
Abstract

To the Editor
Ryde Community Mental Health Service is a busy centre, catering for a large number of people with a chronic mental illness. At any one time, about 170 patients with a diagnosis of treatment resistant schizophrenia are being treated with the antipsychotic clozapine. In the last 11 years, at Ryde, 5 out of a total of 221 patients taking clozapine have developed lymphoma. There are also reports of cases at other centres.
The lymphomas have been of varying types: two Burkitt’s lymphomas, two non-Hodgkin’s lymphomas (NHLs), and one follicular NHL (Table 1). All five patients were treated for their lymphomas at local public hospitals and were able to continue taking their clozapine throughout their treatment, in consultation with the clozapine haematologist.
Patient ages at the start of clozapine and onset lymphoma.
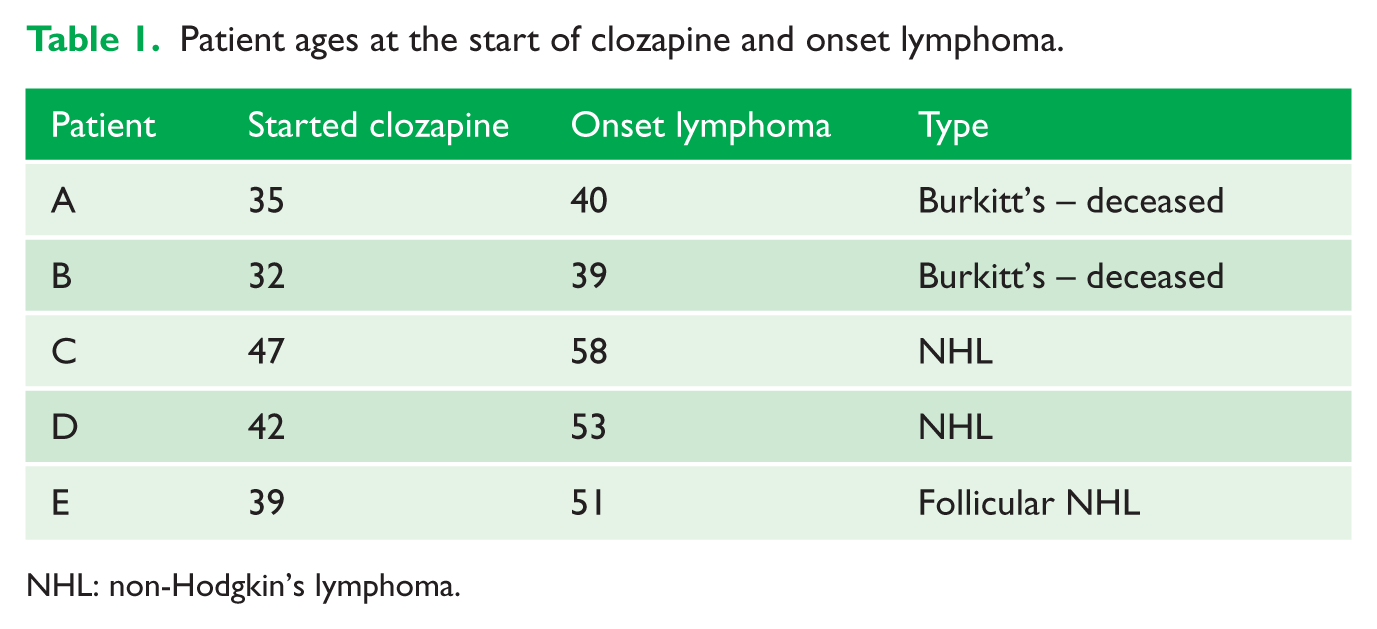
NHL: non-Hodgkin’s lymphoma.
The two members of the group with Burkitt’s lymphoma died. The remaining three NHLs continue to receive treatment.
According to the Cancer Institute of New South Wales (NSW), the lifetime incidence of NHL up to age 85 is 1/42, which is common. However, the three NHLs occurred between ages 51 and 59. The incidence of Burkitt’s lymphoma is about 1% of all NHL, that is, 1/4200.
After contacting the Adverse Drug Reactions Advisory Committee (ADRAC) in Canberra, their Signals Investigation Unit did a search on this topic. They reported that crude reporting rates for lymphoma associated with clozapine use across Australia are in keeping with estimated background population incidence – except for the Ryde cluster.
A literature search shows a number of individual case reports, mainly relating to continuing clozapine through chemotherapy (Ali et al., 2014; Munshi et al., 2013). One 2010 report from Denmark questions a link between clozapine and acute myelocytic leukaemia, based on a register search showing 4/3779 cases and concluding an eight-fold increased risk. (Nielsen and Boysen, 2010)
The question is whether the Ryde cluster is simply a coincidence, or whether there might be a trend, but general under-reporting by doctors who do not see a connection. In public hospitals and community centres, many clozapine patients are treated by registrars on 6-month rotations, leading to non-continuity of the observer.
The purpose of this letter is to raise awareness and the index of suspicion, and report to ADRAC any cases of patients developing lymphoma while being treated with clozapine.
Footnotes
Acknowledgements
I am grateful for the support and assistance of Dr Luke Coyle, consultant haematologist at Royal North Shore Hospital in the Northern Sydney LHD.
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.