
Abstract
Objective:
Although there is clear evidence that reproductive cycle events are associated with mood episodes for women with bipolar disorder, few studies have examined for relationships between these and specific clinical characteristics of the disorder. This study aimed to explore the relationship between mood symptoms associated with reproductive cycle events and features of the disorder indicative of a more severe lifetime course.
Method:
Totally, 158 women of at least 18 years of age participated in the study. Subjects were recruited through a specialist clinic at the Black Dog Institute, Sydney, Australia.
Results:
In total, 77% of women reported increases in mood symptoms during perimenstrual, postnatal or menopausal periods. These women had an earlier age of onset for depressive and hypo/manic episodes and a greater likelihood of comorbid anxiety disorders, rapid cycling and mixed mood compared to those who did not report such reproductive cycle–associated mood changes. Women who experienced postnatal episodes were also more likely to experience worse mood symptoms perimenstrually and menopausally.
Conclusion:
First, reproductive cycle event–related worsening of mood was associated with a more severe lifetime course of bipolar disorder, and, second, it appears that some women have a greater propensity to mood worsening at each of these reproductive cycle events. If replicated, these findings provide important information for clinicians treating women with reproductive cycle event mood changes and highlight the need for improved therapeutics for such presentations.
Introduction
Although the prevalence of bipolar disorder (BD) is similar among men and women, some gender-related differences have been found in clinical features of the disorder (Arnold, 2003). Rapid cycling (Erol et al., 2015; Robb et al., 1998), mixed episodes, depressive episodes and increasing symptom severity over the illness course have been reported to be more frequent in women (Barnes and Mitchell, 2005). Some anxiety disorders, such as panic disorder, may also be more common in women with BD than men (Saunders et al., 2012).
Reproductive cycle events, i.e., the menstrual cycle, pregnancy/postnatal period and menopause, may impact the course of the illness for women with BD. Some authorities have suggested that the interaction between oestrogen, progesterone, brain-derived neurotrophic factor, oxidative stress and inflammation pathways may be particularly relevant for women with BD, with this being a potential mechanism for increased risk of relapse (Frey and Dias, 2014).
The pre- and postnatal period is a well-documented time for increased risk of recurrence for women with BD, with about 45% of women reporting mood disturbances during pregnancy or within 1 month of giving birth (Blehar et al., 1998). A recent meta-analysis of 37 studies investigating the risk of postpartum recurrence in women with BD found an overall risk of 35% (Wesseloo et al., 2015). Although depression is the most commonly reported symptom pre- and postnatally, an eightfold increase in the risk of elevated mood in the week postpartum has been found (Heron et al., 2009).
Some studies have examined the impact of the menstrual cycle on mood symptoms, with 66% of women with bipolar I disorder (BD I) reporting significant mood changes during the menstrual or premenstrual phase (Blehar et al., 1998). A recent review of the literature noted that, of those studies which were prospective, 44–65% of women reported mood changes during the premenstrual phase (Teatero et al., 2014).
An analysis of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) data over a 1-year follow-up period found that those women (with either BD I or BD II) who reported premenstrual exacerbation had greater overall symptom severity and a worse course of illness (Dias et al., 2011). Other studies have also noted that a premenstrual syndrome was more commonly reported by women with BD II than those without BD (Cirillo et al., 2012). Inconsistent results have been found for women with rapid-cycling BD, with one study finding them to have more severe premenstrual symptoms than controls (Price and DiMarzio, 1986), but another study using mood charting techniques over a month-long period reporting no influence of the menstrual cycle on mood (Leibenluft et al., 1999).
It has been noted that about 20% of women with BD report emotional disturbances during the menopause transition period (Blehar et al., 1998). The only prospective study that has examined this (studying 56 women with BD) found that women reported more mood symptoms, and a greater severity of symptoms, during the menopause transition period than at other times (Marsh et al., 2015).
Other studies have also explored mood symptoms in BD and their relationship to reproductive cycle events. In a sample of 50 women with BD, Freeman et al. (2002) reported that 20 of 30 women who had given birth experienced a postpartum mood episode. In additional analyses, they found no impact of contraceptive use or hormone replacement therapy on mood symptoms. Totally, 12 women reported worsening of mood during menopause and 10 reported no change in mood symptoms.
Payne et al. (2007) examined mood events during the menstrual cycle, postnatal period and perimenopause in a large sample (n = 197) of women with BD. Although they found no significant association between these and mood symptoms during other reproductive cycle events for those with BD I, women with BD reported higher rates of premenstrual mood symptoms (70%) compared to controls (30%) (Payne et al., 2007).
In summary, while these studies highlight important associations between reproductive cycle events and BD, potential links between these mood changes and other clinical features of BD remain largely unexplored.
This study aimed to explore the relationship between mood changes associated with reproductive cycle events and clinical features indicative of a greater severity of illness, such as BD subtype, psychiatric co-morbidities (specifically anxiety and substance use disorders), age of onset of mood episodes, number of lifetime episodes, hospitalisations, family history of BD, rapid cycling, self-harm and suicide attempts. It was hypothesised that women who report mood disturbances associated with reproductive cycle events would be more likely to endorse items indicating greater illness severity.
Methods
Participants
Subjects were women aged 18 years and older with Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) BD I or BD II who were recruited through the Bipolar Disorders Clinic (a specialised outpatient tertiary referral service) at the Black Dog Institute, Sydney, Australia. This study was approved by University of New South Wales Human Research Ethics Committee (HREC 09394). All subjects provided written informed consent.
Procedure and measures
Participants attended the clinic for face-to-face interviews with both a trained researcher and a qualified psychiatrist. The Structured Clinical Interview for the DSM-IV-TR Axis I Disorders (SCID-I) (First et al., 2002) was administered by the researcher to confirm a DSM-IV diagnosis of BD. The SCID-I is an interview schedule that assesses domains of BD – major depression, hypo/mania and psychosis. A kappa value of 0.74 has been reported for DSM-IV criteria for BD (Gunderson et al., 2006). After this interview was completed, the participant was then administered a structured questionnaire that was developed by the study investigators (Mitchell et al., 2009), which included questions on symptom course and severity including frequency and duration of episodes, age of onset, mixed episodes, rapid cycling, suicidal acts and details about hospitalisations for BD. At the end of the interview, participants completed a self-report Composite International Diagnostic Interview (CIDI-AUTO) via computer (World Health Organization [WHO], 1997). Modules administered included lifetime occurrence of simple phobia, generalised anxiety disorder, panic disorder, social phobia and agoraphobia along with substance abuse/dependence.
Prior to attending the clinic, subjects were asked to complete a self-report questionnaire of measures including demographic variables and details about reproductive cycle events and their impact on mood. These included questions about prior pregnancies, contraceptive use, perimenstrual (‘just before or during menstrual periods’) symptoms and menopausal status. Specifically, participants were asked to endorse whether they had noted increased or decreased mood symptoms as a result of contraceptive use, during the perimenstrual phase, during menopause and after commencing hormone replacement therapy. For the postnatal period, participants were asked to endorse whether they had an episode within 4 weeks after giving birth and how many of these were depressive or hypo/manic.
Statistical analysis
First, to explore the associations between increased mood symptoms and categorical BD illness characteristics, chi-square analyses were performed on type of BD (I or II), anxiety disorder (yes/no), drug and alcohol abuse or dependence (yes/no), BD-related hospitalisation (yes/no), mixed episodes (yes/no), rapid cycling (yes/no) or episodes of self-harm (yes/no). Second, to explore the associations between new or increased mood symptoms and dimensional BD illness characteristics, multiple analyses of covariance (ANCOVAs) controlling for age were conducted on number of lifetime prior episodes, number of hospitalisations, age of onset (for hypo/mania and depression) and number of episodes of self-harm.
Results
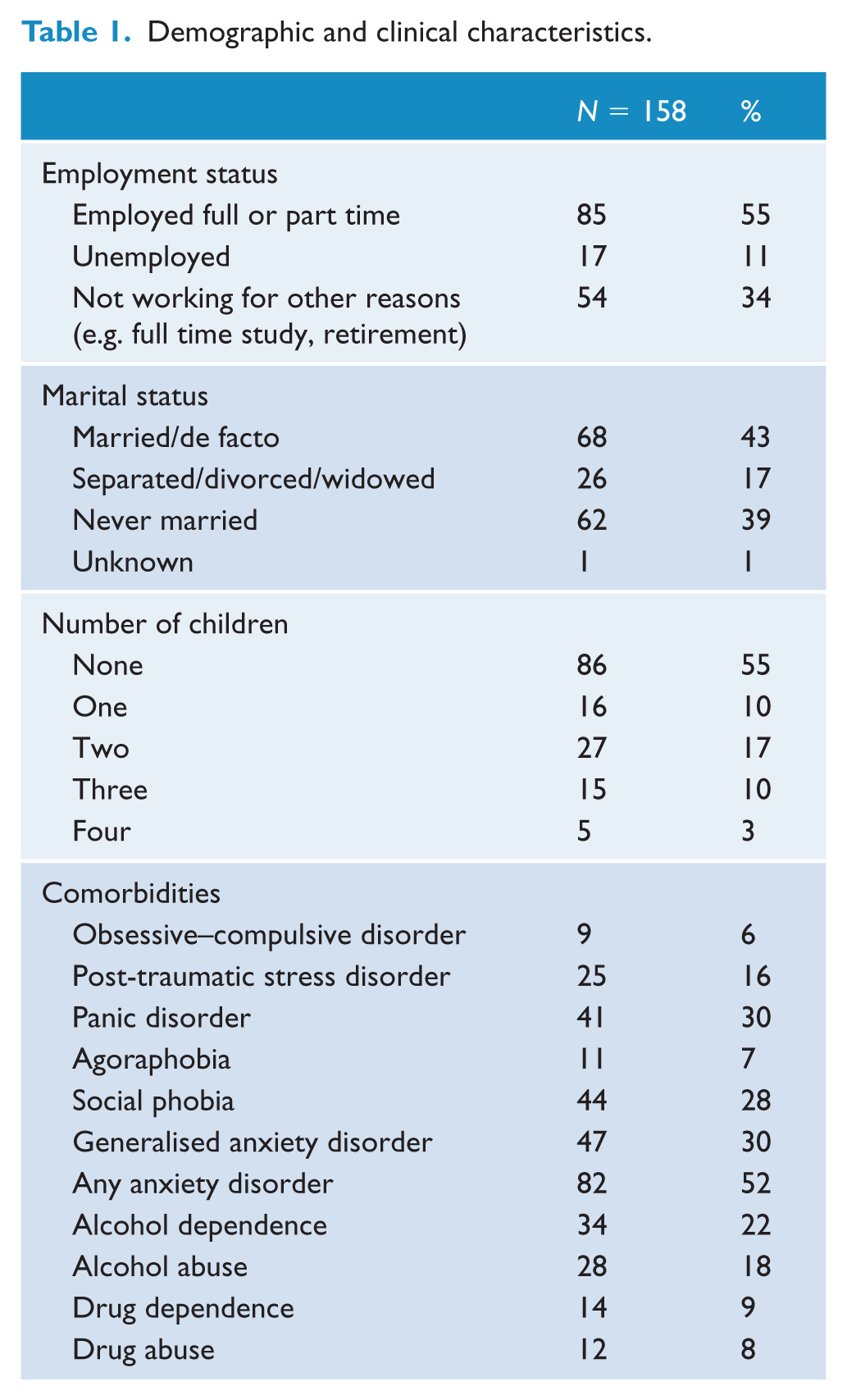
In total, 158 women participated in the study with 108 (68%) being diagnosed with BD I and 50 (32%) with BD II. Their mean age was 37.89 years (standard deviation [SD]: 13.60; range: 19–76 years). About 114 (72%) were born in Australia, with 138 (87%) currently taking antidepressants, antipsychotics or mood stabilisers. Totally, 63 (40%) women had at least one child and 38 (24%) reported having started or transitioned through menopause. Further demographic characteristics of the sample are presented in Table 1. In total, 56 (35%) participants met criteria for a current major depressive episode, 6 (4%) for a current manic episode and 21 (13%) for a current hypo/manic episode as assessed by the Structured Clinical Interview for the DSM-IV (SCID).
Demographic and clinical characteristics.
Any reproductive cycle event–related mood symptoms
Overall, 93 (77%) participants reported having experienced worsening of mood at perimenstrual, postnatal or menopause time periods (see Table 2). Details are outlined below in the specific reproductive cycle event sections.
Reproductive cycle event and contraceptive-associated mood symptom characteristics. a
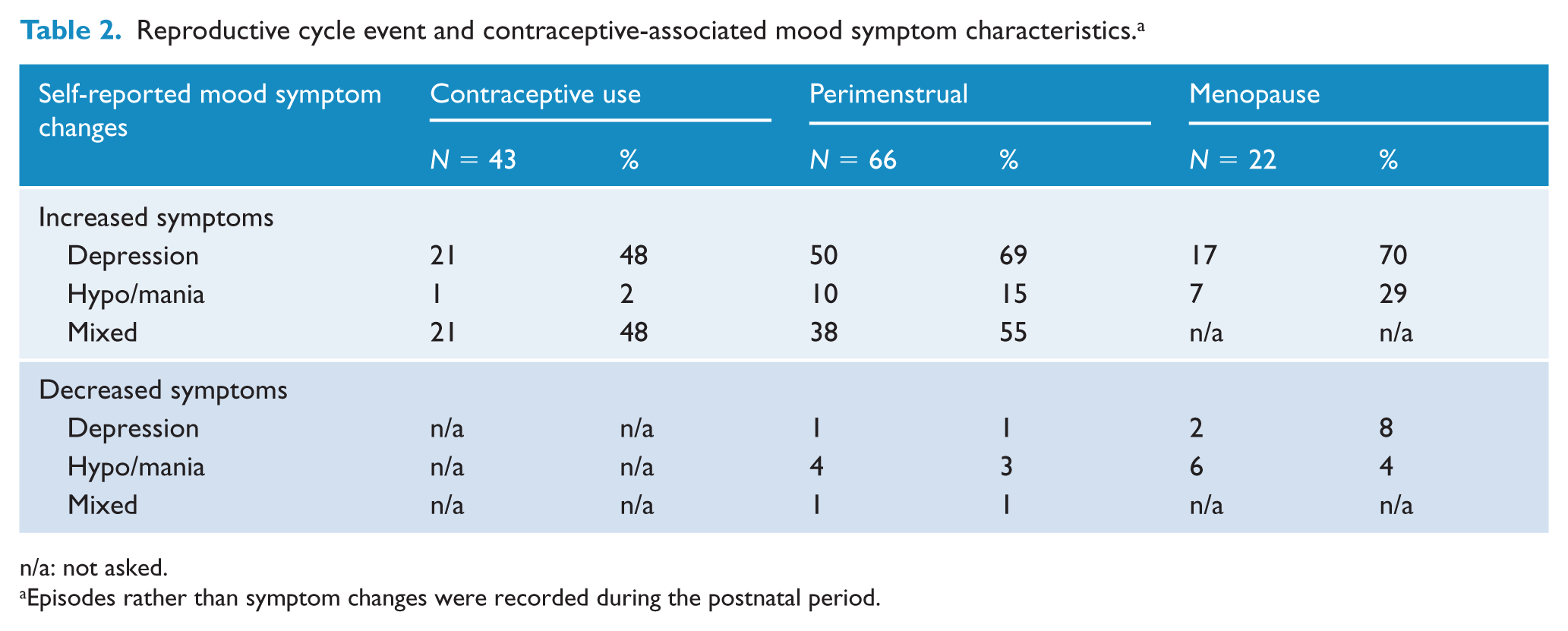
n/a: not asked.
Episodes rather than symptom changes were recorded during the postnatal period.
Women who endorsed worsening mood at any reproductive cycle event were more likely to report a history of mixed mood, self-harm, rapid cycling and an anxiety disorder compared to those who did not report any worsening mood at these points. Significant findings and strong statistical trends are detailed in Tables 3 and 4. The age of onset of the first depressive episode was significantly associated with the endorsement of any reproductive cycle event–related symptom increases, with a younger age of onset being reported by those who endorsed such mood changes. The age of onset of the first hypo/manic episode was also significantly associated with the endorsement of such symptoms with a younger age of onset being associated with these (see Table 4).
Associations between reproductive cycle event mood worsening and illness characteristics: significant and trend chi-square results.
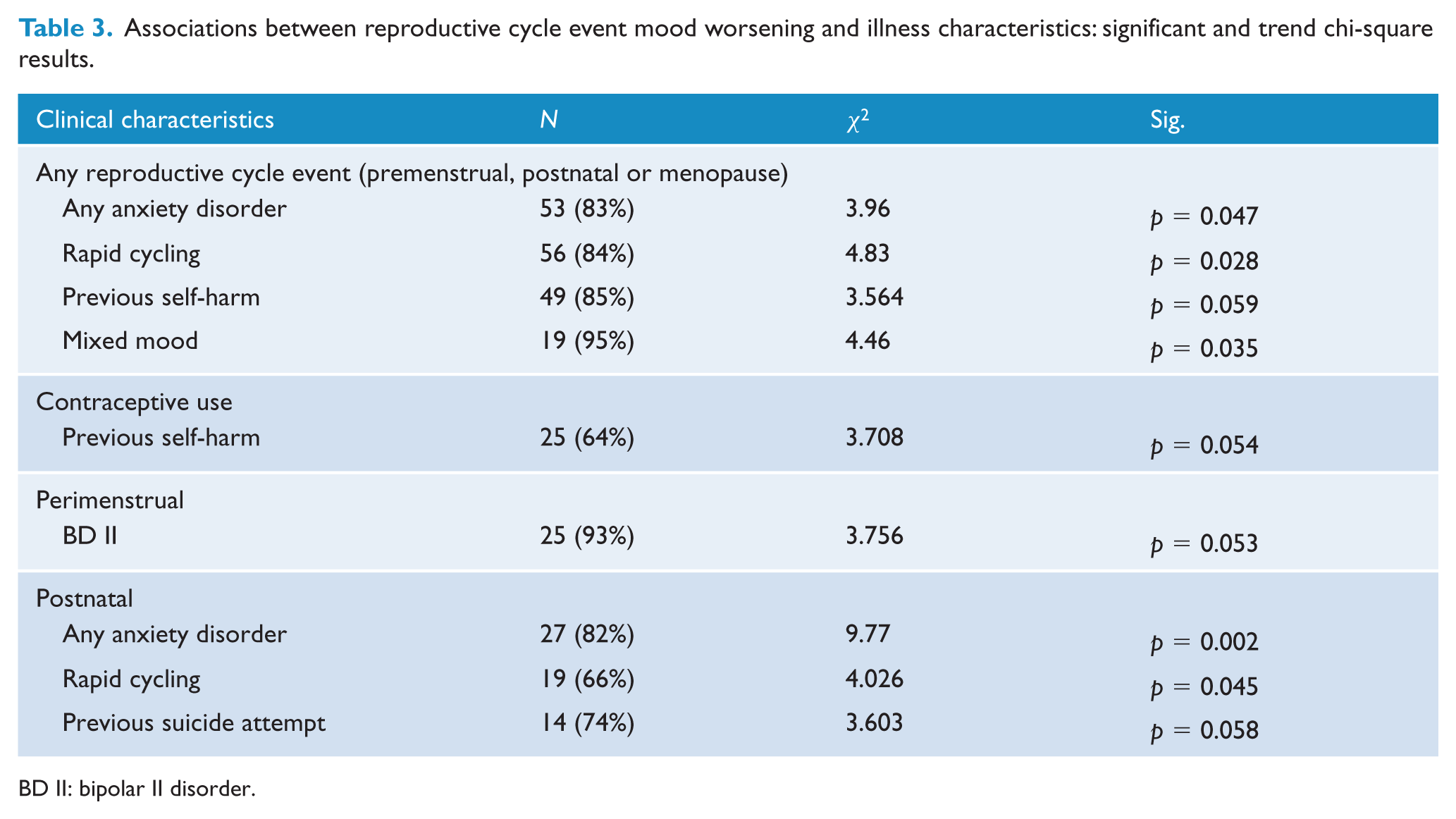
BD II: bipolar II disorder.
Significant ANCOVA results.
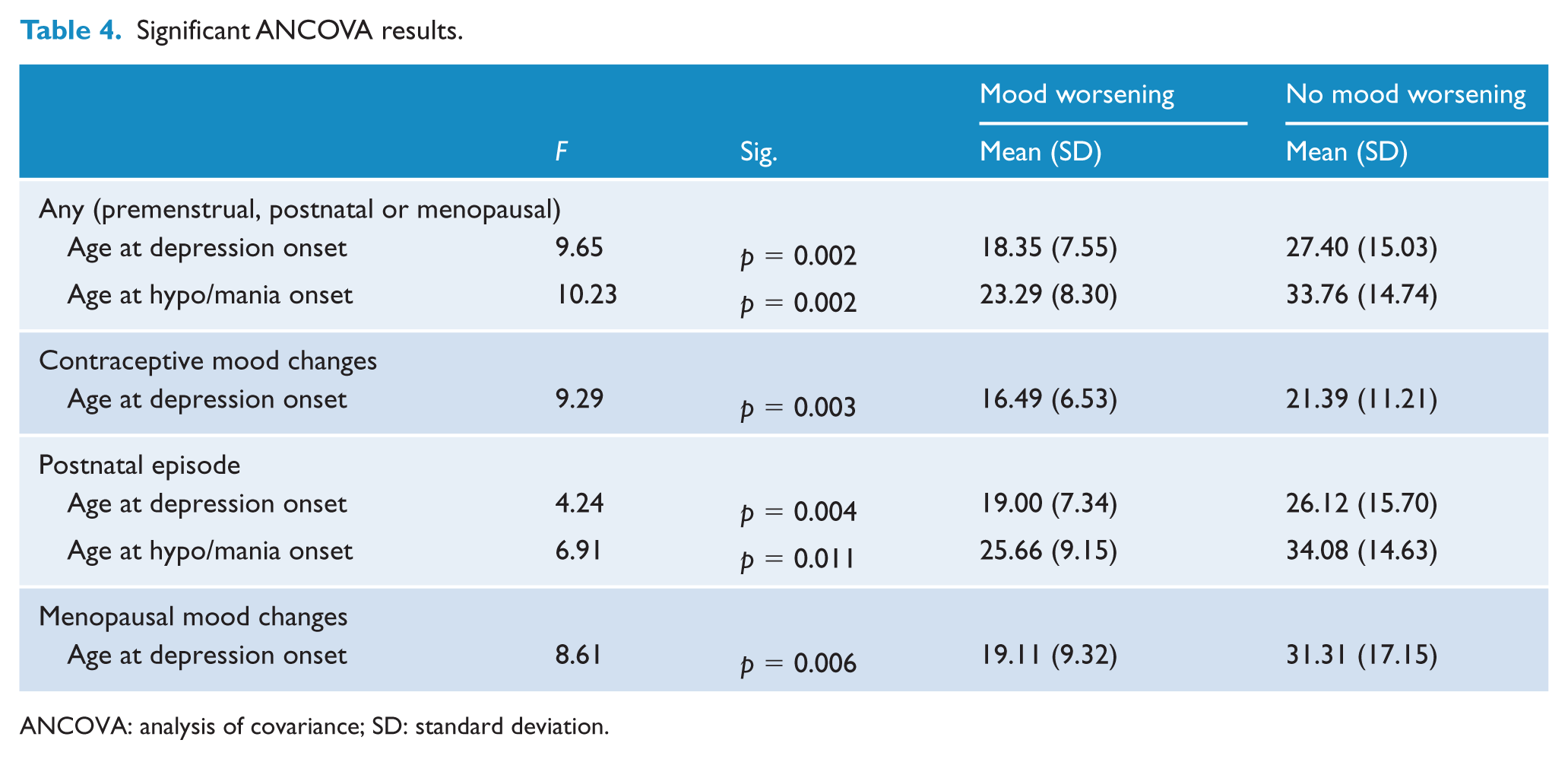
ANCOVA: analysis of covariance; SD: standard deviation.
Contraceptive use
Totally, 124 women (79%) reported lifetime contraceptive use. Of these, 43 (35%) reported worsening mood symptoms during contraceptive use, with the vast majority experiencing either depressive or mixed symptoms (see Table 2). There were no significant associations on chi-square analyses, however, a trend was noted for a history of self-harm, with those who reported mood changes also being more likely to have self-harmed previously (χ 2 = 3.71, p = 0.053). ANCOVAs demonstrated that those who endorsed mood worsening were significantly more likely to report an earlier age of onset for depression compared to those who did not experience mood worsening (Table 4).
Perimenstrual
In total, 66 women (42%) reported mood worsening before or during their menstrual cycle (Table 2). Chi-square analyses were not significant; however, a trend for women who endorsed perimenstrual mood changes was found with those who endorsed these mood changes more likely to be diagnosed with BD II. ANCOVAs revealed no significant findings.
Postnatal
Totally, 34 (55%) of the 61 women who had given birth reported a mood episode within 4 weeks of childbirth. Twenty-eight (93%) reported one or more episodes of postnatal depression with the mean number of episodes being 1.80 (SD = 1.16; range: 0–5). Nine (32%) reported hypo/manic episodes after childbirth with the mean number of hypo/manic episodes being 1.67 (SD = 1.41; range: 1–5). Eight (31%) women reported having experienced both a hypo/manic and a depressive episode after birth.
For the chi-square analyses, women who had experienced any postnatal mood episode (depression and/or hypo/mania) were more likely to endorse an anxiety disorder, rapid cycling and a previous suicide attempt (Table 3). For the ANCOVAs, age of onset for the first depressive episode was significantly associated with the endorsement of postnatal episodes (see Table 4), with a younger age of onset being reported by those who had experienced a postnatal episode. Age of onset for first hypo/manic episode was also significantly associated with the endorsement of a postnatal episode (see Table 4), with a younger age of onset being reported by those who had experienced a postnatal episode.
Menopause
Totally, 22 (58%) of the 38 women in the sample who had started or transitioned through the menopause reported new or worse symptoms at that time. The mean age of commencing menopause was 46.4 years (SD: 6.30; range: 22 –55 years). Fifteen (33%) reported taking hormone replacement therapy (HRT) with seven (47%) describing mood changes as a result. Two participants reported decreasing symptoms and symptom severity (one reported this for both depression and hypo/mania, and the other reported depression improvements only).
There were no significant associations on chi-square testing. The age of onset for the first depressive episode was significantly associated with endorsement of menopause-related mood symptoms, with a younger age of onset being reported by those who endorsed these mood changes (see Table 4). No other results were significant.
Associations between risk of postnatal episodes and perimenstrual or menopausal mood symptoms
Chi-square analyses were conducted to examine possible associations between postnatal episodes and both perimenstrual and menopausal mood symptoms, respectively. First, of the 18 women who reported postnatal episodes (depression and/or hypo/mania), 15 (83%) also reported perimenstrual mood symptoms (χ 2 = 4.07, p = 0.044). Second, of the 17 women who had menopause-related mood symptoms and had given birth, 12 had reported prior postnatal mood episodes (χ 2 = 9.26, p = 0.002).
Discussion
While prior studies have affirmed strong associations between reproductive cycle events and worsening of symptoms in BD, potential links between these mood changes and other clinical features of BD have remained largely unexplored. In this study, we examined for associations between propensity for mood worsening with such events and indices of a greater illness severity.
First, we found that lifetime histories of comorbid anxiety disorders, rapid cycling and mixed mood presentations were significantly more prevalent in women who reported perimenstrual, postnatal or menopause-related mood symptoms (with trends towards increased rates of prior self-harm and suicide attempts). Second, the ages of onset for both first depressive and hypo/manic episodes were earlier for women who endorsed any reproductive cycle mood changes. All of these novel associations are suggestive of a more severe lifetime disorder in those with reproductive cycle event–related mood symptoms.
Consistent with prior reports, this study found high rates of reproductive cycle–related mood symptoms, with 77% of the sample reporting worsening of mood symptoms related to at least one of the reproductive cycle events examined, i.e., perimenstrual, postnatal or menopausal. This is in line with recent findings in the postnatal period (Wesseloo et al., 2015) and menopause (Marsh et al., 2015).
Interestingly, there were significantly increased risks of women experiencing new or worsened mood symptoms at multiple reproductive cycle events. Specifically, we found that women who experienced postnatal episodes were also more likely to experience worse mood symptoms perimenstrually and menopausally, suggesting that some women have a greater propensity to mood worsening at each of these reproductive cycle events. In the only other study of which we are aware that has addressed this issue, Payne et al. (2007) found no association between mood changes at these different events.
The impact of contraceptive use on BD symptoms has been minimally researched. In contrast to Freeman et al. (2002) who found no impact of contraceptive use on mood symptoms, in our study about one-third of women with BD reported mood worsening as a result of contraceptives, with a large percentage reporting both ‘mixed’ and ‘depressive’ symptoms.
This study was cross-sectional, with the inherent potential for errors in retrospective recall. It is clear that further work using a prospective design examining this area is needed. Furthermore, the sample size of the menopausal group was small with only 38 subjects. Other limitations were the self-report nature of the retrospective mood symptom data and the lack of biological measures such as fluctuations in reproductive cycle hormones.
Conclusion
Mood changes related to reproductive cycle events were strongly associated with indices of a more severe lifetime illness course for women with BD, i.e., earlier age of onset for both depressive and hypo/manic episodes, comorbid anxiety disorders, rapid cycling and mixed mood presentations (and a trend towards higher rates of prior self-harm and suicide attempts). Furthermore, women who experienced mood worsening at one reproductive cycle event were more likely to experience such symptoms at other events. If replicated, these findings provide important information for clinicians treating women with reproductive cycle event mood changes and may be an important clinical indicator of risk. It also highlights the need for improved therapeutics for such presentations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded by the Australian National Health and Medical Research Council Program Grant No. 1037196.