
Abstract
Objective:
Clinical experience suggests a growing prevalence of borderline personality disorder in aged residential care and psychiatric facilities with attendant difficulties in their management. This paper reviews the literature concerning the prevalence, phenomenology and diagnosis of borderline personality disorder in old age. The aim is to elucidate the phenomenological differences in old age and thus improve identification of the disorder.
Methods:
A systematic search was conducted using MEDLINE, PubMed, EMBASE and PsycINFO databases, employing the search terms including ‘personality disorder’, ‘borderline personality disorder’, ‘aged care’, ‘gerontology’, ‘geriatric psychiatry’ and ‘life span’. The search included articles in English involving participants 65+ years. Long-term prospective studies of borderline personality disorder, long-term follow-up studies and studies involving older adults from 50+ years were also examined.
Results:
There is a paucity of literature on borderline personality disorder in the elderly. No diagnostic or rating instruments have been developed for borderline personality disorder in the elderly. The phenomenology of borderline personality disorder in the aged population differs in several respects from that seen in younger adults, causing some of the difficulties in reaching a diagnosis. Escalations of symptoms and maladaptive behaviours usually occur when the diagnosis of borderline personality disorder is either not made or delayed. Improved identification of borderline personality disorder in older patients, together with staff education concerning the phenomenology, aetiology and management of these patients, is urgently needed.
Conclusion:
Diagnostic instruments for borderline personality disorder in the elderly need to be developed. In the interim, suggestions are offered concerning patient symptoms and behaviours that could trigger psychiatric assessment and advice concerning management. A screening tool is proposed to assist in the timely diagnosis of borderline personality disorder in older people. Timely identification of these patients is needed so that they can receive the skilled help, understanding and treatment needed to alleviate suffering in the twilight of their lives.
Introduction
The forecast for sustained growth in the global ageing population is a clarion call for the expansion of aged care-appropriate accommodation and services. Changes in roles and health status during ageing may exacerbate the expression of maladaptive personality traits, resulting in behaviours that are disruptive and distressing in the communal environments of aged care facilities. This paper reviews the literature concerning the prevalence, phenomenology and diagnosis of borderline personality disorder (BPD) in old age, documenting changes in the presentation of BPD during the life span that are not reflected in the current diagnostic criteria. Diagnosis is the first important step as it leads to greater awareness of the significant behavioural problems and disruptions that may accompany BPD. Accurate and timely diagnosis promotes understanding and paves the way for research on best practice with respect to BPD management and staff training.
Prevalence of BPD in old age
The prominence of personality disorders (PDs) including BPD is likely to increase with population ageing (Mordekar and Spence, 2008). Clinical experience suggests that BPD is more prevalent in the elderly than previously recognized, which concurs with the research available (Molinari et al., 1994; Richa and Ibrahim, 2012). The prevalence of PDs in community-dwelling adults has been highlighted in several studies, including Lenzenweger (2008), who reported a PD prevalence of 9% and 11% in the two US studies of community-dwelling adults, with a prevalence of 1.3% and 1.4%, respectively, for BPD. This is consistent with other well-conducted epidemiological studies. Torgersen et al. (2001) reported a prevalence of 13.4% for any PD in a Norwegian sample of community-dwelling adults, with 0.7% of this cohort diagnosed with BPD. Three studies have reported a decreasing prevalence of cluster B PDs with increasing age (Engels et al., 2003; Samuels et al., 2002; Ullrich and Coid, 2009). In Australia, Jackson and Burgess (2000) found that 6.5% of 10,641 community-dwelling Australian adults had at least one PD using International Classification of Diseases, 10th revision (ICD-10) criteria. Of these, 0.96% were diagnosed with borderline and 1.33% with impulsive PD. However the prevalence of BPD in adults aged 65 or older was not separately examined in that study.
Although the prevalence of BPD is greater in clinical populations than in the community, information regarding its prevalence in elderly psychiatric populations is highly variable. Widiger and Seidlitz (2002) reviewed six studies that used validated structured interviews for the diagnosis of PDs in elderly psychiatric samples. Prevalence rates for the diagnosis of ‘any PD’ ranged from 10% to 63%, which the authors attributed to differences in the study populations and assessment methods. A more recent Australian study (Stevenson et al., 2011) found that 60% of 98 psychiatric inpatients older than 65 years met criteria for at least one PD. Although this finding requires replication, it highlights the high prevalence of PDs in old age psychiatric inpatient settings. To date, we have found no reliable data concerning the specific prevalence of BPD in the aged psychiatric population in Australia. This is clearly important since the significance of mental illness, and PD in particular, may be underemphasized in the aged. This is exemplified in the Mental Health Council of Australia Fact Sheet which cites the prevalence of mental health disorders as 1 in 4 young adults (16–24 years) but only 1 in 20 elderly adults (75–85 years) (Mental Health Council of Australia, n.d.). In contrast, the Royal Australian and New Zealand College of Psychiatry (RANZCP, 2010) publication, ‘Older Australians Deserve a Better Deal in Mental Health’, cites a higher prevalence of mental health problems in the aged that is more commensurate with international evidence, however makes no mention of the significant involvement of PD among the listed disorders.
Phenomenology of BPD in old age
A recent review of PDs across the life span (Newton-Howes et al., 2015) points out the high prevalence of PDs as well as their propensity to persist and evolve over a lifetime. Zanarini et al. (2012), in 16 years of prospective follow-up of a large cohort of inpatients in the McLean Study of Adult Development (MSAD), identified a pattern of improvement for some features of BPD over time. These authors define acute symptoms as those which spontaneously resolve relatively early. These include core features of impulsivity such as suicidality and deliberate self-harm (DSH), the tendency to manage interpersonal issues with demandingness or entitlement, and severe treatment regressions. However, the so-called ‘temperamental symptoms’ of BPD were more persistent and often associated with ongoing psychosocial impairment. These include affective symptoms such as chronic dysphoria, anger, emptiness and interpersonal symptoms such as abandonment fears and dependency issues, which were slowest of all to resolve or improve. It is these temperamental and interpersonal symptoms that have emerged as the clinical hallmarks of BPD in the elderly. This finding was corroborated by the Collaborative Longitudinal Personality Disorder Study (CLPS) of Gunderson et al. (2011), which also reported a decrease in impulsivity with age. A smaller retrospective study by Rosowsky and Gurian (1991) reviewed the medical records of eight elderly patients who had been diagnosed with BPD and concluded that the symptoms of BPD that persisted into old age were unstable and intense interpersonal relationships; unstable, intense and labile affect; inappropriate intense and poorly controlled anger; and past therapy relationships characterized by ‘specialness’, splitting and countertransference problems.
The phenomenology of PDs in old age, often including BPD, has been examined by a range of authors (Abrams and Bromberg, 2006, 2007; Morgan et al., 2013; Oltmanns and Balsis, 2011; Rosowsky and Gurian, 1991; Sadavoy, 1996; Zweig, 2008). Many studies report significantly lower levels of impulsivity, self-harm and substance-use disorders in the elderly population with BPD compared with younger and middle-aged adults (Arens et al., 2013; Blum et al., 2008; Morgan et al., 2013; Richa and Ibrahim, 2012; Rosowsky and Gurian, 1991; Stevenson et al., 2003).
Studies that show decreased levels of impulsivity with ageing (Zanarini et al., 2012) and in the aged (Arens et al., 2013; Blum et al., 2008; Morgan et al., 2013; Stepp and Pilkonis, 2008; Stevenson et al., 2003) serve to highlight the limited utility of impulsivity as a diagnostic feature of BPD in the elderly. Identity disturbance of the kind seen in younger adults is also reduced in old age (Blum et al., 2008; Rosowsky and Gurian, 1991; Trappler and Backfield, 2001). Given that impulse dysregulation and lack of consistent sense of identity are both core features of BPD in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), their absence reduces the sensitivity of the DSM measures, adding to the difficulties in diagnosing BPD in the aged.
Two other core features, emotional dysregulation and disturbed interpersonal relationships, do however persist in older BPD patients (Gutiérrez et al., 2012). Evaluation of 1447 patients, aged 15–82 years, found significant declines in borderline features to the age of 50, particularly in the externalizing aspects of cluster B including impulsivity, rule breaking and emotional turmoil. It was notable that abandonment fears, selfishness, lack of empathy and manipulation remained the same when the data were analysed at criterion level. A likely consequence of this is illustrated in a community sample study of older adults aged 55–64 years (Powers et al., 2013). These authors found that symptoms of BPD predicted interpersonal stressful life events that were attributable to unstable interpersonal relationships and impulsivity. They noted that while impulsivity decreases with age in BPD, it can continue to result in negative consequences ‘even when present at sub-threshold levels of the disorder’ (p. 473). These observations clearly demonstrate the insensitivity of the current DSM criteria for elderly patients, emphasizing the need to develop a revised set of diagnostic criteria for BPD in the aged population (Blum et al., 2008; Morgan et al., 2013; Oltmanns and Balsis, 2011; Powers et al., 2013; Richa and Ibrahim, 2012; Rosowsky and Gurian, 1991; Trappler and Backfield, 2001).
There is growing awareness among clinicians that older patients with BPD have higher levels of ‘depressivity’ (Arens et al., 2013) and are more likely than those without BPD to suffer from co-occurring major depressive disorder (MDD) and/or dysthymia (Avari et al., 2011; Devanand et al., 2000). In their study of community residents in Germany, Arens and colleagues found a significant increase in ‘depressivity’ in association with ageing, with ‘depressivity’ scores increasing markedly from the 46–65 cohort to those aged over 65 years. The importance of depressive symptoms in BPD is illustrated by a 27-year follow-up of a cohort of 64 BPD patients by Paris and Zweig-Frank (2001), who reported substantial overall improvement in BPD symptoms over time in patients whose mean age at follow-up was 51 years. However, patients meeting diagnostic criteria for dysthymia on the Structured Clinical Interview for DSM-IV (SCID) had poorer outcomes on all measures at follow-up. Thus, ‘depressivity’, whether expressed as MDD or dysthymia, appears to be associated with slower remission of BPD symptoms and, importantly, may be predictive of the persistence of BPD into older age. This is supported by a recent study by Galione and Oltmanns (2013), who evaluated a community-based population of 1630 people aged between 55 and 64 years. Their major finding was that a history of major depression was related to stable temperamental symptoms of ‘depressivity’ and distress even in those with sub-syndromal BPD.
Taken together, the growing literature describing these phenomenological factors conforms to clinical impression that impulsive behaviours defined by acting out – risk-taking behaviours, substance abuse and DSH of the kind seen in younger adults with BPD – are not major features of BPD in old age (Trappler and Backfield, 2001). However, acts of DSH usually seen in younger patients, and those more common in the elderly, can occur in response to psychosocial stressors, particularly if support and coping skills are lacking (Avari et al., 2011; see Table 1). Suicidal threats are common, whereas suicidal gestures are much less so. It is notable, however, that although infrequent, suicide attempts in elderly patients with BPD tend to be serious and life-threatening (Sadavoy, 1996). These findings are summarized in Table 2.
Forms of self-harm in the elderly with BPD.
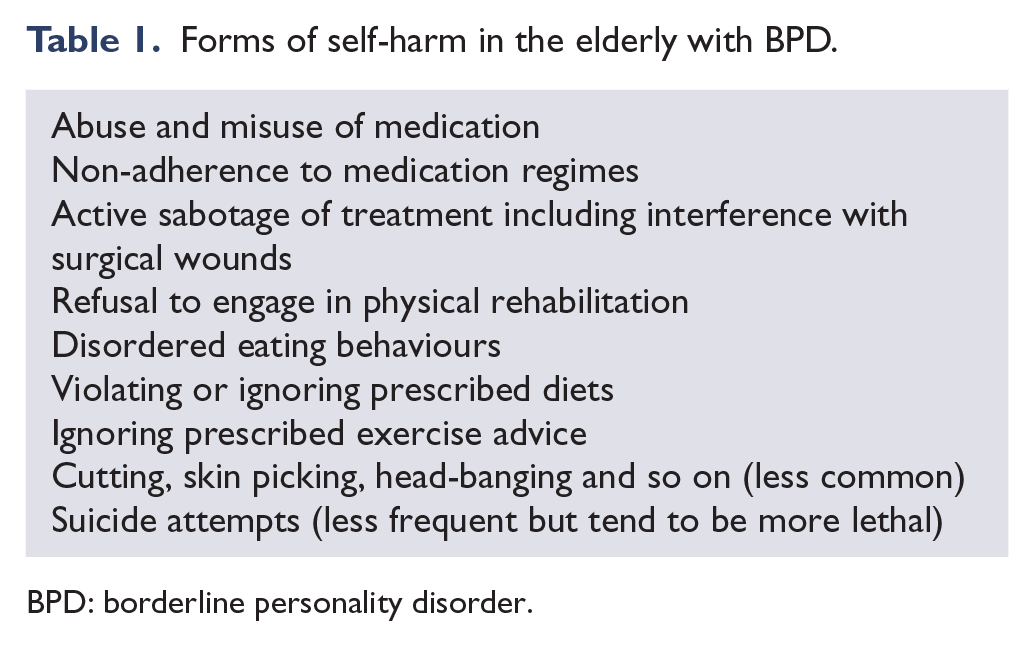
BPD: borderline personality disorder.
Phenomenology of BPD in old age compared with younger adults.
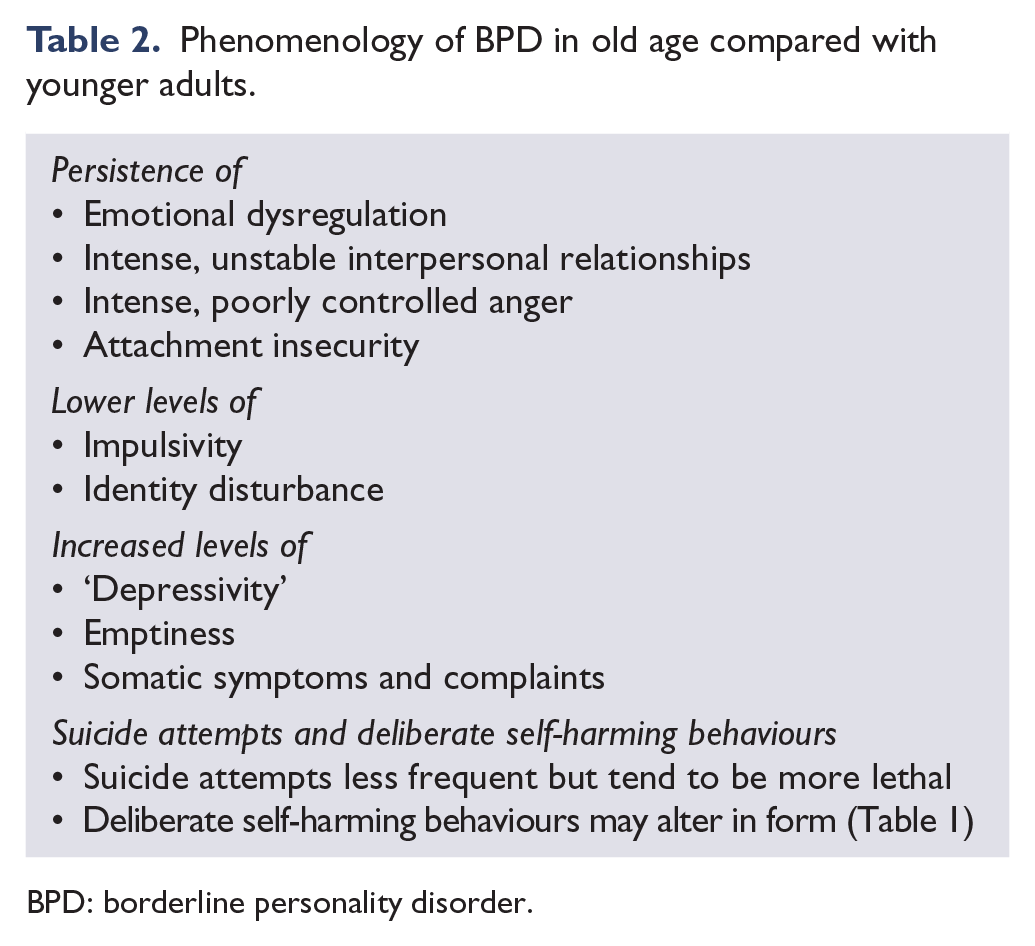
BPD: borderline personality disorder.
The frequent use of somatization by older patients is often expressed in dramatic and frequent demands for medical attention (Arens et al., 2013; Sansone et al., 2013; Trappler and Backfield, 2001). Trappler and Backfield (2001) used detailed case histories to describe the clinical characteristics of three older inpatients with BPD. They noted that somatization-associated therapeutic, medical and psychopharmacological interventions can lead to prolonged admissions and undermining of personal and professional boundaries, both of which are accompanied by intense and negative countertransferential reactions in staff.
Another stable BPD factor in the elderly is the continuation of extremes of idealization and devaluation in their relationships, including those with healthcare providers (Sadavoy, 1996). Not surprisingly, the instability and intensity of relationships between BPD patients and staff in inpatient or nursing care facilities are a major cause of management difficulties. Sadavoy (1996) proposed that identity disturbance in the elderly manifests differently than in younger adults, expressed instead as regrets about life choices concerning spouse, career, values and parenthood. Hall et al. (2012) provide two case vignettes that outline the difficulties posed by elderly patients with BPD in residential care facilities. Their account is striking for its similarity to the clinical experience of the authors of this paper, with repeated complaints about nursing care, hostility, refusal to comply with treatment, complaints about lack of care and attention from family members, escalating demands for medication, frequent mood changes, emotional outbursts, extremes of idealization and devaluation, difficulties with abandonment, difficulties maintaining close relationships and negative countertransferences.
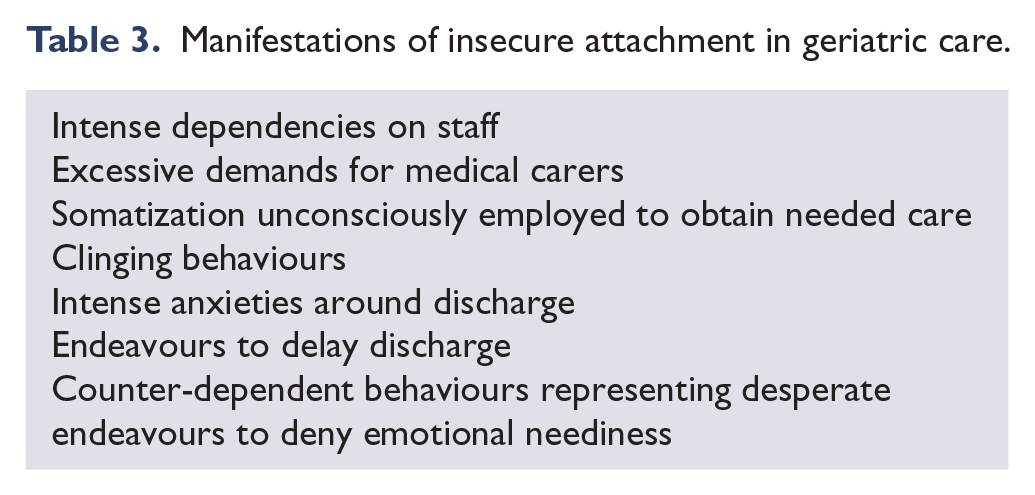
Disturbed attachments in association with difficulties in mentalizing are fundamental to the clinical manifestations of BPD (Fonagy and Bateman, 2008). Fossati et al. (2012), in their community study of 1192 non-clinical participants, identified predictors of BPD across four age ranges. Attachment scores were significant predictors of BPD features across all age groups, although different scales were relevant in different age groups. In patients over 50 years, insecure attachment accompanied by preoccupation with relationships was a significant predictor of BPD features. This may be expressed in a range of maladaptive ways (Table 3).
Manifestations of insecure attachment in geriatric care.
The late-life re-emergence of symptoms and behavioural characteristics of BPD, after lying dormant or being less apparent in middle age, was foreshadowed by Stone (1994, 2001) and more recently by Shea et al. (2009). Both noted the potential for an age-related reversal of improvement in functioning in some patients, often in the context of stressful life events in later life. These findings conform to a growing clinical awareness of a subset of patients with BPD who improve in middle age (many no longer meeting DSM-IV diagnostic criteria for BPD) and then relapse as they age. The clinical and research challenge is to identify the characteristics of this group.
Diagnosis of BPD in the aged population
Although many articles attest to the difficulties of diagnosis and assessment of PDs including BPD in the elderly (Abrams and Bromberg, 2006, 2007; Molinari et al., 1994; Morgan et al., 2013; Newton-Howes et al., 2015; Oltmanns and Balsis, 2011; Richa and Ibrahim, 2012; Rosowsky and Gurian, 1991; Segal et al., 1996; Zweig, 2008), no diagnostic or rating instruments have been developed specifically for use in this population. As discussed above, diagnostic instruments developed for the general adult population are not suitable in the elderly because several criteria for PDs in general and for BPD in particular no longer apply (Abrams and Bromberg, 2006, 2007; Agronin and Maletta, 2001; Molinari et al., 1994; Morgan et al., 2013; Oltmanns and Balsis, 2011; Richa and Ibrahim, 2012; Rosowsky and Gurian, 1991; Sadavoy, 1996; Segal et al., 1996; Trappler and Backfield, 2001; Zweig, 2008). The perception of BPD as a young person’s diagnosis likely contributes to its under-diagnosis in aged patients. The 1996 review by Segal et al. regarding the diagnosis and assessment of PDs in older adults stated that ‘DSM diagnostic criteria may be inadequate for older individuals given the unique physical, cognitive and social complications encountered by this segment of society’ (p. 394). Despite this early insight, little progress has occurred in the development of validated clinical assessment tools for BPD in old age.
The problem of diagnosis is captured in the following examples. Molinari et al. (1994) gave the Structured Interview for Disorders of Personality–Revised (SIDP-R) to 200 inpatients in old age psychiatric facilities. Use of the SIDP-R showed a prevalence of PDs of 56.5%. By contrast, psychiatrists gave far fewer Axis II diagnoses than were detected using the SIDP-R, particularly for female patients. With respect to BPD diagnosis in particular, Molinari et al. (1994) found that psychiatrists identified only 3 patients, whereas the SIDP-R identified 13. Similarly, Rosowsky and Gurian (1991) analysed the records of eight elderly patients (aged 64–85 years) who had been diagnosed with BPD by experienced clinicians. However, in contrast to the previous example, neither the Revised Diagnostic Interview for Borderlines (DIB-R) (Zanarini et al., 1989) nor the use of the DSM-111-R criteria for BPD (American Psychiatric Association [APA], 1987) identified any patient as having BPD. Lowering the diagnostic cut-off scores for each measure increased sensitivity somewhat, but it was clear that neither instrument reflected the key symptoms of BPD in the aged.
A recent Australian study (Stevenson et al., 2011) reported a 58.8% prevalence of PD in 98 psychiatric inpatients aged over 65 years using SCID Axis I and II (SCID-I and SCID-II). Notably, psychiatrists detected PD in only 19.8%. Ullrich and Coid (2009) have commented on the reluctance of psychiatrists to attribute maladaptive personality traits or disorder to elderly patients. Several factors, including the lack of a longitudinal history that would help confirm the presence of maladaptive traits over the life span, lack of patient cooperation with history-taking and lack of collaborative information from friends and family because of the individual’s social isolation, can hamper diagnosis. Fear of misattributing PD to a patient when neurodegenerative changes may affect presentation, in addition to anxiety about pejorative effects that a diagnosis of PD may have on patient, staff, and family, may also be factors. The presence of PD, including BPD, may not be considered when co-occurring or co-morbid disorders take centre stage on initial presentation (Segal et al., 1996; Stevenson et al., 2011). Given the limited awareness of BPD across mental health systems more broadly, the absence of key symptoms of BPD in the presentation of elderly patients compounds the problem of achieving accurate and timely diagnosis.
Discussion
Mounting evidence that failures and delays in diagnosing PD, including BPD, adversely affect patients and staff in old age inpatient services is borne out by clinical experience. The literature clearly describes the persistence of features of BPD into old age in some cases, with its associated symptoms and behaviours resulting in significant management difficulties. BPD features may also emerge for the first time in old age (see Table 2). This might occur after the loss of a ‘containing relationship’ or of a role that provided a ‘holding function’ sufficient to cover significant personality difficulties. Chronic interpersonal difficulties mean that many of these patients are estranged from family and friends and lack current intimate relationships. Hostile, angry behaviours are common, as are prominent somatic symptoms and demands for medical attention. Patterns of idealization and devaluation of staff persist into old age and can create havoc in facilities unused to dealing with them. Attachment insecurity and fears of abandonment are revealed by endeavours to prevent or delay discharge from hospital and rehabilitation environments. Conflicts around dependency may be revealed by help-rejecting behaviour. Self-harm typical of younger patients is sometimes seen in the elderly, but atypical self-harming behaviours occur more frequently (see Table 1), often representing attempts to delay discharge from inpatient care. Negative countertransferences evoked in staff towards these patients are characteristic in relation to BPD (Betan et al., 2005). Staff in geriatric residential facilities, including psychiatric facilities, often lack education about PDs, their phenomenology, treatment and nursing care. The introduction of educational programs that increase empathy for the intense suffering of these patients would decrease the likelihood of iatrogenic damage or treatment breakdown that can otherwise occur.
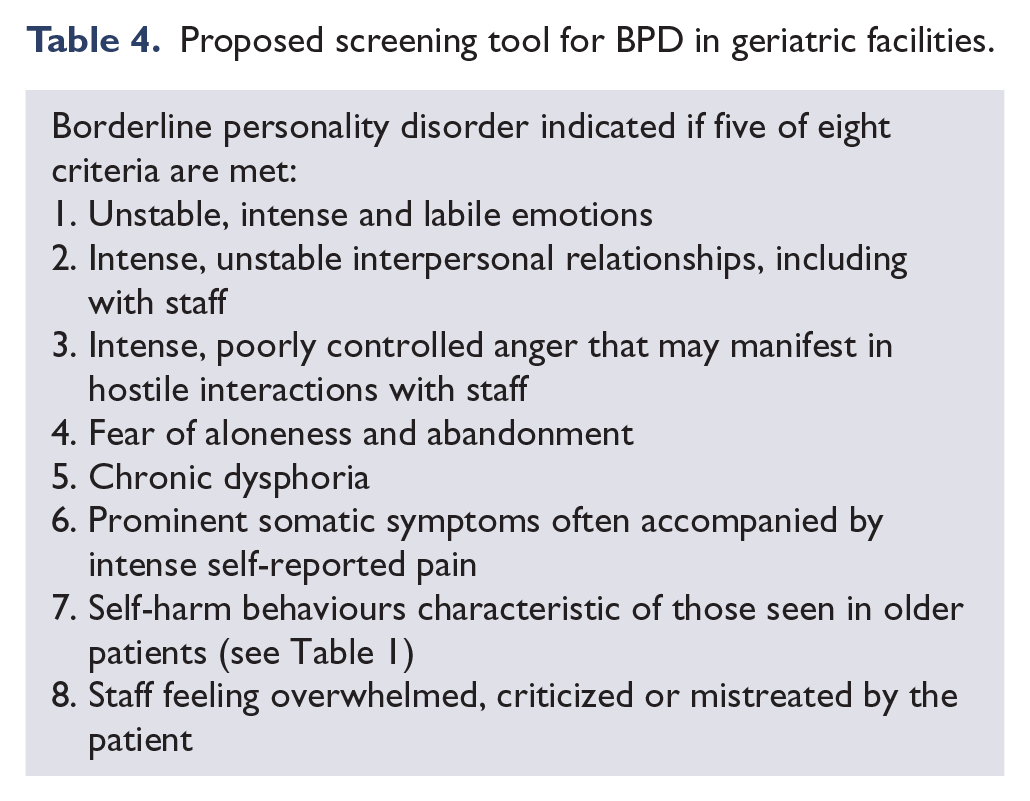
There is sufficient evidence in the literature and from clinical experience to suggest that patients in old age facilities manifesting some combination of the characteristics described in Tables 1–3 could benefit from psychiatric consultation early in the course of admission (see Table 4). When, in addition to these characteristics, there is a longitudinal history of difficulties in interpersonal relationships, lack of social contacts, abandonment fears or counter-dependent behaviours, the likelihood of PD, particularly BPD, is heightened. The authors of this review suggest that the presence of five of the eight criteria listed in Table 4 could be used as a screening tool for BPD in old age to assist in determining when to request psychiatric assessment in aged care facilities. The first five criteria represent core features of BPD in the elderly; criteria 6 and 7 represent the most prominent symptoms reported in older adults; criterion 8 refers to staff feelings most commonly reported in the face of repeated maladaptive behaviours of these patients. These criteria could be provisionally employed as diagnostic pointers for BPD in the elderly, while research is conducted to evaluate their sensitivity and specificity.
Proposed screening tool for BPD in geriatric facilities.
With the large ageing population, there will be greater numbers of people with BPD and other PDs, resulting in an increased burden of the disorder in both outpatient and inpatient settings. Careful study is required to elucidate the symptomatology, phenomenology, co-morbidities, attachment patterns, trauma history and family history of patients who fail to sustain remission, fail to remit, relapse from previously achieved recovery from BPD or manifest features of BPD for the first time in old age. The ongoing difficulties of patients who continue to struggle with BPD or have it recur in old age are profound. The timely identification of these patients is urgently needed so that they can receive the skilled help, understanding and treatment for BPD needed to alleviate their suffering in the twilight of their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.