
Abstract

To the Editor
We describe a case of severe depression with comorbid anxiety which quickly remitted following low-intensity cognitive behavioural therapy (LiCBT) delivered by novice coach. ‘SR’, an elderly male, presented to NewAccess, a LiCBT service based on the United Kingdom’s Improving Access to Psychological Therapies programme (www.iapt.nhs.uk/about-iapt/). Coaches without formal mental health qualifications initially undertake 6 weeks’ LiCBT training, followed by 1 year’s supervised practice (by qualified CBT practitioner). NewAccess ensures treatment fidelity by only treating common mental health problems (anxiety; depression) using highly structured LiCBT. SR was coach BK’s first client following training. SR gave informed consent (following institutional review board [IRB] ethics approval) to participate in the research.
SR presented with severe depression, suicidal ideation and severe comorbid anxiety. SR disclosed an adolescent suicide attempt and expressed current generalised suicidal ideation without detailed plans. Concordant with NewAccess procedure, BK elicited protective factors, provided crisis support information and reviewed risk every session.
SR was offered in situ or telephone treatment. SR consented to in situ workbook-supplemented LiCBT treating his depression using Behavioural Activation (Martell et al., 2001). Assessment and initial treatment sessions were supervised in situ, with subsequent weekly supervision delivered remotely. Figure 1 shows large reductions in SR’s depression severity (Cohen’s d = 8.68, Percentage of Non-Overlapping Data (PND) = 100 1 ), anxiety severity (d = 7.22, PND = 100 [see Note 1]) and functional impairment (d = 2.27, PND = 67 [see Note 1]) over five treatment sessions. Psychological distress also reduced (see Note 1). At treatment completion, SR’s symptoms were subclinical and lacking suicidal ideation. Despite BK targeting depression, treatment gains generalised to SR’s comorbid anxiety. At follow-up, SR was in full remission. SR expressed satisfaction with the service.
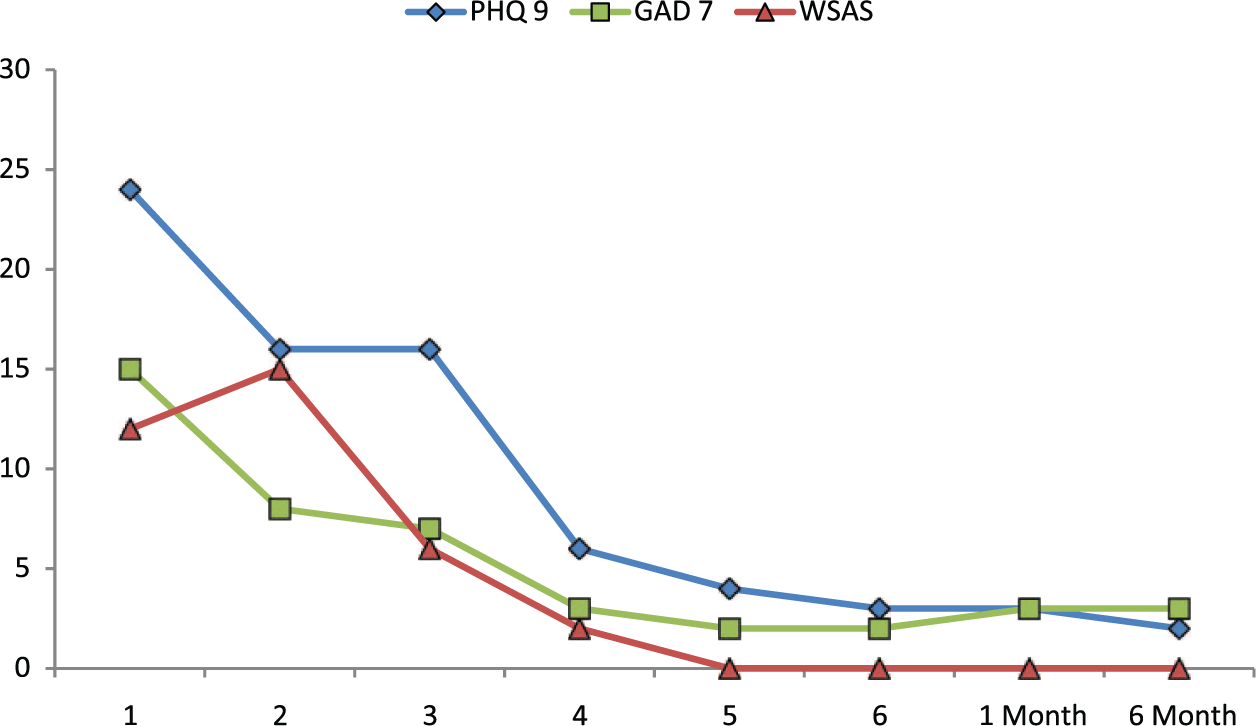
SR’s depression, anxiety (PHQ-9, GAD-7; Löwe et al., 2008) and functional impairment (WSAS; Mundt et al., 2002) scores from assessment to 6-month follow-up (see Note 1).
Cases like SR’s are typically treated by mental health professionals with extensive training. As full remission is ideal, SR’s case demonstrates that LiCBT delivered by novice coach can be effective for severe depression and anxiety. Creating a new workforce of LiCBT coaches could act as an early intervention service, and free highly qualified mental health professionals to treat complex cases where LiCBT is less effective. SR’s case suggests that Australian LiCBT programmes are effective, acceptable to service users and may help reduce untreated depression and anxiety.
Footnotes
Acknowledgements
We thank beyondblue and the North Coast Primary Health Network for their support in the development of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The not-for-profit organisations beyondblue and Movember are funders of the NewAccess programme.