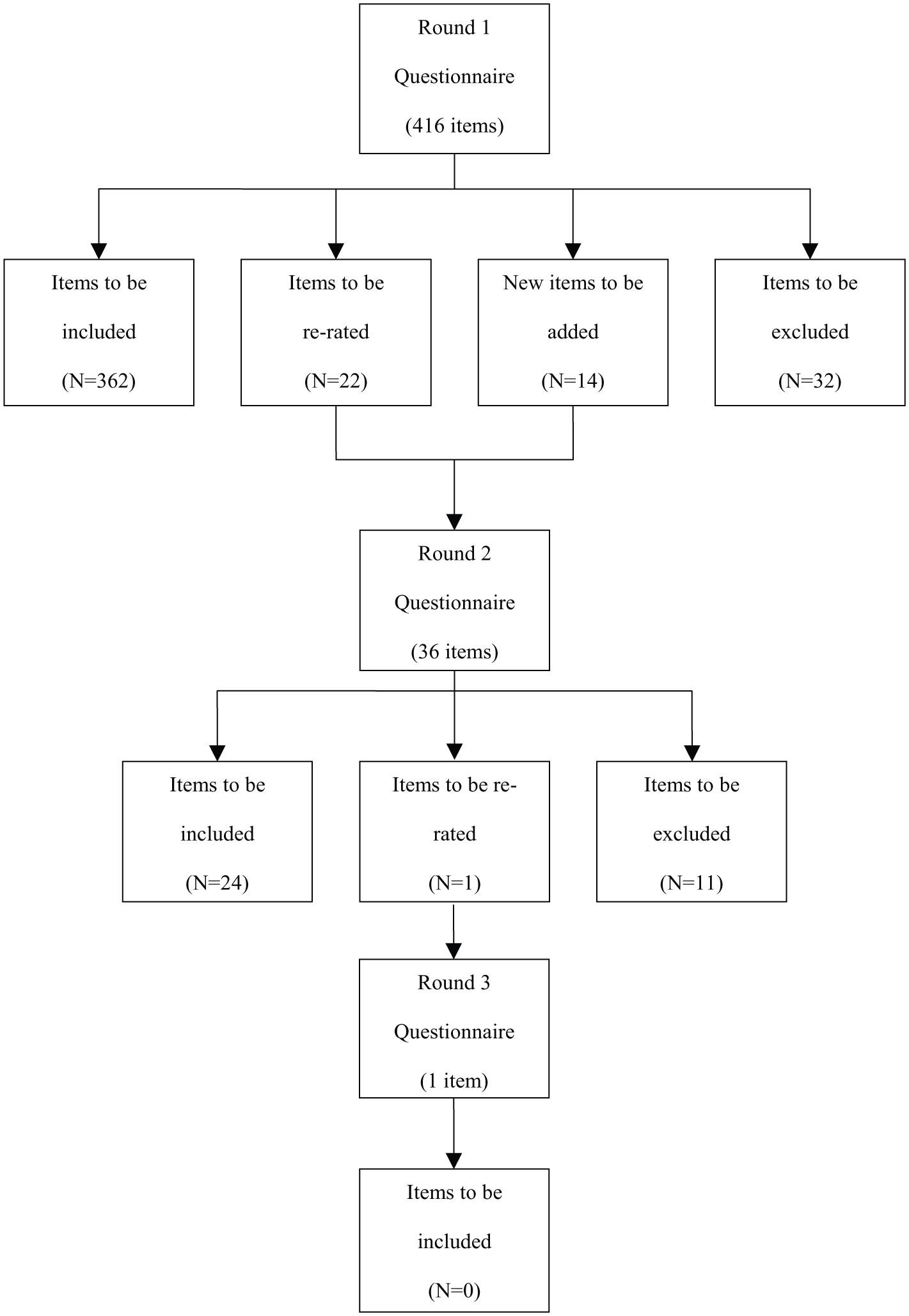
Overview of items included, excluded, created and re-rated in each round of the survey.
The authors prepared a draft of the target items and domains by grouping items of similar content under specific headings and organising the items to make cohesive prose. The included items retained the original wording of the items as much as possible, while remaining easy to read.
The final consensus-derived statement provides strategies for the screening, treatment, management and monitoring of physical health in people with enduring psychotic illness. The endorsed strategies provide information on engagement and collaborative partnerships; clinical governance; risk factors, morbidity and mortality in people with enduring psychotic illness; assessment, including initial assessment and follow-up assessment; barriers to care; strategies to improve care; education and training; treatment recommendations; medication side effects; and the role of health professionals.
Discussion
The project aimed to identify strategies that could be implemented by those responsible for the treatment, management and monitoring of physical health in people with enduring psychotic illness. Overall, 386 strategies were endorsed from a comprehensive range of suggestions. The endorsed strategies were written into a consensus statement which is freely available to organisations in order to inform policy and practice.
Commonly, the methodology used to develop a consensus statement or clinical guidelines is based on a systematic review of the literature, extraction of quantitative data from the identified relevant studies and a formulation of recommendations based on the strength of the evidence. However, the area of practice covered by the present consensus statement was not amenable to such an approach for two reasons. The first is that there was an absence of suitable evidence. The second is that some of the issues covered, such as clinical governance and the roles of professionals, are informed by values and opinions and are therefore not amenable to a randomised trial approach. Instead, the current statement has used expert consensus as a way of gathering practice-based evidence and to make systematic judgements about the knowledge and skills that health practitioners need to provide high-quality integrated care for people with enduring psychotic illness. This method has been widely used to develop clinical practice guidelines in other areas (e.g. endometriosis management [Schleedoorn et al., 2016], withdrawal of life-sustaining measures [Downar et al., 2016] and cardiac monitoring of high-dose verapamil in cluster headache [Koppen et al., 2016]).
A particular advantage of using the Delphi method to develop this consensus statement is that equal value is given to the views of various categories of experts. The inclusion of a group of clinical practitioners working directly with patients, and the equal weighting of their views with academic experts has resulted in a set of recommendations with a strong and equal focus on practice-based evidence. This equal weighting differentiates this expert consensus statement from most guidelines currently available (see Supplementary Table 1).
However, the Delphi method used in this study does have some limitations, including a potential dependence on a weak evidence base (particularly in the area of interventions for physical comorbidities) as a source of questionnaire items. In addition, the quality of the final guidelines depends on the type of panel members involved and their level of expertise.
In order to compare the current statement with previous guidelines from Australia and New Zealand, we conducted an additional search of the National Health and Medical Research Council (NHMRC) Clinical Practice Guidelines portal and the New Zealand Guidelines Groups website in 2014. This search revealed two sets of guidelines covering a similar domain to the current expert consensus statement. One set of guidelines was produced in 2010 by the School of Psychiatry and Clinical Neurosciences and The University of Western Australia for use by psychiatrists and general practitioners (Stanley and Laugharne, 2010). They were developed through an extensive review of the literature and best practice guidelines and covered medication effects, lifestyle factors, physical conditions (pre-existing or developing) and allergies, alcohol and illicit drug use, and psychosocial factors. These guidelines largely focus on what individual practitioners should do and provide practical tools for implementation by the individual clinician. They also included consultation with consumer and carer organisations. However, unlike the present consensus statement, they do not cover broader organisational policies and practices. Another difference is that the earlier guidelines were written by a team from one organisation and did not involve a broader consultation with clinical experts nor did they involve consumer and carer expertise. A second set of earlier guidelines, produced by NSW Department of Health (2009), was more similar in scope to the current expert consensus statement. They were developed by an expert working group of clinicians and senior managers through a process of evidence review and consultation, and were written specifically for NSW mental health services. In addition, the recently published RANZCP clinical practice guidelines for the management of schizophrenia and related disorders (Galletly et al., 2016) contain recommendations about the nature and frequency of monitoring for physical health disorders, including medication side effects. The RANZCP guidelines also address smoking, alcohol and substance use. These guidelines were developed by consensus of a group of Australian and New Zealand experts in the management of schizophrenia and related disorders, who reviewed the relevant evidence, including national and international guidelines, and made evidence-based recommendations. Where evidence was weak or lacking, consensus-based recommendations (CBR) were formulated.
Clinical guidelines are an increasingly familiar part of clinical practice. However, the development and publication of guidelines does not in itself ensure their use in practice and consideration must be given to dissemination and implementation (Grimshaw et al., 2004). According to the National Institute of Clinical Studies (NICS) (2006), the success of clinical guidelines in changing practice and patient outcomes depends on factors such as the methods used to develop the guidelines, the dissemination and implementation strategies used, the methods used to evaluate effectiveness, the methods used to update the guidelines and the clinical setting. As passive dissemination methods alone are less likely to lead to changes in professional behaviour, a formal structured implementation process must be developed which draws on the available evidence relating to behaviour change among health care professionals and the effectiveness of different dissemination and implementation strategies. A multifaceted strategy which is informed by available resources and perceived barriers to the management, treatment and monitoring of physical health in people with enduring psychotic illness offers the best chance of improving professional practice. The strategy needs to address organisational and individual barriers and facilitate adaptation to local settings. Powell et al. (2012) provide a typology of implementation strategies for clinical practice guidelines, which include the following strategy types: plan, educate, finance, restructure, quality management and attend to policy context. Lambert and Newcomer (2009) have also pointed to the need to overcome barriers at the service, patient and illness levels, emphasising the need for service reorganisation, communication enhancement, improved training and education, better incentives, accreditation rigour and government leadership.
Of these six strategies identified by Powell et al. (2012), the RANZCP has the clearest mandate in the area of education. This strategy should include review of the relevant sections of the registrar training programme, including the Entrustable Professional Activity (EPA) on physical comorbidity, to be consistent with the recommendations of this expert consensus statement. A further area of action would be incorporation of relevant educational activities in the Continuing Professional Development (CPD) programme. The RANZCP can also make a contribution to the strategy of ‘attend to policy context’ by advocating for changes in service delivery and resourcing which improve access to good physical health care for people with enduring psychotic illness. The use of the Delphi process with a wide array of experts has also contributed to the ‘plan’ strategy by getting preliminary buy-in from consumer and carer advocates and from key professionals outside the area of psychiatry. Future work could build on these relationships through direct contact with relevant stakeholders.
Ideally, as recommended by NICS (2006), the RANZCP should also develop an evaluation of any implementation strategies. This evaluation should assess how well the expert consensus statement is known and valued by users, the extent to which the recommendations are applied and the extent to which the application leads to improved physical health care of people with enduring psychotic illness (Burgers et al., 2005).
Consensus statement for the physical health care of people with enduring psychotic illness
Purpose
This consensus statement aims to assist health professionals to
Understand the factors that significantly increase morbidity and mortality rates in people with enduring psychotic illness,
Develop a comprehensive process for the assessment of comorbid physical health of people with enduring psychotic illness,
Facilitate the development of treatment and management plans to improve the health of people with enduring psychotic illness.
Intended audience
This expert consensus statement is for
Mental health professionals, including psychiatrists, psychiatric registrars, mental health nurses and allied health professionals working in the mental health field, i.e. occupational therapists, social workers, psychologists, pharmacists, exercise physiologists, physiotherapists, medical officers and dietitians;
Health professionals who provide health care, but are not mental health specialists;
People with enduring psychotic illness;
Families and carers of people with enduring psychotic illness.
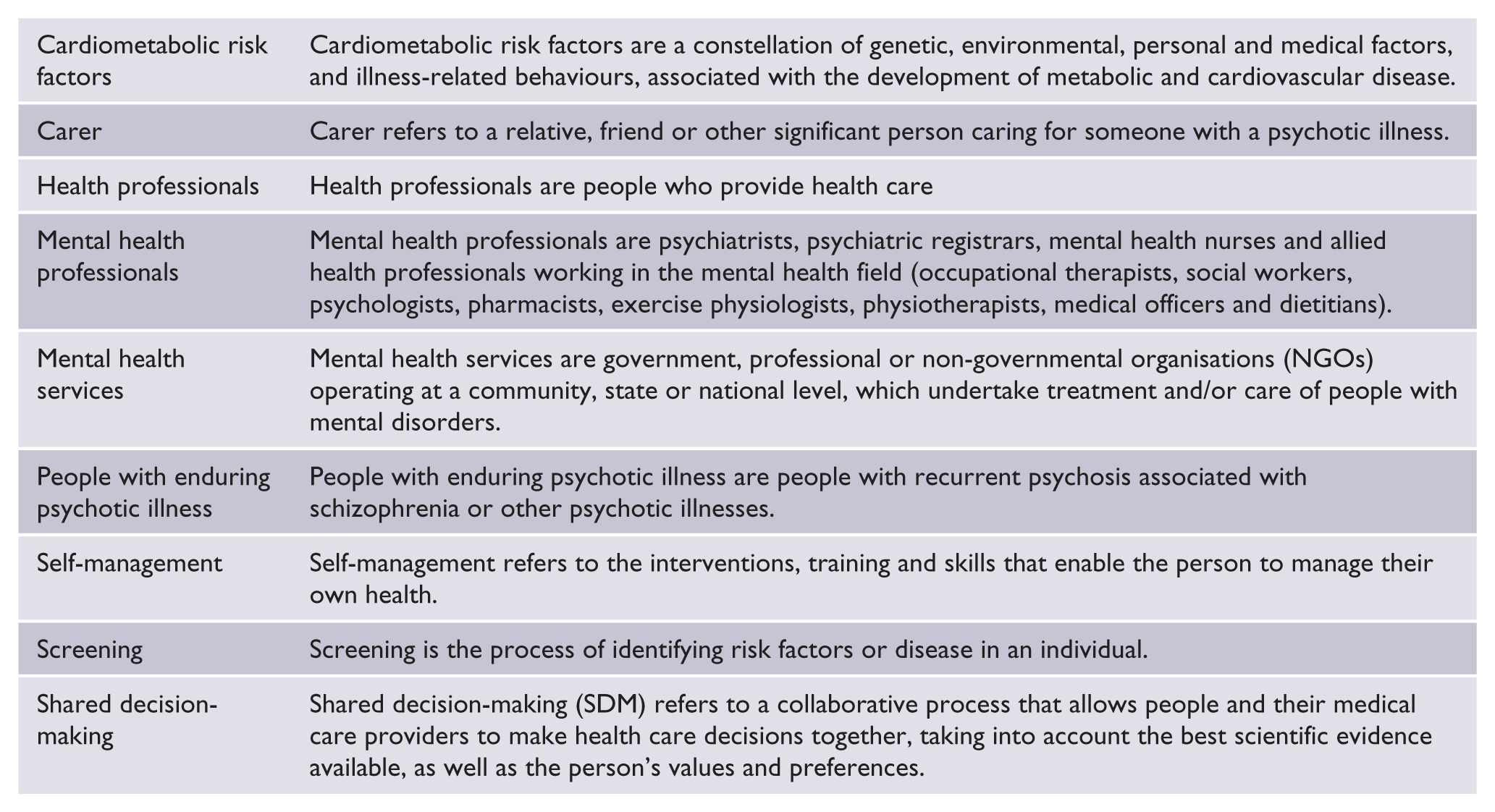
Definitions of terms
The following terms are used in the consensus statement:
Health professionals should recognise the factors affecting the health and well-being of people with enduring psychotic illness
Health of people with enduring psychotic illness
Poor physical health can exacerbate the signs and symptoms of mental illness and, along with low rates of detection, subsequent management and, critically, follow-up of physical illness, and can lead to increased rates of premature mortality in people with enduring psychotic illness. Some of the lifestyle factors that lead to the poor physical health of people with enduring psychotic illness are as follows.
Tobacco use
People with enduring psychotic illness are more likely to smoke than those without the illness, and this elevated rate has remained high even as the population level of smoking has fallen. They have limited access to any form of tobacco cessation treatment, and this represents a barrier to quitting smoking. Smoking induces particular hepatic microsomal enzymes, which increase the metabolism of selected psychotropic medications, and smokers may therefore require higher doses of some anti-psychotic medications than non-smokers to achieve similar medication effects. It should be noted that the risks of using nicotine are different to those of inhaling aryl hydrocarbons (‘tars’), which are carcinogenic.
Diet and weight
People with enduring psychotic illness are more likely to have a poor diet and be overweight or obese. All-cause morbidity and mortality is independently associated with weight gain. Additionally, the social stigma associated with weight gain may increase the risk that people with enduring psychotic illness may stop taking their medication.
Oral health
Dental health is poor in people with enduring psychotic illness. There is an association between poor oral hygiene and adverse cardiometabolic outcomes.
People with enduring psychotic illness may be unaware of their physical health problems and liabilities due to a variety of biological, social and behavioural factors such as, for example, cognitive impairment associated with their mental illness. This may impact on the person’s ability to seek help for physical health problems and/or make appropriate lifestyle changes to facilitate treatment and ongoing preventative health behaviours.
Importance of collaboration, partnership and support
Mental health services and health professionals should form collaborations with a range of services and providers
Mental health professionals should collaborate and communicate with general practitioners to develop integrated mental and physical health care plans for people with enduring psychotic illness living in the community. People with identified cardiometabolic risks should be referred to general practitioners for review, treatment and long-term follow-up in a shared-care model. A shared decision-making approach should be adopted when considering the risks and benefits of treatment of psychotic illness.
Mental health services should form strategic alliances with local non-governmental organisations (NGOs), divisions of general practice and relevant regional tertiary services with respect to physical health care management, including dentistry.
Health professionals should engage an interpreting service for people with enduring psychotic illness, or their families and carers who do not have the level of English proficiency necessary to discuss and adequately understand the implications of medical and health-related issues.
Health professionals should work in partnership with people with enduring psychotic illness, families and carers
All health professionals involved in the person’s care, the person themselves and their families and carers have a role to play in the physical health care of people with enduring psychotic illness. This role may involve
Providing practical support to enable change to a healthier lifestyle in all phases of the illness, e.g. help to get to the location of lifestyle-related programmes, working in partnership to encourage and assist the person to establish a relationship with a general or other medical practitioner and attend regular physical health check-ups.
Ensuring that the appropriate medical tests and examinations are carried out, interpreted and that appropriate action is taken. A ‘champion’ to ensure the coordination of a distributed multidisciplinary approach to these tasks is undertaken may be embedded in service roles.
Supporting the person to adhere to their treatment plans and make lifestyle changes and supporting the family to make any necessary adaptations to the family environment to facilitate these lifestyle changes
Encouraging good dental hygiene and regular check-ups.
Mental health professionals should provide support for the person with enduring psychotic illness, their families and carers to manage the person’s physical and mental health
It is important for mental health professionals to understand the support required by the families and carers to assist people with enduring psychotic illness to manage their physical and mental health. This support should include
Provision of high-quality education about physical health, lifestyle and appropriate management options, including the following information: psychotropic medications that may contribute to increasing cardiometabolic risk factors; symptoms that indicate the possibility of diabetes; importance of regular physical health checks; that smoking greatly increases the risk of cardiovascular disease and cancer; role of diet, smoking cessation and exercise in improving physical health; need to maintain regular contact with general practitioners and other health professionals involved in the person’s physical health care; importance of adherence to any agreed programme to improve physical health; provision of practical diet and nutrition skills, including planning for shopping and preparing meals; that healthy lifestyle can improve sleep, mood, levels of anxiety and general well-being; importance of social connections as a protective factor for physical health; organisation of access to free service-supported or sanctioned physical activity programmes.
All mental health service managers and health professionals should play a role
All mental health service managers and health professionals should understand their role in the screening, detection, management and follow-up of the cardiometabolic health of people with enduring psychotic illness. They should advocate for appropriate resources to undertake their role.
Role of mental health service managers
Mental health service managers should ensure that there is a sustainable screening, detection, management and follow-up system for all people with enduring psychotic illness in their service. They should evaluate the effectiveness of programmes they have set up. Mental health service managers, planners and funders should develop and implement key performance indicators (KPIs) for monitoring the care provision and physical health status of people with enduring psychotic illness.
Mental health service managers should increase mental health staff competencies in physical health screening in people with enduring psychotic illness. They should do this by
Providing inter-disciplinary training in the co-operative management of physical comorbidity,
Increasing general practitioners’ practical knowledge of severe mental illnesses and their relationship to physical comorbidities,
Providing staff who can specialise in assisting in the promotion of lifestyle changes,
Ensuring that people with enduring psychotic illness are provided with education about healthy lifestyle as a preventative measure before cardiometabolic risk increases,
Training staff in the use of motivational interviewing techniques to encourage healthy lifestyle changes,
Providing opportunities for training of families and carers.
Role of psychiatrists
Psychiatrists should be responsible for ensuring that the screening, detection, formulation and any associated follow-up procedures are carried out. This should be undertaken from the first episode of psychosis. Psychiatrists should provide clinical oversight, coordinate and ensure that the appropriate medical tests and examinations are interpreted, appropriate action is taken and a follow-up medical management plan is formulated and implemented.
Psychiatrists should ensure that every person with enduring psychotic illness being discharged from inpatient care has a comprehensive physical and mental health care plan. This health care plan should clearly delineate which health care professional is responsible for each aspect of care. The plan should be communicated to community health services, primary care providers and families and carers.
Role of mental health nurses and nurse practitioners
Mental health nurses should be trained to carry out standardised physical health interviews with people with enduring psychotic illness.
Mental health nurses should undertake the screening, detection, treatment and management, and follow-up of cardiometabolic disorders in people with enduring psychotic illness. They should measure the height, weight and waist circumference, blood pressure and random blood glucose of people with enduring psychotic illness. They should also provide education and training to mental health professionals, people with enduring psychotic illness, and their families and carers.
Advanced nurse practitioners should order appropriate metabolic screening tests for people with enduring psychotic illness.
Additional roles of health professionals and mental health professionals
Health professionals and mental health professionals should encourage people with enduring psychotic illness to participate in healthy lifestyle group activities. Individuals should be assessed and assisted to attend appropriate group-based physical activity programmes or individual physical activity programmes, depending on their need.
Role of NGOs
Where available, people with enduring psychotic illness should be referred to NGOs specialising in the rehabilitation and support of people with a mental illness to improve their lifestyle. Appropriate professionals and support workers within these services include dietitians, exercise physiologists, occupational therapists and support workers.
All health professionals should participate in the screening, detection, management and follow-up of people with enduring psychotic illness
Rationale for screening and detection
Health professionals should ensure that people with enduring psychotic illness are screened for risk factors that contribute to worsening physical health.
Cardiometabolic risks
People with enduring psychotic illness are more likely than the general population to develop impaired glucose tolerance, impaired fasting glucose and diabetes. The delayed diagnosis of and prolonged exposure to raised blood glucose levels can cause visual impairment and blindness, damage to kidneys which can lead to renal failure, foot and toe conditions related to peripheral neuropathy, cardiovascular disease, bladder and sexual dysfunction, neurological symptoms including diabetic neuropathy, and recurrent infections (especially urinary and skin).
Cancer risk
Smoking, obesity, consuming high levels of alcohol and poor diet can contribute to the risk of cancer in people with enduring psychotic illness. Risk is further increased because of the low rates of self-examination, low rates of screening, delay in diagnosis and lack of follow-up, low rates of participation in follow-up, inadequate information on family history of cancer, and medication side effects, e.g. hyperprolactinaemia.
Dental health
Dental health is also poor in people with enduring psychotic illness. They are less likely to visit a dentist or a dental hygienist, and more likely to experience problems such as a bad mouth odour; ulcerated, bleeding and/or inflamed mucous membranes, lips or gums; decayed and/or fractured teeth; calculus on teeth; and an absence of saliva. Smoking, sleep disorders, dry mouth and side effects of medication are among some of the factors contributing to the poor dental health in people with enduring psychotic illness. Their interactions promote inflammatory processes relating to cardiometabolic risk.
Osteoporosis risk
People with enduring psychotic illness are at increased risk of osteoporosis and fractures. The factors associated with this increased risk include hypogonadism (diminished functioning of the testes or ovaries), lack of weight-bearing exercise, smoking, medication side effects, alcohol and drug use, dietary vitamin and mineral deficiency, decreased exposure to sunlight and polydipsia (excessive fluid intake).
Respiratory disease risk
High rates of smoking and passive smoking in people with enduring psychotic illness contribute to increased risk of respiratory diseases such as chronic bronchitis and asthma.
Depression and anxiety risk
Physical health conditions in people with enduring psychotic illness contribute to their higher rates of depression and anxiety disorders.
Requirements for screening and detection
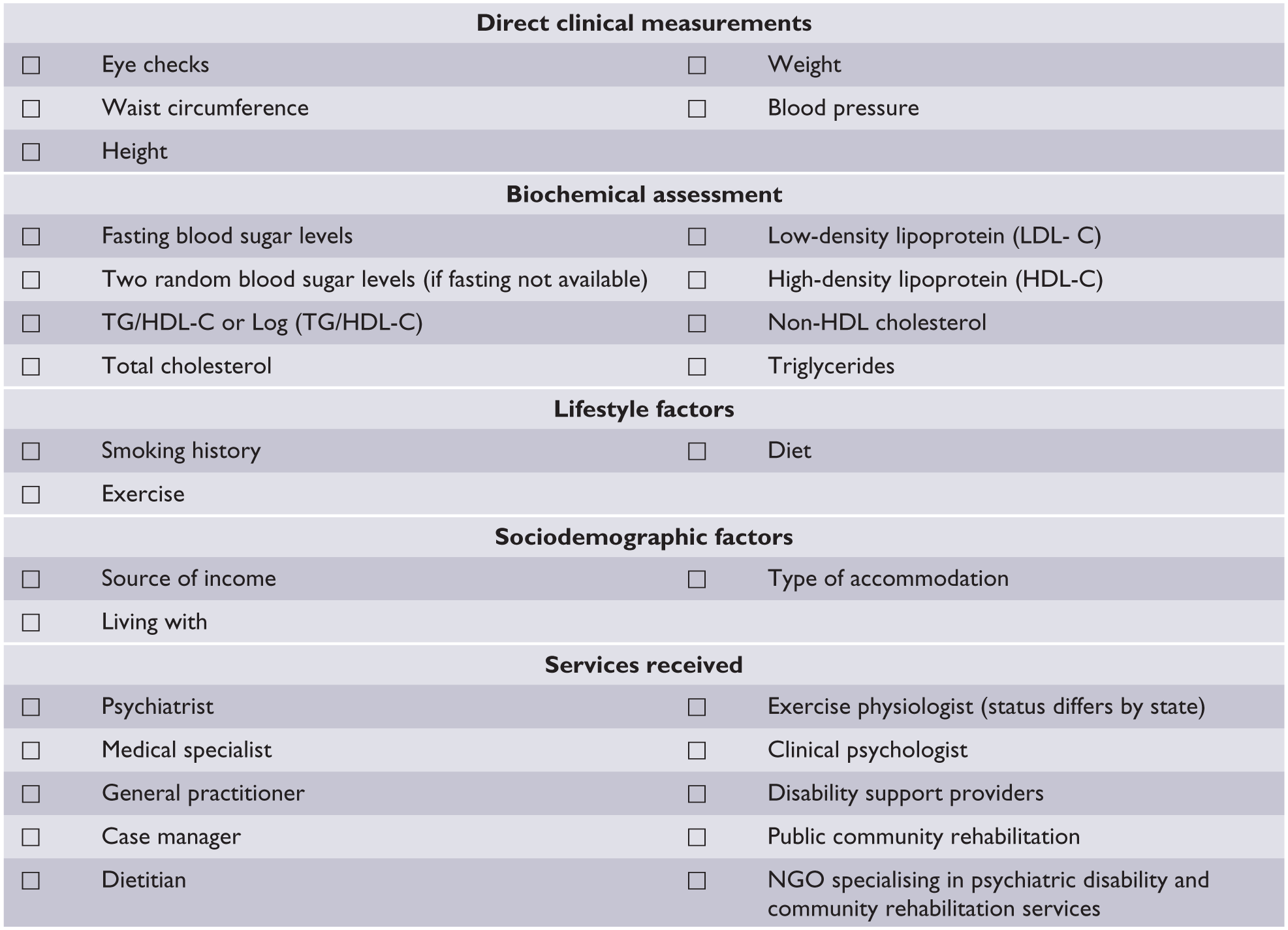
Mental health services should ensure that a comprehensive assessment of the comorbid physical health status of people with enduring psychotic illness is performed. All health professionals involved in the person’s care, the person themselves and their families and carers should play a role in ensuring that the appropriate medical tests, examinations and salient risk factors for chronic disease are interpreted and appropriate action is taken. See Figure 2 for a comprehensive initial assessment checklist.
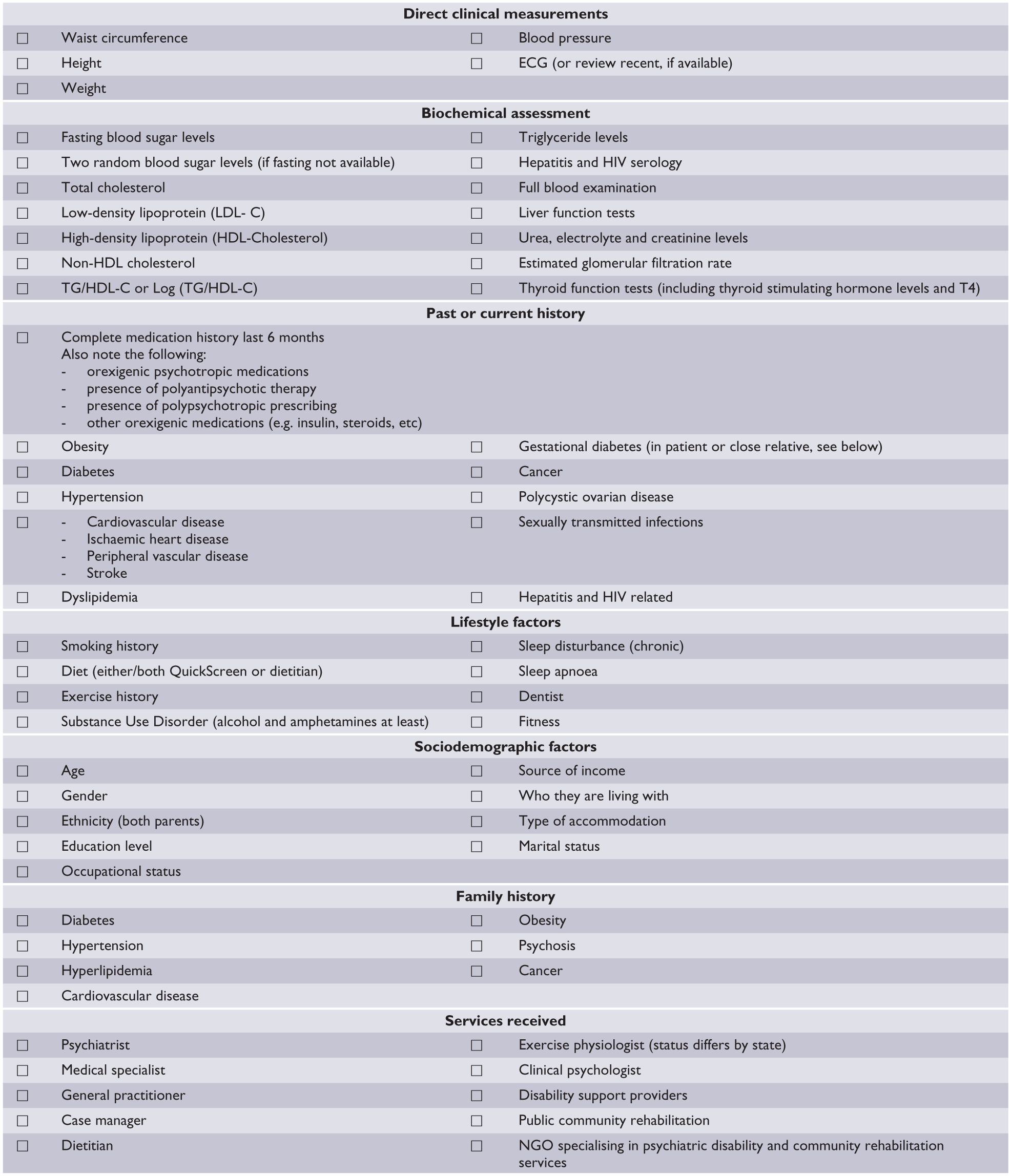
Initial assessment checklist.
Mental health services should provide a suitable room for the physical examination and ensure that it is equipped with the following: tape measures, digital scales, height measures (calibrated rigid stadiometer), glucometer and accessories, stethoscope, sphygmomanometer, urine analysis kit (dip stick type to check for microscopic haematuria, proteinuria and infection), hand washing facility, disposable/surgical gloves, appropriate bio-hazard disposable units, privacy gowns and drapes, access to pathology order forms and online results, and a chaperone (available as appropriate or on request). See Figure 3 for a checklist for physical examination room equipment.
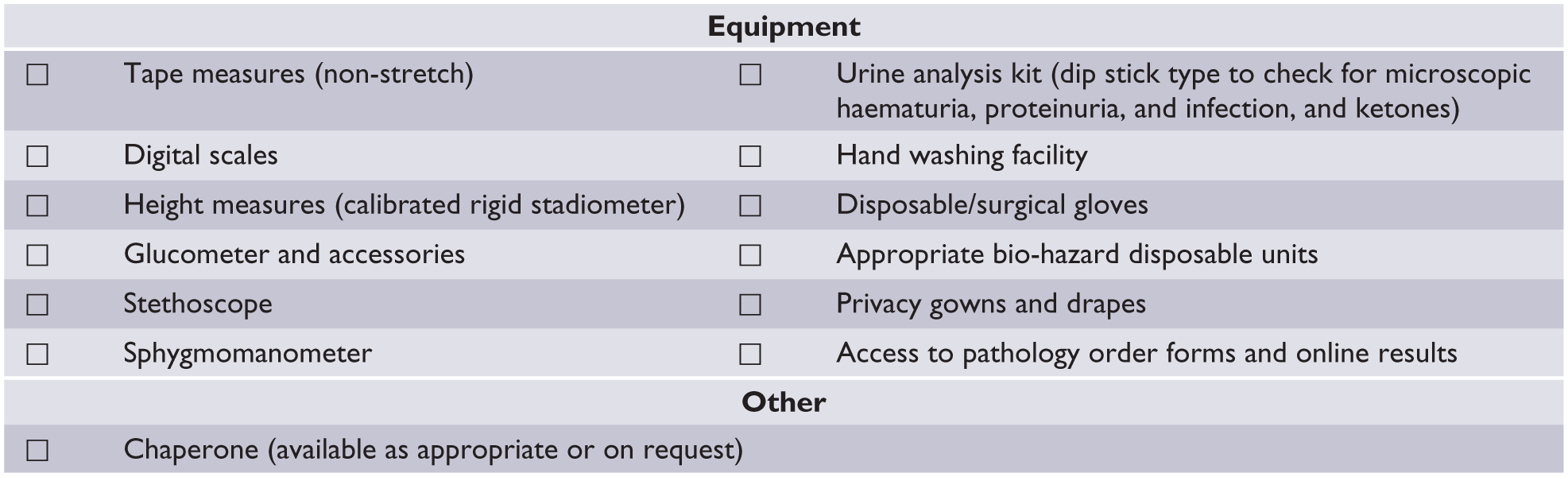
Checklist for equipment and support for physical examination.
The initial assessment should include the following measurements: waist circumference, height and weight. Biochemical investigations should include fasting blood sugar levels (BSLs), two random BSLs (if fasting not available), total cholesterol count, LDL-C, high-density lipoprotein cholesterol (HDL-C), TG/HDL-C or log (TG/HDL-C), non-HDL-C, TG levels, hepatitis serology, full blood examination, liver function tests, urea, electrolyte and creatinine levels, estimated glomerular filtration rate, haematuria, proteinuria and thyroid function tests (including thyroid stimulating hormone [TSH] and free T4).
Because a significant proportion of people with enduring psychotic illness have experienced trauma, this needs to be considered when taking the medical history, undertaking physical examinations and investigations.
The initial assessment should also cover
Socio-demographic factors, including age, gender, ethnicity, type of accommodation, education level, socioeconomic adversity, rurality, marital status, occupational status, source of income and who they are living with;
Family history of diabetes, hypertension, hyperlipidaemia, cardiovascular disease, stroke and cancer;
Personal history of smoking, alcohol and other substance use, physical activity, diet and sleep hygiene;
History of or treatment for obesity, diabetes, gestational diabetes, cardiovascular disease, stroke, hyperglycaemia, hyperlipidaemia, hypertension, cancer, polycystic ovarian disease, sleep disturbance (chronic), sleep apnoea, constipation and sexually transmitted infections;
Whether the person is receiving services from any of the following: psychiatrist, medical specialist, general practitioner, case manager, dietitian, clinical psychologist, exercise physiologist, disability support, public community rehabilitation, NGO specialising in psychiatric disability and community rehabilitation service;
Dental hygiene and dry mouth.
Development of a management plan
Psychiatrists should ensure that a comprehensive management plan is developed based on the results of the initial assessment. The following people should play a role in ensuring that an appropriate medical management plan is implemented: psychiatrist, general practitioner, registrar, nurse, case manager, people with enduring psychotic illness and their families and carers.
Psychiatrists should ensure that all the screening information is used to formulate a cardiometabolic risk profile at initial assessment and prior to starting or changing psychotropic medications. Psychiatrists should inform and discuss the person’s cardiometabolic risks with them, their families and carers.
Psychiatrists should ensure that there is an appropriate medical treatment plan for standard cardiometabolic risks such as dyslipidaemia, dysglycaemia, hypertension and obesity. These treatment plans should follow standard guidelines.
A comprehensive management should also include
An annual dental assessment;
Dietary intervention in accordance with relevant guidelines;
Physical activity intervention in accordance with relevant guidelines;
Provision of an individually tailored smoking cessation programme, including nicotine replacement therapies at no cost, and referral to smoking cessation services;
Sleep assessment, including obstructive sleep apnoea;
Promotion of social connections, e.g. through group activities.
Medication side effects
Psychotropic medications may contribute to cardiometabolic risk factors. People with enduring psychotic illness and their families or carers should be informed about the range of cardiometabolic risks associated with the psychotropic medications they have been recommended. If the person develops cardiometabolic risk factors after the initiation of psychotropic medications, the psychiatrist should review the medications and consider less risky alternatives. Poly-antipsychotic prescribing and polypharmacy in general should be carefully scrutinised, and where appropriate, a de-prescribing strategy should be formulated. They should also assertively manage any medical comorbidity that arises as a side effect of treatment.
Health professionals should be aware of the specific physical health side effects of clozapine. They should also monitor the side effects of any psychotropic medications that may impair the ability to operate machinery, including driving vehicles.
Follow-up assessments
Psychiatrists should ensure that follow-up assessments are carried out every 3–6 months and at any change of psychotropic medications, or when the person presents with new signs and symptoms relating to cardiometabolic risks.
The follow-up assessment should include all the factors assessed at initial assessment. If the person has a history of, or is receiving treatment for, any chronic disease, then the follow-up assessments should identify the services they are receiving (see Figure 4 for a follow-up assessment checklist).
Follow-up assessment checklist.
Service managers and clinical leaders should develop policies and procedures for integrated care
Mental health service managers should work with senior clinical leaders to develop integrated clinical care policies and procedures that are directed specifically towards the physical health needs of people with enduring psychotic illness. They should ensure that standardised procedures for assessing cardiometabolic risk factors are used. They should also develop policies and procedures to enable the relay of clinical information between mental and physical health service providers.
Mental health service managers should ensure that quality improvement activities specifically evaluate the effectiveness of integrated physical and mental health care.
The RANZCP and other relevant Colleges should advocate for the inclusion of people with enduring psychotic illness as high-risk patients in the formulation of companion guidelines by other professional bodies, e.g. cardiology and endocrinology.
Footnotes
Acknowledgements
We would like to thank the panel members for their contribution to the development of the expert consensus statement. We would also like to thank Dr Huseyin Mustafa, Rajneet Arora, Joyce Goh, Shuli Rawson and Edwina Ward for their assistance.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Oakley Browne was, until recently, employed as Chief Psychiatrist with the Victorian Government Department of Health. He is currently Chair of the Committee for Therapeutic Interventions and Evidence-based Practice of the Royal Australian and New Zealand College of Psychiatrists (RANZCP). Tim Lambert is Director of the Collaborative Centre for Cardiometabolic Health in Psychosis (ccCHiP), a multidisciplinary, inter-professional clinical, research and training service supported by Sydney Local Health District and Sydney University/Charles Perkins Centre. Anthony Jorm and Nicola Reavley receive salary support from the National Health and Medical Research Council (NHMRC).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.