
Abstract

To the Editor
Multiple sclerosis (MS) and intracranial space-occupying lesions can produce psychiatric manifestations, particularly mood disorders. Treatment of the latter with electroconvulsive therapy (ECT) in patients with MS and intracranial space-occupying lesions has been described, and while neurological deterioration is a risk during active demyelination, this is uncommon (Palm et al., 2014). The incidence of spontaneous seizures following ECT in patients with MS or space-occupying lesions also appears to be rare, with only two reported cases (Fried and Mann, 1988; Urban-Kowalczyk et al., 2014). We discuss a 49-year-old woman with rapid-cycling bipolar affective disorder, two meningiomas and relapsing–remitting MS (treated with dimethyl fumarate) who had previously responded to ECT. She had no clinical/radiographic evidence of active demyelination or mass effect and no history of seizures (Figure 1).
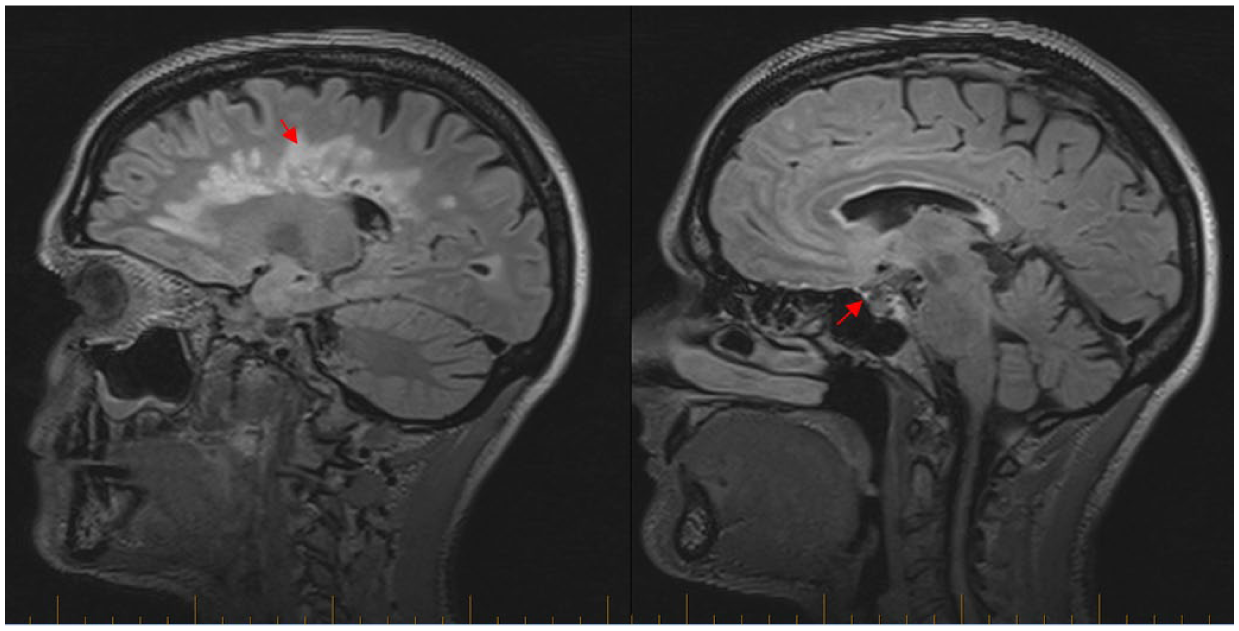
MRI showed stable areas of hyperintensity affecting supratentorial white matter, corpus callosum, pons, right cerebellar hemisphere and thoracic spinal cord. There were two meningiomas: one involving the right greater wing of the sphenoid extending into the cavernous sinus, pituitary fossa and foramen ovale; the second involving the lateral aspect of the Sylvian fissure.
The patient was admitted in a depressive state and, to reduce rapid-cycling, her anti-depressant medications (nortryptyline and escitalopram) were ceased. However, an affective switch emerged that was complicated by transient delirium. Olanzapine and lithium were administered with good effect. She was discharged upon resolution of her symptoms, but readmitted with depression within 1 week.
The patient was prescribed a course of right-unilateral ultra-brief ECT. Seizure threshold was found at 19mC. She did not receive a suprathreshold dose, and there was no clear seizure endpoint on electroencephalography. Twenty minutes after the ECT stimulus, the patient experienced a generalized tonic–clonic seizure requiring pharmacological termination. ECT was discontinued and her pharmacological management was optimized with lithium and lamotrigine. As she neared euthymia, she was discharged.
Urban-Kowalczyk et al. (2014) highlight the difficulty in determining whether post-ECT seizure in a patient with MS is a rare complication of ECT or a component of MS itself. They suggest the latter is more likely, given seizures are known complications of MS, and ECT theoretically raises seizure threshold. Alternatively, this patient may have experienced continued epileptic activity following ECT that culminated in a generalized seizure. Meningioma is a less likely cause in this instance given the lack of a mass effect. Another possibility is an undiagnosed propensity to seizures given the history of delirium, which retrospectively may have been seizure related. Olanzapine, which reduces seizure threshold, may have unmasked this propensity. Current literature indicates ECT can be used safely in MS (Palm et al., 2014); however, this case illustrates a rare but significant adverse event without a clear mechanism, highlighting the need for greater understanding of the relationship between ECT, MS and space-occupying lesions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.