
Abstract
Objective:
Oxidative stress, inflammation and heavy metals have been implicated in the aetiology of autistic disorder. N-acetyl cysteine has been shown to modulate these pathways, providing a rationale to trial N-acetyl cysteine for autistic disorder. There are now two published pilot studies suggesting efficacy, particularly in symptoms of irritability. This study aimed to explore if N-acetyl cysteine is a useful treatment for autistic disorder.
Method:
This was a placebo-controlled, randomised clinical trial of 500 mg/day oral N-acetyl cysteine over 6 months, in addition to treatment as usual, in children with a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision diagnosis of autistic disorder. The study was conducted in Victoria, Australia. The primary outcome measures were the Social Responsiveness Scale, Children’s Communication Checklist–Second Edition and the Repetitive Behavior Scale–Revised. Additionally, demographic data, the parent-completed Vineland Adaptive Behavior Scales, Social Communication Questionnaire and clinician-administered Autism Diagnostic Observation Schedule were completed.
Results:
A total of 102 children were randomised into the study, and 98 (79 male, 19 female; age range: 3.1–9.9 years) attended the baseline appointment with their parent/guardian, forming the Intention to Treat sample. There were no differences between N-acetyl cysteine and placebo-treated groups on any of the outcome measures for either primary or secondary endpoints. There was no significant difference in the number and severity of adverse events between groups.
Conclusion:
This study failed to demonstrate any benefit of adjunctive N-acetyl cysteine in treating autistic disorder. While this may reflect a true null result, methodological issues particularly the lower dose utilised in this study may be confounders.
Introduction
The underlying genetic, environmental and biochemical factors have been a focus in research into autism spectrum disorders (Matson and LoVullo, 2009). A mounting body of evidence has implicated oxidative stress as a potential contributing factor in the aetiology of autism disorders (Villagonzalo et al., 2010), particularly the antioxidant glutathione and its pathways (Main et al., 2012). Glutathione is one of the most important and ubiquitous antioxidants in the human body (Berk et al., 2008c). It acts as a free radical scavenger and helps to buffer reactive products of oxidative reactions. Glutathione also facilitates a number of other critical functions within the cell that include DNA repair, protein and prostaglandin synthesis, amino acid transport and enzyme activation (Wu et al., 2004). Glutathione is also essential for gastrointestinal and immune system functioning, and detoxification of organic and inorganic xenobiotics, including heavy metals such as mercury and lead (Kern and Jones, 2006; Sen, 1997).
A systematic review reported relatively consistent findings of glutathione deficiency in autism (Main et al., 2012). These results have been replicated (Adams et al., 2011; Al-Yafee et al., 2011; Geier et al., 2009), providing evidence for a potential role of glutathione deficiency in autistic disorder. Autistic disorder is also associated with a range of systemic abnormalities linked to glutathione dysfunction, including decreased detoxification capacity of heavy metals, phenolic compounds and acetaminophen (Kern and Jones, 2006), processes for which glutathione is essential (Sen, 1997). Glutathione also plays a role in gastrointestinal and immune functioning (Sen, 1997), both of which have been shown to be impaired in autism (Cohly and Panja, 2005; Molloy and Manning-Courtney, 2003).
Glutathione has thus been proposed as a treatment target in autistic disorder (Berk et al., 2008c). Administration of N-acetyl cysteine (NAC) is an effective method of replenishing cysteine, the rate-limiting agent in glutathione synthesis (Atkuri et al., 2007).
Pilot studies, commenced at a similar time to the current study, of NAC in children with autism have reported equivocal results. In a placebo-controlled, randomised trial (n = 31), Hardan et al. (2012) using a dose of 900 mg daily for the first 4 weeks, 900 mg BID for 4 weeks and 900 mg TID for 4 weeks found no change on the total Aberrant Behaviour Checklist (ABC) scores, but found significant improvements in the irritability subscale of the ABC in the NAC treatment group over 12 weeks. NAC treatment was also associated with improvements in social cognition and a trend in repetitive stereotyped behaviours and autism mannerisms. Ghanizadeh and Moghimi-Sarani (2013) in a placebo-controlled, randomised trial of NAC 1200 mg/day in addition to risperidone (n = 40), found that NAC did not alter the primary outcome, overall behaviour and emotional problems as measured by total scores on the ABC, but significantly reduced the irritability subscale of the ABC in children with autism. They found no changes in stereotypic behaviour, communication or social interaction. Both these trials were characterised by their small sample size and relatively short duration. The aim of the current study was to investigate the efficacy of NAC compared to placebo in a larger sample with a wider range of outcome measures, over a period of 6 months.
Methods
Study design
This study was a placebo-controlled, randomised clinical trial of 500 mg/day oral NAC for 6 months, in addition to treatment as usual, in children with autistic disorder. The study was conducted across two outpatient sites, both located in Australia: the Centre for Developmental Psychiatry and Psychology (CDPP), Monash University, and Barwon Health/Gateways Support Services, Geelong.
The trial was approved by Barwon Health (09/141) and Monash University (2010001294) Human Research and Ethics Advisory Committees, and conducted in accordance with the Good Clinical Practice guidelines under a Clinical Trial Notification provided to the Therapeutic Goods Administration. A full protocol was developed in accordance with Standard Protocol Items Recommendations for Intervention Trials (SPIRIT) 2013 guidelines, and the study reported using Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Participants
Participants were recruited through autism assessment services, community-based autism support services, including Autism Victoria (Amaze) and the wider media. Individuals were eligible for participation in this study if they had a diagnosis of Autistic Disorder according to DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision) criteria (American Psychiatric Association, 2000) and were aged between 3 and 9 years, inclusive, upon entry to the study. Diagnoses were confirmed through comprehensive case review of all available past and current assessment materials and reports by two child psychologists experienced in the assessment and diagnosis of autistic disorder in children. Children undergoing any pharmacological treatment for autistic disorder were allowed to continue with that treatment, as usual. At least a two week period of stable treatment was required for inclusion into the study. Any changes of treatment during the study period were noted, but this did not constitute withdrawal from the trial.
Individuals were excluded from the study if they had a known or suspected clinically relevant systemic medical disorder or known genetic or metabolic cause of developmental delay, such as fragile X or Rett syndrome; had a prior sensitivity or allergy to NAC; were considered likely to be unable to comply with the treatment protocol, e.g., having a highly restricted diet leading to refusal to take NAC; had parents/guardians who were non-fluent in English; had a history of asthma or epilepsy, as these are equivocally influenced by NAC (Carlsten et al., 2014; Reinero et al., 2011); or were already receiving any treatment containing NAC, glutathione or their precursors. Participants were withdrawn from the study if they ceased taking the trial medication for 7 consecutive days, parents/guardians withdrew consent or a serious adverse event occurred that impacted their participation. Withdrawal due to adverse events could be either at the request of the parent/guardian or the discretion of the investigator.
Randomisation and masking
The investigational product in this study was 500 mg NAC or placebo capsules, administered orally once daily. The dose was selected based on our previous experience with NAC. Specifically, we selected 500 mg/day based on the adult dose of 2000 mg/day being effective in our previous trials of NAC in psychiatry, over a similar treatment period (Berk et al., 2008a, 2008b, 2014) and with no reliable information on the safety profile of NAC in children. The study was commenced in 2010 and was unknowingly being run in parallel with that of Hardan and Ghanizadeh. As such, our selection of dose for the study was based on titration of an adult dose we had been using in our previous trials. The NAC and placebo capsules were identical in size and appearance, and were stored in identical bottles. The outside of the placebo capsules was lightly dusted with trace amounts of NAC to approximate the smell of the active capsules and assist in keeping participants blinded. If a participant was unable or unwilling to swallow the capsules whole, parents/guardians were advised to empty and stir the capsule contents into a beverage. Examples of delivery methods included orange juice or chocolate flavoured milk.
Participants were randomised sequentially into either the NAC or placebo groups using a computer program designed for clinical trial randomisation (randomization.com). An independent researcher, who had no contact with any participants, coordinated the computer-generated randomisation codes. Treatment and placebo packs were randomly allocated in blocks of four, with a treatment/placebo ratio of 1:1. Participants, their parents/guardians, trial staff and the statistician were blind to treatment arm allocation for the duration of the study.
Procedures
Participants and their parents/guardians attended appointments at baseline, 1, 3 and 6 months and were provided with a bottle of capsules at the first three visits. For each participant, the first dose of NAC or placebo was administered at the baseline visit, in order to monitor for any acute reactions in a supervised environment.
During the treatment phase, an adverse events checklist was completed on a monthly basis post-baseline to monitor adverse events or safety concerns. Questionnaires were completed by parents/guardians at baseline, 1, 3 and 6 months. Unless there were prohibiting circumstances, the same parent/guardian completed all questionnaires and attended all interviews.
Phone interviews were conducted at 2, 4 and 5 months to monitor any adverse events between appointments. In the event of urgent safety concerns, procedures were in place to refer participants to immediate medical treatment, with unblinding to occur if deemed medically necessary.
Outcomes
Primary outcomes
The primary outcome measures were improvement in social skills (e.g. social awareness, capacity for reciprocal social communication) as measured by the Social Responsiveness Scale (SRS), improvement in verbal and non-verbal communication, as measured by the Children’s Communication Checklist–Second Edition (CCC-2) and improvement in repetitive and stereotypic behaviour as measured by the Repetitive Behavior Scale–Revised (RBS-R) and their subscales over the course of the treatment (baseline, 1, 3 and 6 months).
Composite scores derived from the CCC-2 include the General Communication Composite (GCC) and the Social Interaction Deviance Composite (SIDC). The GCC and SIDC are demonstrably sensitive measures in identifying communication difficulties and pragmatic language impairments in children with autistic disorders.
Baseline measures
At baseline only, a demographic interview was completed, along with the parent-completed Vineland Adaptive Behavior Scales–Second Edition (Vineland-II) and Social Communication Questionnaire (SCQ)–Lifetime and Current versions. A subset of participants also completed an age-appropriate cognitive assessment: the Wechsler Preschool and Primary Scale of Intelligence–Third Edition (WPPSI-III) for children aged up to 7 years, or the Wechsler Intelligence Scale for Children–Fourth Edition (WISC-IV) for children aged over 7 years. Cognitive assessments were only conducted with participants who did not have a current assessment (i.e. had not completed a cognitive assessment in the last 2 years).
Secondary outcomes
Secondary outcomes were the Developmental Behaviour Checklist–Primary Carer Version (DBC-P) (Einfeld and Tonge, 1995) and three global impression scales known as the Parent Global Impression–Improvement scale (PGI-I), Clinical Global Impression–Improvement scale (CGI-I) and Clinical Global Impression–Severity scale (CGI-S).
The DBC-P consists of 96 items, forming five subscales: Disruptive, Self-Absorbed, Communication Disturbance, Anxiety and Social Relating, and a total score (Total Behaviour Problem Score). The DBC-P Attention Deficit Hyperactivity Disorder (ADHD) scale and a series of individual DBC-P items (37: Impulsive; 38: Irritable; 85: Tense, anxious, worried) were secondary outcomes.
Statistical analysis
Sample size calculation
The three primary outcomes for this intervention were continuous endpoints. For evaluation of intervention efficacy, the pertinent quantity is the difference D between mean change (from baseline to week 24) in the two treatment arms. A dimensionless effect size (ES) is defined as ES = D/σ, where σ is an overall estimate of the standard deviation (SD) of change. With a sample of 98 participants (49 per group), the differential change in the main outcomes detectable with 80% power and two-sided Type I error rate α = 5% is 0.57.
Data analysis
T-tests and chi-square tests were used to compare baseline characteristics between the intervention and control groups. An intention to treat (ITT) analysis was performed using a linear mixed model approach. To assess the impact of the intervention on primary and secondary outcomes, time by treatment interactions were examined in a repeated measures split-plot in time analysis of variance (ANOVA) model for continuous outcomes. Model parameters were estimated using generalised estimating equations (GEEs) with an exchangeable working correlation matrix to take account of the repeated measures for each participant. The overall p-values for intervention by follow-up interaction were reported. Follow-up by intervention interaction impacts and their 95% confidence intervals (CIs) were reported. ESs (follow-up by intervention effect) were calculated using Cohen’s d. A secondary set of analyses were planned to adjust for any baseline characteristics that were found to be imbalanced between groups to the extent of a 0.25 SD difference in means (quantitative measures) or an odds ratio of 1.5 (binary measures). Tests were two-tailed with statistical significance set at an alpha level of 0.05. The analyses were undertaken using STATA© 13.
Results
Participant flow
Eligible participants were recruited from April 2011 to April 2013. In total, 102 children with autistic disorder were randomised into the study. Of these, 98 children (79 male, 19 female; age range: 37–119 months) attended the baseline appointment with their parent/guardian, forming the ITT sample.
Figure 1 displays the participant flow through the study. A total of 71 participants completed the 6-month trial, 35 from the placebo group and 36 from the NAC group.

Participant flow chart.
Baseline characteristics
Participants in the treatment and placebo groups did not differ significantly on any demographic or baseline measure. Table 1 summarises these characteristics by group.
Baseline characteristic of the sample (N = 98).
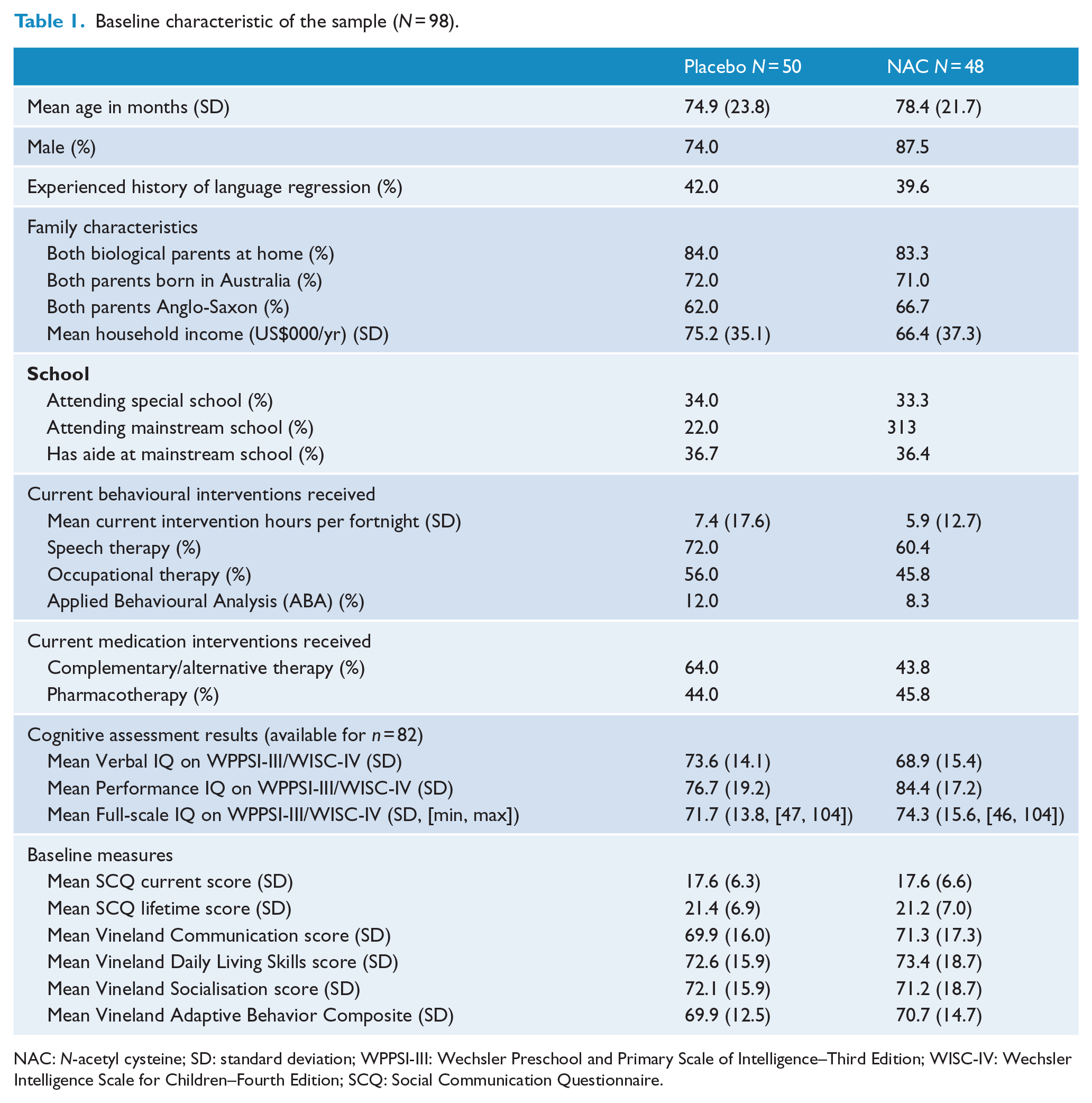
NAC: N-acetyl cysteine; SD: standard deviation; WPPSI-III: Wechsler Preschool and Primary Scale of Intelligence–Third Edition; WISC-IV: Wechsler Intelligence Scale for Children–Fourth Edition; SCQ: Social Communication Questionnaire.
At baseline, the mean age of the sample was 6 years and 4 months (SD = 22 months). Most participants (64.3%) came from an Anglo-Saxon background, with the majority of participants’ parents (71.4%) also being born in Australia. All participants were living with at least one biological parent, except for one who lived with his grandparents. Most participants (83.7%) lived with both biological parents in one home.
Two-thirds of participants were currently attending mainstream (26.5%) or special school (33.7%), with a small number attending both concurrently (4.1%). Of those attending a mainstream school, 36.5% had access to a classroom aide. Almost all participants were currently engaged in some form of behavioural therapy at baseline (78.6%). Hours spent in behavioural intervention at baseline ranged from 1–100 hours per fortnight (mean = 6.67 hours per fortnight). Use of pharmacotherapy was less common with 26.5% on a psychotropic medication (most commonly; melatonin – 12/2% and risperidone – 5.1%). Other medications included health supplements (most commonly fish oil – 19.4%), anti-allergy medication (total use – 5.1%), skin medication (total use – 4.1%) and 9.1% of children were on a range of other medications (e.g. paracetamol). There was no difference between the groups in terms of average hours per week in terms of behavioural therapy interventions.
Primary outcomes
There were no significant differences between NAC and placebo-treated groups for any of the primary (Table 2) or secondary (Table 3) outcome measures. Regarding primary outcomes, scores on the SRS, Children’s Communication Checklist and the RBS showed no between group differences, nor did subscale scores differ. Similarly, secondary outcomes, the DBC-P, and three global impression scales, the PGI-I, CGI-I and CGI-S, did not differ between the NAC and placebo-treated groups.
Main outcomes comparison at 4-, 12- and 24-week follow-up.

SD: standard deviation; NAC: N-acetyl cysteine; CI: confidence interval.
Overall p-value for the NAC by follow-up interaction.
Follow-up vs baseline by intervention group interaction with placebo at baseline as reference group.
Secondary outcomes comparison at 4-, 12- and 24-week follow-up.

SD: standard deviation; NAC: N-acetyl cysteine; CI: confidence interval; PBO: placebo group; CGI-S: Clinical Global Impression–Severity; DBC: Developmental Behaviour Checklist; TBPS: Total Behaviour Problem Score; ADHD: Attention Deficit Hyperactivity Disorder.
Overall p-value for the NAC by follow-up interaction.
Follow-up vs baseline by intervention group interaction with placebo at baseline as reference group.
All primary and secondary outcomes for baseline to 24-week follow-up were compared using the GEE approach as secondary analyses. No significant intervention effects were found. Cohen’s d ESs for secondary analyses were similar to those reported in Tables 2 and 3.
Safety and tolerability
NAC was well tolerated by participants. Two participants from the placebo group were withdrawn due to unwillingness to take the trial medication, compared to 0 from the NAC group. Table 4 shows the number of adverse events by group. Gastrointestinal symptoms and colds/cold-like symptoms were the most frequently experienced adverse events, occurring roughly equally across both groups.
Incidence of participants experiencing adverse events by group.

NAC: N-acetyl cysteine.
There were two serious adverse events involving the hospitalisation of participants. One participant in the NAC group was hospitalised for dental surgery unrelated to the trial. A participant from the placebo group was withdrawn from the study following hospitalisation for treatment of a bowel obstruction. Case review by the investigators indicated that this was a pre-existing issue for this child and unlikely to be related to the trial medication. There was no significant difference in the number and severity (mild, moderate, severe) of adverse events between NAC and placebo at months 1, 3 and 6.
Discussion
This placebo-controlled, randomised trial investigated the efficacy of NAC 500 mg daily in 98 children with autistic disorder. No significant differences were found on the primary outcomes of communication, social interaction and repetitive behaviours, or on the secondary outcomes of problem behaviours or parent/clinical global impression. Even without Bonferroni correction for multiple testing, no significant effect on any symptoms domain emerged, suggesting a true null effect of NAC at the dose used.
These results are in contrast to the previous studies by Hardan et al. (2012) and Ghanizadeh and Moghimi-Sarani (2013), both of which failed to find a change in total ABC scores, the primary outcome of both studies, but found that NAC significantly improved ABC irritability scores. Hardan et al. (2012) found improvements in social cognition and autistic mannerisms on the SRS and a reduction in repetitive behaviours on the RBS-R in the NAC treatment group. The reason for the difference between these results and the current trial is unclear. Clinical and selection factors may be relevant, including dosage, different ages, clinical populations, levels of acuity, comorbidity and concomitant psychosocial therapy among many operative variables. Autistic disorder is also a particularly heterogeneous clinical phenotype, and this too may have played a role in these divergent results (Betancur, 2011).
This study was the largest and longest treatment duration (6 months) of any clinical trial of NAC in children with autistic disorder to date. The sample may be considered reasonably representative, with a gender ratio (4:1) matching that in the population of children with autistic disorder, and a relative diversity of socioeconomic backgrounds. A range of comprehensive, valid measures was used to assess changes in autism symptomatology across the trial.
Limitations of this study included the moderate rates of withdrawal (19.4%) and loss to follow-up (8.2%). The relatively long duration of the trial, 6 months, as well as the time commitment involved in completing trial appointments and questionnaires, may have contributed to this. In addition, this study relied mainly on parent report of symptoms, aside from the use of the Clinical Global Impressions scales, and the ABC scale (showing efficacy in other studies) was not used in the current study. No tests of biomarkers were included to check whether the administration of NAC at this dose had any effect on glutathione levels or any other of the neurobiological targets of NAC. Since this study was designed, there has been a randomised controlled trial published, using a smaller sample size with also non-significant primary outcomes, but with a signal for reduced irritability (Hardan et al., 2012). Given this, and the adjunctive nature of the intervention, future studies may consider powering their sample size against a smaller ES. The current study employed a moderate–large ES (0.5) for the power calculation but a more conservative estimate may be warranted.
This study used a much lower dose of NAC than the Hardan et al. (2012) and Ghanizadeh and Moghimi-Sarani (2013) trials (2700 and 1200 mg/day, respectively). The dose of 500 mg/day was chosen in this study due to the younger age of some participants, and the lack of safety and tolerability data for NAC over longer durations in children. However, the relatively low dose may be a reason this study failed to replicate the results of the two pilot studies. Other studies that have looked at variable or higher doses of NAC suggest that higher doses may be necessary.
Conclusion
This study failed to demonstrate any benefit of NAC in the management of autistic disorder. While this may be a true null result, methodological issues particularly clinical subtypes and dose require closer examination in future studies. This trial was registered on the Australian New Zealand Clinical Trials Registry (ACTRN12610000635066).
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Simons Foundation Autism Research Initiative (SFARI) Grant 201473. A pilot award and scholarship support for Ms Villagonzalo was obtained from Australian Rotary Health. Michael Berk is supported by a National Health and Medical Research Council (NHMRC) Senior Principal Research Fellowship (1059660). We gratefully acknowledge these funding sources.