
Abstract

Schneiderian first-rank symptoms (FRS) indicate a clinical presentation where there is significant disturbance in the recognition of oneself as a unique, discrete entity, capable of autonomous action and perception. The first description of FRS was coined by Kurt Schneider (1939), where he later expounded that FRS – characterised by a loss of self coupled with perceived control by external forces – were of key clinical significance in determining a diagnosis of schizophrenia. His aim was to distinguish schizophrenia from other forms of psychoses, especially affective psychoses. The Diagnostic and Statistical Manual of Mental Disorders (DSM) bestowed considerable weighting to FRS in earlier editions in deciding a diagnosis of schizophrenia, but their importance was significantly downgraded in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), with little published evidence justifying the move. This brief report therefore aimed to assess the importance of FRS in distinguishing between non-affective and affective psychoses, an issue garnering only sporadic attention since Mellor (1982).
To this end, the 2010 Australian Survey of High Impact Psychosis (SHIP) represents a large-scale epidemiological survey which examined elements of FRS in individuals with a history of psychosis. A complete study description has been published (Morgan et al., 2014). We aimed to examine the lifetime prevalence of FRS in 1825 patients with a primary diagnosis of (1) schizophrenia, (2) schizoaffective disorder, (3) bipolar disorder, (4) depressive psychosis, (5) delusional disorder or (6) psychosis-not otherwise specified. Table 1 shows the prevalence of patients by group endorsing type (A) and number (B) of lifetime FRS. Most FRS appeared especially elevated in schizophrenia and schizoaffective groups, with relatively lower prevalence in remaining groups, except for heightened thought echo in depressive psychosis. Over half of affective psychoses patients endorsed at least one FRS. Comparable proportions of groups endorsed one to six FRS, although it was more likely for schizophrenia and schizoaffective groups to report seven or more FRS.
Prevalence of patients by group (%) endorsing type and number of lifetime FRS.
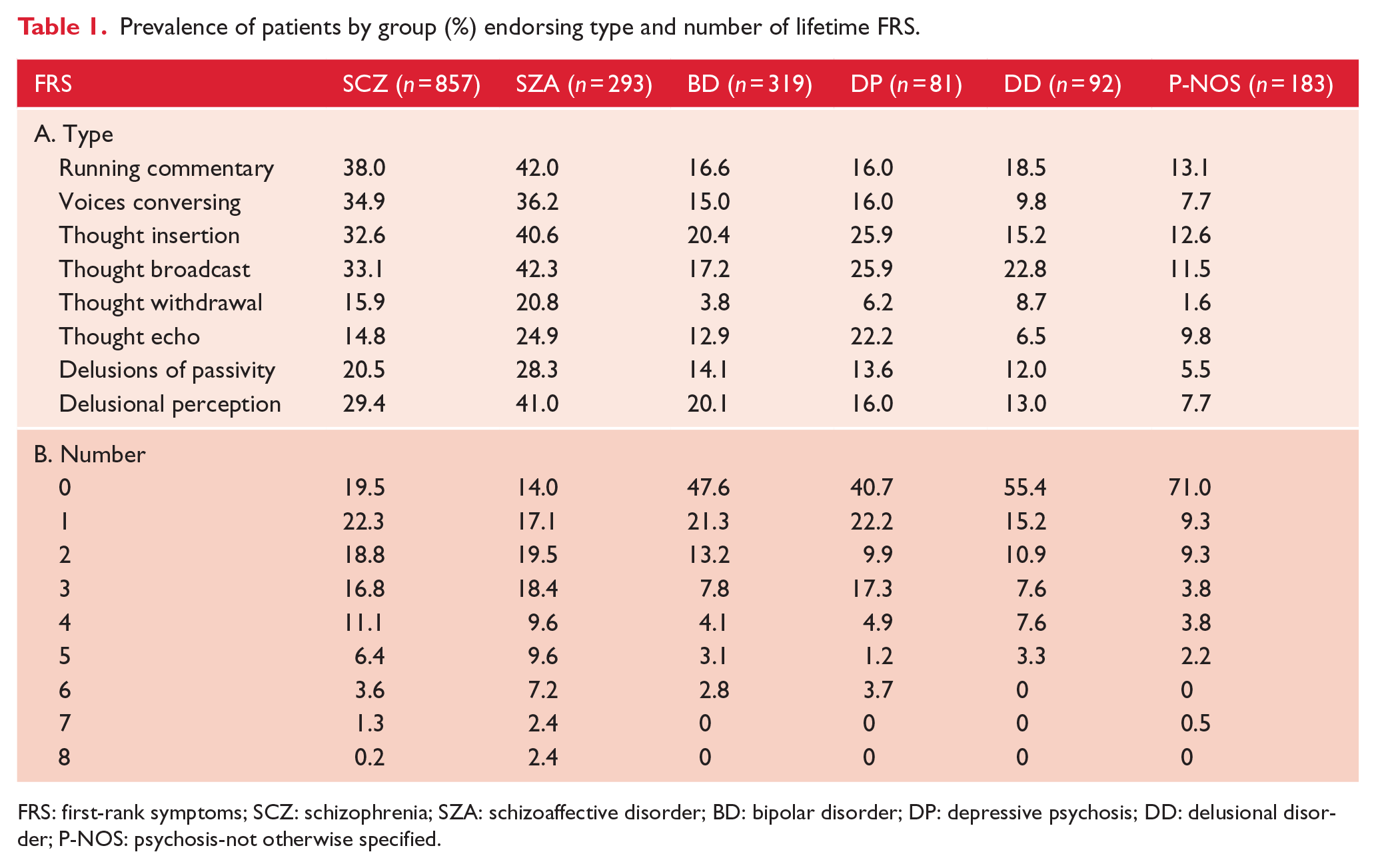
FRS: first-rank symptoms; SCZ: schizophrenia; SZA: schizoaffective disorder; BD: bipolar disorder; DP: depressive psychosis; DD: delusional disorder; P-NOS: psychosis-not otherwise specified.
Discriminant function analysis (DFA) was employed to investigate whether the presence of specific FRS could successfully predict group membership. Two significant functions were identified. Function 1, Wilks’ Λ = 0.87, χ2(32, n = 1642) = 219.8, p < 0.001, explained 10.2% of the variance in the model (canonical correlation = 0.32) and maximally separated non-affective (schizophrenia group centroid = 0.15; schizoaffective group centroid = 0.40) and affective (bipolar group centroid = −0.49; depressive group centroid = −0.47) psychoses groups. Function 2, Wilks’ Λ = 0.97, χ2(21, n = 1642) = 43.0, p < 0.005, explained only 1.7% of the variance in the model (canonical correlation = 0.13) and could not effectively discriminate between non-affective (schizophrenia group centroid = −0.10; schizoaffective group centroid = 0.21) and affective (bipolar group centroid = 0.06; depressive group centroid = 0.24) psychoses groups. Function 1 was strongly and positively correlated with running commentary, voices conversing, thought withdrawal/insertion and delusions of passivity, whereas Function 2 was strongly and positively correlated with thought echo. By inference, the shared variance between thought broadcast and delusional perception was perceived as non-discriminant across disorders.
Focusing on group membership, the original classification results revealed that only 26.7% of overall cases (schizophrenia = 24.3%; schizoaffective = 39.9%; bipolar = 11.6%; depressive = 21.0%; delusional disorder = 65.2%) were correctly classified. This modest figure was largely driven by low classification accuracies for schizophrenia and affective psychoses, with marginally improved classification accuracies for schizoaffective and delusional disorder groups. The leave-one-out cross-validated classification results were slightly less accurate at 26.3% (schizophrenia = 24.2%; schizoaffective = 38.9%; bipolar = 11.6%; depressive = 19.8%; delusional disorder = 63.0%), but largely supported the same pattern of findings. Inspection of these results did not reveal specific biases towards misclassification of any one disorder for another.
On the whole, there was higher prevalence of FRS in schizophrenia and schizoaffective groups, but FRS were by no means exclusive to non-affective psychoses. In fact, our analysis showed that approximately one in two affective psychoses patients experienced one or more FRS. Furthermore, DFA confirmed that the presence of FRS was unable to accurately verify clinical diagnosis; endorsing specific FRS did not effectively distinguish non-affective from affective psychoses groups. Therefore, the current dataset has provided some empirical support for downgrading the importance of FRS for schizophrenia diagnosis in DSM-5. We hypothesised this could be due to two reasons: (1) There is now evidence that FRS are present (albeit reduced in frequency and/or severity) in affective psychoses (Toh et al., 2015) and personality disorders, thereby diminishing their significance as a key defining feature of schizophrenia. (2) A number of authors have also commented on the heterogeneity of FRS, with patients typically reporting one or two, but very few endorsing the full range identified by Schneider (Waters, 2015). This makes it difficult to speculate on shared cognitive and neurobiological mechanisms.
In light of this, questions remain as to the exact place of Schneiderian FRS today. While FRS may not offer diagnostic specificity nor explicitly contribute towards delineating the Kraepelinian dichotomy, there remains concrete rationale for not overlooking their phenomenological importance. At present, there is a lack of consensus as to what truly constitute FRS, with these symptoms typically being inadequately characterised. Employing broad versus narrow definitions or emphasising certain key FRS (e.g. running commentary and voices conversing, as in previous editions of DSM) at the expense of others has yielded divergent findings across existing studies. Until general agreement is reached with regard to a clear definition of FRS, any endeavours to advance scientific inquiry as to their aetiology in non-affective versus affective psychoses (or other disorders), or indeed even their phenomenology, will be flawed. To this end, there perhaps needs to be a reworking of the classical concept of FRS as defined by Schneider (1939). How this is best done remains open to debate from the field. Such a move could moreover have the concomitant benefit of addressing concerns surrounding their heterogeneity, possibly stemming from fragmented classification at the outset. Another motive against discarding FRS lies in its potential for therapeutic impact. Regardless of diagnosis, FRS experiences in affected individuals can be immense in terms of emotional distress and/or psychosocial dysfunction. Added research attention thus needs to be given, with sound management of FRS forming the focus of targeted clinical interventions. For these reasons, we recommend caution in attempts to completely dismiss this genre of research.
On a related note, what does this mean for future versions of DSM (and other psychiatric classification systems relying on FRS)? We do not believe that the obvious conclusion would be to jettison the entire DSM approach to schizophrenia versus affective psychoses. While the current dataset certainly exemplifies challenges inherent to categorical rankings within the DSM, until a more rigorous but still functional classification system can be put forward, perhaps such as the Research Domain Criteria (RDoC), there remains merit in further refinements to the existing DSM. Some critics may dismiss the DFA as a pointless exercise, contending that FRS were never meant to be the sole basis for disease classification. However, we maintain that the DFA did serve as an effective statistical exercise, whose primary purpose was to stimulate constructive debate as to the precise role of FRS in DSM nosology, and more broadly psychiatric literature, moving forward.
In terms of future research, several intriguing questions may be raised: (1) How are affective psychoses patients who experience FRS different from those who do not? (2) Are there perhaps some shared cognitive and neurobiological mechanisms that underlie the operation of FRS across non-affective and affective psychoses groups? Further in-depth investigations into subsets of affective psychoses patients experiencing FRS is imperative and will bring us closer to resolving this.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis (SHIP). The members of the SHIP Study Group are V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethical approvals for the study were obtained from relevant institutional human research ethics committees. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Australian Government Department of Health and Ageing. Funding for this project was partially provided by a Barbara Dicker Brain Sciences Foundation (BDBSF) grant. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the BDBSF.