
Abstract

Man’s mind, once stretched by a new idea, never regains its original dimensions.
The accurate diagnosis of mixed states is becoming increasingly important, partly because these mood states seem to be associated with higher rates of suicide and treatment refractoriness, and partly because they are now being recognized as originating from major depression; in addition to bipolar disorder. However, clinically the primary problem of how best to capture mixed depression (predominantly depression with manic features) and mixed mania (predominantly mania with depressive features) remains, especially since the newly created ‘mixed features specifier’ in DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th edition) simply requires the presence of at least 3 symptoms from the opposing pole during either a manic or depressive episode. Apart from lacking specificity with respect to the symptoms relied upon, this definition excludes the fundamental symptoms of mixed states—distractibility, irritability and psychomotor agitation (DIP), justifying this omission on the basis that they are common to both depression and mania and therefore of no value in differentiating between them. However, in our view, it is premature to have excluded these core symptoms because their presence in both mood states is a consequence of their dimensional relationship with mood that points to common underlying factors contributing to the symptoms of mania and depression.
In practice, the lack of an appropriate definition of mixed states has distorted diagnosis and limited treatment. Therefore, we propose an alternative perspective for defining mixed states that may improve clinical identification and better inform treatment.
Diagnosis
‘True’ mixed state or transitional phase?
In attempting to understand the composition of mixed mood presentations, it is useful to consider their origin. An important distinction is whether mixed mood symptoms represent a true mixed state in which the admixture of symptoms occurs autonomously, or a mixed phase where symptoms of mania and depression simply overlap during the ‘natural’ transition between bipolar mood states. In practice, the clinical picture is often further complicated by the effects of medications, which in some instances can ‘create’ a syndrome of mixed mood symptoms, known as a Treatment-Emergent Affective Switch (TEAS). Therefore, when assessing mood states, it is important to fully contextualize mixed episodes because this information will assist in teasing apart whether patients have a true mixed state, are transitioning between mood states (mixed phase) and/or are experiencing TEAS.
Core features of mixed states
Certain symptoms are common to both predominantly manic and depressive mixed mood states, such as anxiety, irritability and agitation, and recent research has shown that these symptoms characterize a significant proportion of mixed mood presentations (Pacchiarotti et al., 2013; Young and Eberhard, 2015). Furthermore, in mixed depression, irritability and psychomotor agitation are the most discriminant features but not the most prevalent (Benazzi and Akiskal, 2006), whereas in mixed manic states, loss of interest and energy, feelings of worthlessness and helplessness are the features most predictive of a mixed episode (Kim et al., 2013). These findings suggest that some of the symptoms excluded by DSM-5 may indeed be core to the identity of mixed states.
Mixed states in 3D: mood, thought and psychomotor activity
It has long been hypothesized that fluctuations along the dimensions of thought, mood and psychomotor activity give rise to varied mixed mood state presentations. Specifically, Kraepelin and Weygandt proposed 6 subtypes of mixed states (see Figure 1)—best mapped by longitudinal assessment of each of the three dimensions of thought, activity and mood. Each dimension is ‘activated’ during pure mania and ‘inhibited’ during depression, and combinations of varying degrees within each of these dimensions produces a variety of mixed states.
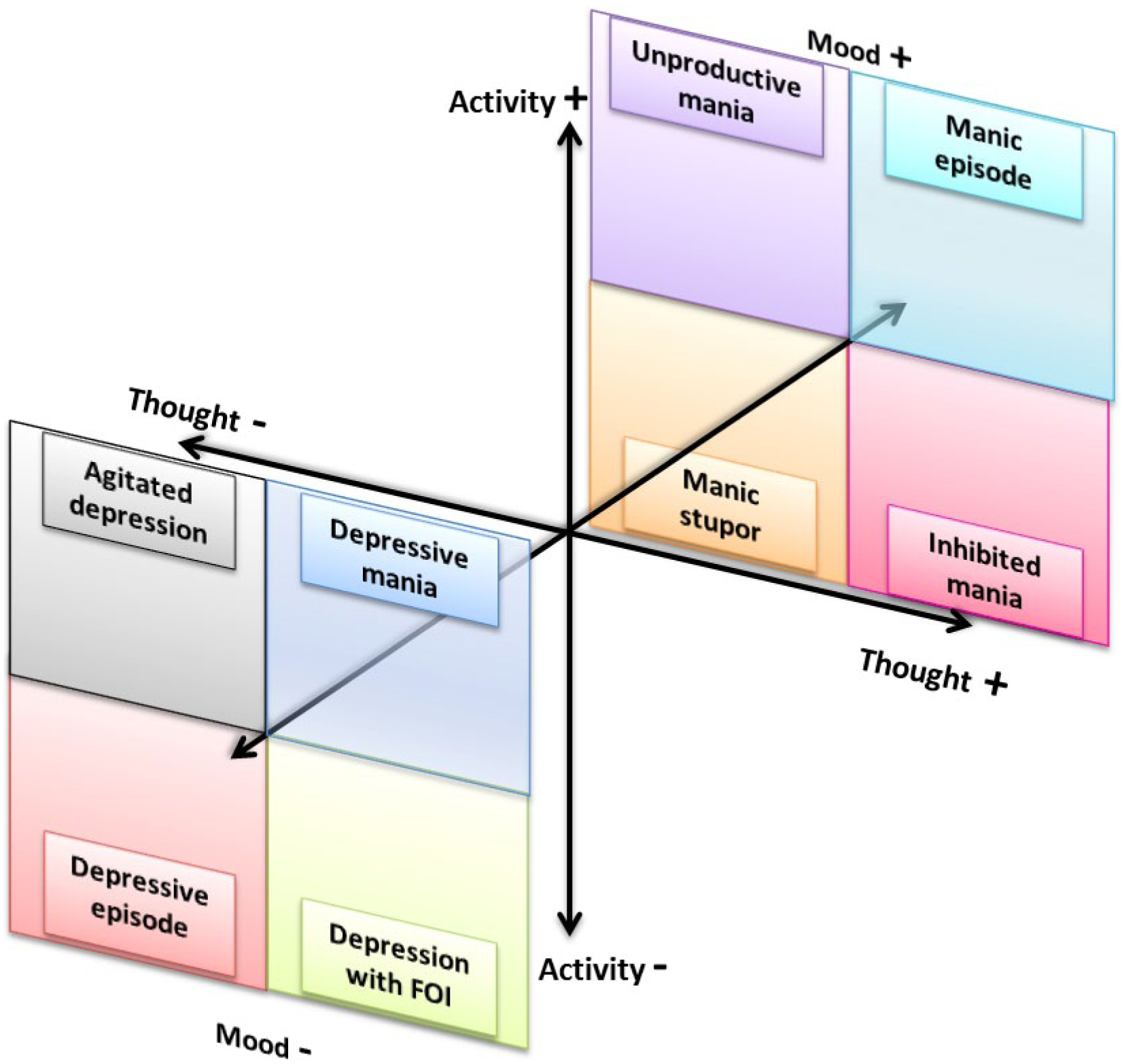
Varying degrees of activation (+) and inhibition (−) along the dimensions of thought, mood and activity create ‘pure’ depressive and manic episodes as well as six subtypes of mixed states, initially proposed by Kraepelin and Weygandt: Unproductive mania—activated mood and activity, and inhibited thought; Manic stupor—activated mood and inhibited thought and activity; Inhibited mania—activated mood and thought, and inhibited activity. Agitated depression (Excited depression)—inhibited mood and thought, and activated activity; Depressive mania (Irritable depressive mania; Anxious mania; Furious mania)—inhibited mood, and activated thought and activity; Depression with flight of ideas (FOI)—inhibited mood and activity, and activated thought.
Adopting a 3D perspective
Detailing fluctuations along the dimensions of thought, activity and mood, Weygandt focused on three types of mixed states because of their greater prevalence and persistence: manic stupor characterized by elevated mood, and inhibited thought and activity; agitated depression which features depressed mood, inhibited thought and increased psychomotor activity; and unproductive mania which differs from agitated depression only in terms of mood. Despite a degree of similarity between these mixed state subtypes, it is important to note that they differ with respect to severity along these dimensions. This is also true for their overall clinical profile with varying combinations of additional symptoms of differing intensity. This approach to describing mixed states better captures the context in which symptoms occur compared to the approach adopted by DSM-5, in which the only context differentiating mixed mania and mixed depression is the primary mood state.
In reality, there are a number of ways that symptoms cluster to create further nuanced mixed states. For example, a recent factor analysis of bipolar patients identified two subtypes of mixed states; a ‘pure’ mixed presentation, similar to ‘agitated depression’, consisting of anxiety, tension, suicidality, motor hyperactivity, excitement and the absence of motor retardation, in a predominantly depressed mood (Pacchiarotti et al., 2013), and another (less well characterized) mixed state subtype that comprises irritability and dysphoria. Interestingly, the two ‘forms’ seem to also differ in terms of illness profiles, clinical course and suicidality.
Examining the clinical features of patients with DSM-III-R (Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised) mania, an earlier study (Cassidy et al., 2001) found 5 subtypes, two of which were mixed. In the larger mixed group (21.4% of the sample), depressed mood, anxiety, suicidal ideation, feelings of guilt, irritability, aggression, psychosis and paranoia were the prominent features, and these patients also experienced moderate levels of racing thoughts and pressured speech, but notably lacked euphoria and grandiosity; resembling Kraepelin’s ‘depressive or anxious mania’. The other mixed subtype (15.6% of the sample) had high levels of depressed mood, anxiety and lability, but the symptoms of guilt and suicidality were supplanted by euphoria, or grandiosity, or humor, or psychosis. Interestingly, over time, the two mixed mania presentations also separated in terms of their longitudinal pattern with a sustained depressed and irritable mood state eventuating in depressive mania versus frequent alternation between elevated and depressive mood states.
In present day psychiatric practice, too great an emphasis is placed on emotional symptoms, e.g., elevated mood and grandiosity, partly due to DSM-5’s definition of mixed features. However, in reality, patients in a ‘true’ mixed state are more likely to present with symptoms of agitation and irritability, and in fact seldom exhibit euphoria. Hence, clinically, it may prove more useful to focus on the extent to which symptoms are mixed across all three dimensions. Applying a 3D framework to define mixed states in this manner should provide richer more granular descriptions of mixed presentations.
Conclusion
Conceptualizing mixed states along additional domains of activity and thought is a significant departure from traditional mood-centric categorical classifications and reflects the reality that the clinical manifestations of mood disorders, and in particular mixed states, are complex and likely to reflect dimensional variations. The three dimensional approach we have proposed examining thought, mood and activity, ideally over time (adding a fourth longitudinal dimension), is likely to improve the diagnosis and management of mixed presentations and may help develop a deeper understanding of mood disorders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GM has received funding from a National Health and Medical Research Council (NHMRC) Program Grant (APP1073041); American Foundation for Suicide Prevention (PRG-0-090-14); and SPARK.