
Abstract
Objective:
People with bipolar disorder frequently have persistent symptoms, continued problems functioning and comorbid medical conditions. We propose applying the athletic coaching concept of marginal gains to help patients address these challenges to achieve wellness.
Method:
We review the concept of marginal gains and potential interventions to improve long-term outcomes for bipolar patients.
Results:
Evidence exists to help bipolar patients with diet and exercise, gradual behavioral change, mobile applications and peer support.
Conclusion:
Marginal gains, small and doable improvements across a broad range of areas, have great potential to improve the lives of people with bipolar disorder.
Introduction
Bipolar disorder is a lifelong waxing and waning psychiatric condition with a challenging and burdensome course for many patients. Despite modern guideline-concordant and evidence-based pharmacotherapy and psychotherapy, only about 20–30% of patients achieve sustained wellness (Perlis et al., 2006), while others experience fluctuating dysregulations in their mood, sleep, anxiety and ability to function. Thus, it is imperative that we identify strategies and treatments that, in aggregate, can change the course of bipolar disorder and increase the probability of wellness. The purpose of this paper is to introduce the athletic coaching concept of marginal changes to improve the course of bipolar disorder.
Marginal gains
It is difficult for people to make positive lifestyle changes. For example, a large proportion of the population struggles with their weight and try endless diets to no avail. Making positive lifestyle changes is even more challenging for those diagnosed with bipolar disorder. We propose to take a lesson about training from a professional cycling team originally designed to improve athletic performance at the highest levels and apply these lessons to help our bipolar patients achieve wellness and improve over time (Team Sky, 2010).
Sir David Brailsford, the British Cycling’s performance director, was asked to help Team Sky (Great Britain’s premier professional cycling team) win the Tour de France (Team Sky, 2010). Brailsford realized that because it was essential for his team to refrain from doping and ride ‘clean’, he would have to find legitimate methods to improve the performance of his cyclists. He decided to decompose every aspect of cycling and improve each one by 1%, a marginal improvement. Over time, while it might not immediately be apparent, each 1% improvement would eventually add up to a significant advantage. In contrast, a 1% negative change in each area could lead to a significant disadvantage (Clear, 2014). Thus, he implemented a wide variety of small changes including improving the nutrition of the riders; the ergonomics of the bike seat (Clear, 2014); the pillow, sheets and mattresses while traveling; their sleeping position (Slater, 2012); their clothing (Team Sky, 2010); the comfort of the bus and even implemented hand washing techniques used by surgeons to avoid getting or spreading infections (Durrand et al., 2014).
Sir Brailsford expected that these changes would result in substantial improvements within 5 years. Remarkably, he needed to only wait 3 years, as Team Sky won 70% of all track cycling gold medals in 2012 London Olympics as well as winning three Tour de France competitions (Clear, 2014).
This concept of marginal gains seems to be a natural fit for bipolar disorder given the challenges of this population, like many serious mental health conditions, to make lifestyle changes. An example of the aggregation of marginal gains in health care was demonstrated by the National Enhanced Recovery Partnership (NHS Improving Quality, 2013). This partnership carefully studied the pre-operative process and broke it into seven phases. They designated potential small changes to each phase, from primary care and the period before admission to the process of transferring to home/community and the follow-up. Some outcomes could be noticed with the initial implementation, such as improved patient experience and length of hospital stay. Furthermore, some authors propose the implementation of marginal gains in the operative pre-habilitation, by identifying factors that could lead to a worse prognostic or a higher operative risk, like anemia, smoking and individual medications, starting from elective surgery toward the big challenge of emergency cases (Durrand et al., 2014). Indeed, they believe that Team Sky’s approach can be feasible and effective for improving clinical and surgical practice.
We propose that sustained marginal gains can have a substantial aggregated positive impact for the treatment for bipolar over time for two reasons. First, individuals with bipolar disorder have a tendency to make small, negative changes over time that lead to poorer outcomes. For example, bipolar patients have increased rates of risk factors for cardiovascular disease, such as obesity, dyslipidemia and metabolic syndrome which is associated with sedentary behavior, such as TV watching (Gomes et al., 2013; Kaur, 2014). It is easy to add 30 minutes of TV watching a day when depressed. This would translate into 15 hours of sedentary behavior a month or 180 hours a year. This is further supported by Health Belief model (Rosenstock, 1974). This model posits that behavioral change should occur when one understands the perceived susceptibility (e.g. comorbid obesity) and perceived benefit of making the behavioral change (e.g. exercising), but that perceived barriers (e.g. fatigue, depression) and self-efficacy (e.g. competence to successfully do the behavior) can get in the way. Thus, making extremely small or seemingly unnoticeable changes as suggested by the marginal gains theory may help to overcome these perceived barriers and enhance self-efficacy that the changes can be made.
Second, given the illness severity of bipolar disorder, it is likely more challenging for them than others to make lifestyle changes (as posited by the Health Belief Model), and thus, they could greatly benefit from identifying very small positive and doable changes (Sylvia et al., 2013). Figure 1 illustrates these two scenarios, or the power of marginal losses over time as well as the power of aggregated marginal gains. This is perhaps not surprising as the theory of marginal gains mimics what may be considered common knowledge among behaviorists that smaller changes made over time can be much less overwhelming than making fewer, larger changes (Snyder and Cunningham, 1975). However, theories of persuasion caution us that it may not be that simple. For example, the elaboration likelihood model (Cacioppo and Petty, 1984) highlights that a person will only be persuaded to change if (1) they are highly motivated to receive the information about change and (2) they are able to cognitively process the information. These may both present challenges for individuals with bipolar disorder.
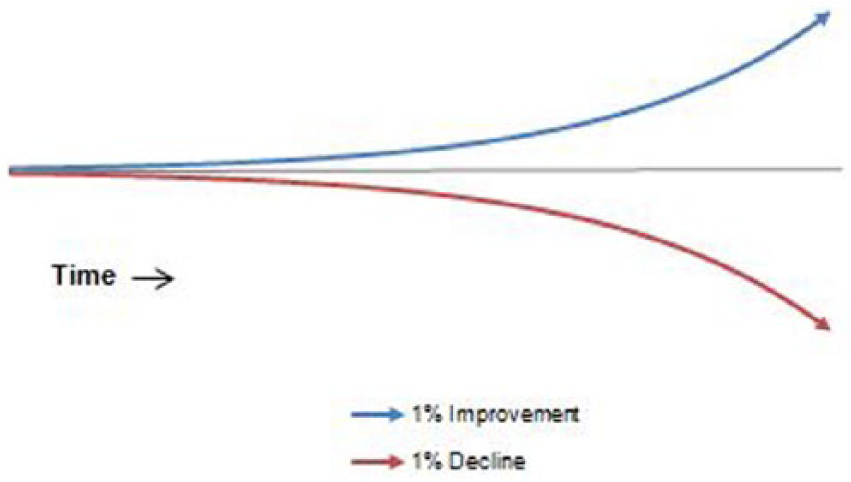
Aggregation of marginal gains and losses over time.
To further illustrate this point, consider a bipolar patient going to a physician’s office to seek help. It is not uncommon that the patient returns home from this appointment with a list of doctor’s recommendations (e.g. lose weight, increase social support, exercise more and attend work regularly). These recommendations may be so overwhelming that the patient not only gives up on trying to make improvements but also actually begins to slip in doing the positive things that were already being done. Thus, instead of being on the path to marginal gains, they are on the path to marginal losses with a slow deterioration in outcomes (see Figure 1). Thus, the key with marginal gains is persisting in making almost imperceptible changes so that the perceived barriers are low and self-efficacy is sufficiently high.
Method
We selected pertinent articles supporting the idea of marginal gains and behavioral change from peer-reviewed journals. We will (1) outline the small and achievable changes that bipolar patients can make, following the example of Team Sky and (2) offer some suggestions on how to get bipolar patients to make such changes. We propose that following the example of Team Sky that identifies areas for 1% improvement, patients can move toward wellness. The challenge is to help patients persist with small changes that result in imperceptible improvements. Persistence with marginal gains can lead to results over time and is worthy of clinical investigation. Thus, we need to decompose tasks for patients with bipolar disorder, just as Sir Brailsford did for the Team Sky, into small, acceptable and easy to achieve changes.
Results
Marginal gains for bipolar disorder
Gradual behavioral change
Consistent with the Health Belief model of behavioral change, perceived barriers must be eliminated and self-efficacy to accomplish the changes must be high. Thus, we propose that there are three steps to making marginal improvement gains: (1) accept that change is needed, (2) find the motivation to change and (3) problem-solving obstacles in the way of making change (Prochaska et al., 1994). We will discuss each of these steps of gradual behavioral change in turn as well as provide several tools to overcoming perceived barriers (e.g. lack of time, bored, too difficult and negative thoughts).
Acceptance and dialectical behavioral therapy
Acceptance of one’s reality is the first step in making behavioral change. Acceptance is being aware of the present moment or objectively observing one’s current reality (Linehan, 1993). For example, acknowledging that you are overweight, your current reality, is necessary in order to make changes to help you lose weight. Unfortunately, acceptance is not straightforward. Often individuals, especially bipolar individuals, believe that they have accepted their reality (e.g. ‘I know that I can no longer fit into my clothes’, ‘I know that I am fat’), but instead they are judging their current reality opposed to objectively seeing it. Thus, an important concept of truly accepting one’s reality is to not judge it. This is also important in making behavioral changes as judging, or lack of acceptance, can cause people to become stuck or unwilling to change.
Dialectical behavioral therapy (DBT) offers excellent advice and strategies to help individuals practice ‘radical acceptance’ (Linehan, 1993). Radical acceptance refers to a core principle of DBT, which is accepting oneself as he or she is while concurrently working toward changing maladaptive behaviors. For example, DBT has a strong emphasis on reducing suicidal behavior. To accomplish this, the therapist validates the patient’s current emotions and cognitive beliefs while simultaneously trying to ‘reframe’ problems so that the individual can add them to their problem-solving repertoire. In this way, by approaching one aspect of a larger problem, it is possible for the patient to improve functioning (Linehan, 1993). Thus, DBT can be very helpful in moving individuals with bipolar disorder toward making 1% changes by letting them see their reality and accept it non-judgmentally.
Motivation and motivational interviewing
Motivational interviewing (MI) is a counseling method originally developed to help individuals reduce substance use, but has been applied more generally to patients tending to lack motivation, such as bipolar disorder. The goal of MI is to build an individual’s intrinsic motivation to change by helping them explore and resolve ambivalence (Miller and Rollnick, 2002). As theories of persuasion highlight (i.e. elaboration likelihood model), motivation is central to making changes. MI is a client-centered, non-confrontational way to help people understand why it may be in their best interest to make gradual changes. MI is based on stages of change (Prochaska et al., 1994; see Table 1, outlining the change process), highlighting that not everyone is necessarily ready to make behavioral changes. The first stage, precontemplation, is usually associated with the lack of acceptance, illustrating the importance of acceptance as the first step toward making gradual behavioral changes.
Stages of change.
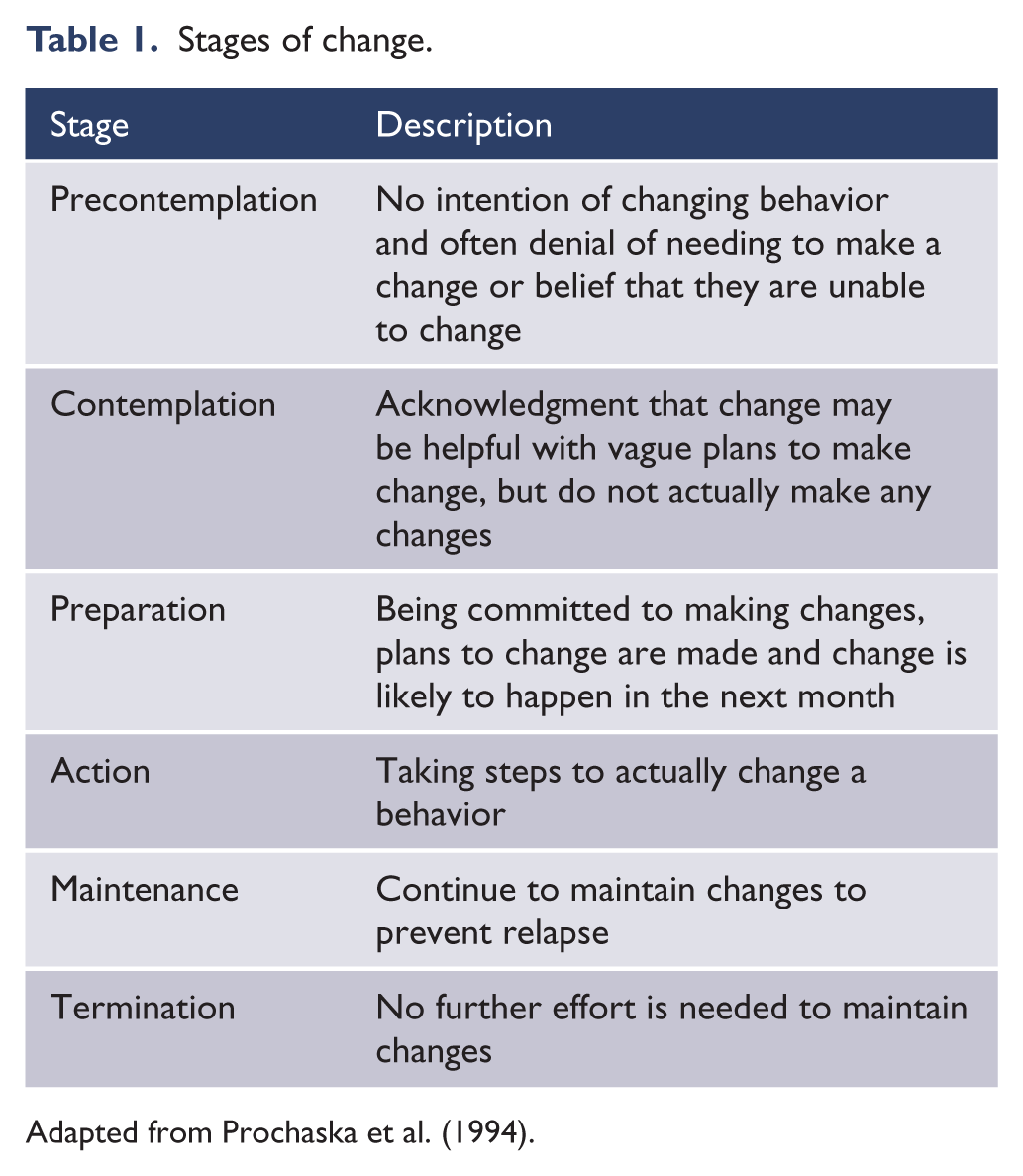
Adapted from Prochaska et al. (1994).
MI can help bipolar individuals move through these change stages and benefit from aggregation of marginal gains. MI does this by eliciting change talk and highlighting how current behaviors may not be working. This follows Fisher’s narrative paradigm of persuasion, or that people prefer a narrative of ‘good reasons’ or a good story for making change (e.g. examples of others making lifestyle changes) opposed to simply rational facts (Fisher, 1984, 1987). For example, some questions to stimulate these discussions are ‘How might you like things to be different?’ or ‘How does your current diet interfere with things that you would like to do?’. Importantly, and as highlighted by the health belief model, knowledge alone, or psychoeducation about nutrition and bipolar disorder, is usually not sufficient to motivate change within a client, and challenges in maintaining change should be thought of as the rule, not the exception. The concept of making gradual changes is vital as small, focused and realistic goals are the cornerstones to MI promoting this change process (Freedman and Combs, 1996). There have been many studies highlighting the positive impact of MI. Specifically, 74% of randomized clinical trials using MI found it effective in making behavioral changes (Rubak et al., 2005). MI has also been shown to double adherence rates to treatment in individuals with mood disorders (Swanson et al., 1999). In sum, only by acknowledging the need to change, accepting their current reality and finding the motivation to change can bipolar patients make 1% gradual changes.
Making marginal changes with cognitive behavioral therapy
Cognitive behavioral therapy (CBT) hopes to move people through these stages of change, to obtain marginal gains, by identifying and changing one’s dysfunctional belief system and associated distorted thoughts. An awareness or willingness to see that one’s thoughts are distorted or not entirely accurate is needed to create incentive to change beliefs and thoughts. Thus, acceptance is usually an important first step in practicing CBT. CBT can be a powerful therapeutic style in enhancing change (Sylvia et al., 2009). CBT also includes elements similar to other psychosocial interventions such as increasing patients’ understanding of the treatment and management of bipolar disorder (i.e. identify triggers to episodes, mood monitoring), medication adherence and lifestyle regularity (Basco et al., 2007).
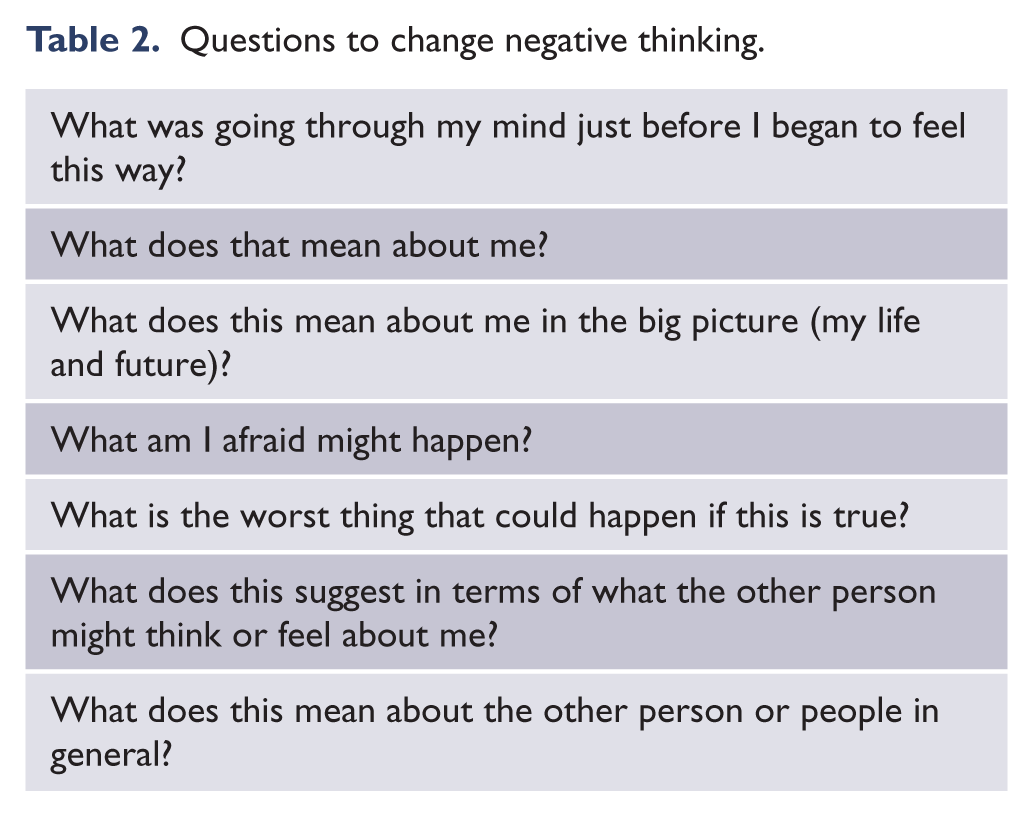
CBT posits that people can alter their experience of reality by reformulating thoughts, a common obstacle to making behavioral changes. Changing thoughts involves changing deep-rooted patterns of thinking that affect many aspects of life. The first step in changing negative thinking is identifying one’s negative thoughts. Dr. Judy Beck suggested a list of questions to help an individual generate their negative (often distorted or inaccurate) thoughts (Table 2; Beck, 1995). The second step to changing one’s thinking is to identify alternative or more rational, balanced thoughts. The power of this skill is tremendous as changing one negative thought a week (perhaps a 1% marginal change) could lead to a new pattern of more positive thinking.
Questions to change negative thinking.
CBT has proven to be an effective treatment strategy for bipolar disorder. A randomized controlled study (Lam et al., 2003) found that changing negative thinking patterns lead to fewer manic, depressive and mixed episodes for individuals with bipolar disorder. CBT has helped bipolar patients make 1% (and greater) changes with sleep, a key component of mood stability in bipolar disorder (Leibenluft et al., 1996). Thus, CBT can help bipolar patients make marginal gains, greatly impacting symptoms and functioning.
Making marginal changes with coaching
Individuals seeking to make behavioral changes may also benefit from coaching. A coach helps people define realistic goals to improve functioning. In the coaching relationship, the coach often acts as an expert giving advice in a specific field. In other instances, the coach acts more as a support system to help motivate and empower the individual seeking help (Cavanagh, 2005).
Grant (2005) states that an assumption in the coaching relationship is that the individual seeking help is not experiencing serious emotional distress or psychopathology, as coaches are often not trained to manage severe pathology. However, coaching may still benefit higher functioning or more stable individuals with bipolar. The emphasis on goal setting and staying focused on making specific changes can be very beneficial (Cavanagh, 2005). For example, if an individual with bipolar disorder saw a workplace coach, this coach may be particularly suited to improve workplace functioning. Attending work more steadily could be an important 1% gain for bipolar patients as it could improve job security, increase regularity of one’s day (which buffers against bipolar episodes) or improve social relationships (Shen et al., 2008).
While coaching may help individuals make small improvements and set goals, it is often not covered by insurance and thus may not be the most feasible option for bipolar patients. Additionally, many coaches are instructed to refer individuals with psychopathology to other treatment programs and therapists (Cavanagh, 2005), making it less likely that an individual with bipolar disorder would participate in long-term coaching. However, when considering behavioral change, it is an option.
Making marginal changes with phone and web applications
Many Americans use phone applications, and thus applications designed to improve well-being and mood could be highly accessible effective tools to help bipolar patients make gradual changes. Consistent with the health belief model, phone applications could help to increase self-efficacy by giving patients an easy way to track changes on their own as well as reduce perceived barriers by giving a tool with immediate feedback and information on behavioral change. For example, phone applications help individuals track mood, anxiety, sleep, medications taken, diet and exercise. For example, ‘BeWell’ is an automated well-being application that presents information in an accessible user-friendly way and helps patients monitor and track changes in sleep, exercise and social interaction. BeWell is appealing because it does not require user data entry, but instead uses accelerometers, microphones and global positioning system (GPS) to provide information about user well-being (Lane et al., 2011).
Applications are also being developed to provide treatment recommendations. MONARCA is a phone application designed for the monitoring and maintenance of bipolar disorder. Specifically, it uses information from cell phone towers to estimate activity levels and time spent outside the house, which it then correlates with Hamilton Depression Rating Scale (Faurholt-Jepsen et al., 2013). MONARCA breaks down patient symptoms into categories of improvements made and can subsequently help patients track progress in manageable increments (Faurholt-Jepsen et al., 2013). Users enter data on activity levels and mood on a scale from −3 to +3, on sleep as number of hours per night and other variables, such as irritability, alcohol consumption and cognitive function, among others, are entered in a yes/no format. MONARCA allows patients to visualize data entered within the past month to create short-term goals that can build off of previously made progress. Additionally, if certain data are entered, the application shows the patient personalized suggestions. For example, if a user reported sleeping less than 6 hours a night for three consecutive nights, the suggestion might be to sleep in a cold, dark room. In a trial of 12 individuals with bipolar disorder using MONARCA for 14 weeks, individuals reported that MONARCA improved their awareness and disease management (Faurholt-Jepsen et al., 2013).Thus, MONARCA may help improve awareness and provide visualizations of progress collected from daily assessments (Faurholt-Jepsen et al., 2013).
In a study of a mobile self-monitoring program, Mobile Tracking of Young People’s Experiences, using the program for 2–4 weeks led to increased emotional self-awareness (Kauer et al., 2012). This study looked at 118 adolescents and young adults aged 14–24 years with mild to severe mental health concerns. Individuals using the application recorded data on eight areas of functioning, including activities, mood, quality and quantity of sleep and exercise, emotional self-awareness, depression and anxiety symptoms, mood, alcohol and cannabis use and stress. A control group entered data in an abbreviated form of the program that excluded emotional self-awareness, depression and anxiety symptoms, mood, alcohol and cannabis use and stress. Another study found that a 6-week web program, called MoodGYM, significantly improved dysfunctional thinking and increased knowledge of effective psychological tools (Christensen et al., 2004). MoodGYM comprises interactive modules, including anxiety and depression assessments, relaxation audio files, quizzes and homework assignments. Thus, phone applications could help increase emotional self-awareness in a manageable, easily accessible manner. Moreover, these data were automatically uploaded in a format accessible to the user’s doctor, therefore facilitating communication between patient and doctor. In a similar study (N = 10), a mobile mood sampling application was associated with increased energy and significantly decreased anger, sadness and anxiety (Morris et al., 2010). This application presented mood-reporting scales to users periodically throughout the day. After entering and recognizing their moods, users were directed to series of CBT strategies adapted for use on a phone application. For example, one breathing exercise involved a blue circle that slowly expanded and contracted to simulate rate of breathing for the user. Through these activities, users became aware of their moods and subsequently learned coping strategies for dealing with emotions (Morris et al., 2010).
Other applications may help bipolar patients make lifestyle changes, such as marginal gains in diet, sleep and exercise (Sylvia et al., 2010). For example, diet can be monitored using phone applications and is thus, an excellent candidate for making small changes. Team Sky monitored their diet intake as well as its nutritional value as part of their marginal gains strategy. My Meal Mate (MMM) is an application that allows users to record foods and drinks consumed (and corresponding nutritional components) as well as the duration of exercise to track one’s calorie consumption. MMM shows users graphical data of calorie intake over time and sends weekly individualized text messages charting progress. In a 6-month-long trial of 128 individuals using MMM, the average weight loss was 5.0 kg (11.02 lb; Carter et al., 2013). If an individual with bipolar disorder could reduce their daily caloric intake by 1% each day, or approximately 20 calories, this would lead to 140 calories not consumed each week which is nearly the amount needed to lose 1 lb. Similarly, by tracking daily alcohol consumption, patients could determine a very small, or approximately 1%, reduction in alcohol (perhaps a beer with less alcohol content or half a shot less of wine). Tracking daily exercise with phone applications (similar to MMM) can also supply important data to make marginal gains. Strava, a cycling and running application, allows users to track workout distance and speed. If these data could be used to cycle 1% faster, speeding up from 15 to 15.15 miles per hour, this almost unnoticeable change could be a small step toward improving overall wellness.
Sleep–wake cycle stabilization is another area in which marginal gains could have far reaching effects for individuals with bipolar disorder. Disrupted sleep has been shown to trigger mania (Wehr et al., 1987) and lead to worse course of illness and difficulty in functioning (Walz et al., 2013). Sleep was also a key aspect that the Sir Brailsford targeted with Team Sky (i.e. they changed their sleeping position as well as the pillows, sheets and mattresses to maximize comfort). Sleepbot is an application that tracks sleeping patterns and allows users to see information about time spent asleep and movement throughout the night. This application presents graphs designed to help users improve sleeping habits. Similarly, activity scheduling, or improving one’s daily social rhythms, can help patients with bipolar disorder to improve their mood. Ehlers et al. (1988) proposed the social Zeitgeber theory, which posits that stressful life events can lead to depressive episodes by disrupting social and biological rhythms. There is also evidence that disruptions in social rhythms are associated with the onset of manic episodes (Malkoff-Scwartz et al., 1998). Interpersonal and social rhythm therapy (IPSRT) was developed as treatment designed to regulate circadian rhythms and sleep–wake cycles (Frank et al., 2000). Phone applications that focus on tracking and regulating sleep–wake cycles are now widely available on smartphones. These applications follow the model of IPSRT, tracking sleeping patterns and increase regularity in circadian rhythm and sleep–wake cycles and subsequently decrease episodes of mania and depression.
While medications are the foundation of treatment for bipolar disorder, they have a high burden of side effects (Buoli et al., 2014) and their effectiveness is compromised by low adherence rates (Sajatovic et al., 2015). Recent phone applications have been developed to help patients become more aware of their non-adherence as well as to more effectively communicate these data to their treating provider to improve medication adherence. For example, MedAgenda is a phone application for the iPhone that tracks taken and missed medication doses, provides detailed medication instructions and generates automated reminders (Dayer et al., 2013). Applications like these could help individuals with bipolar disorder track progress toward making, and persisting with, 1% behavioral changes.
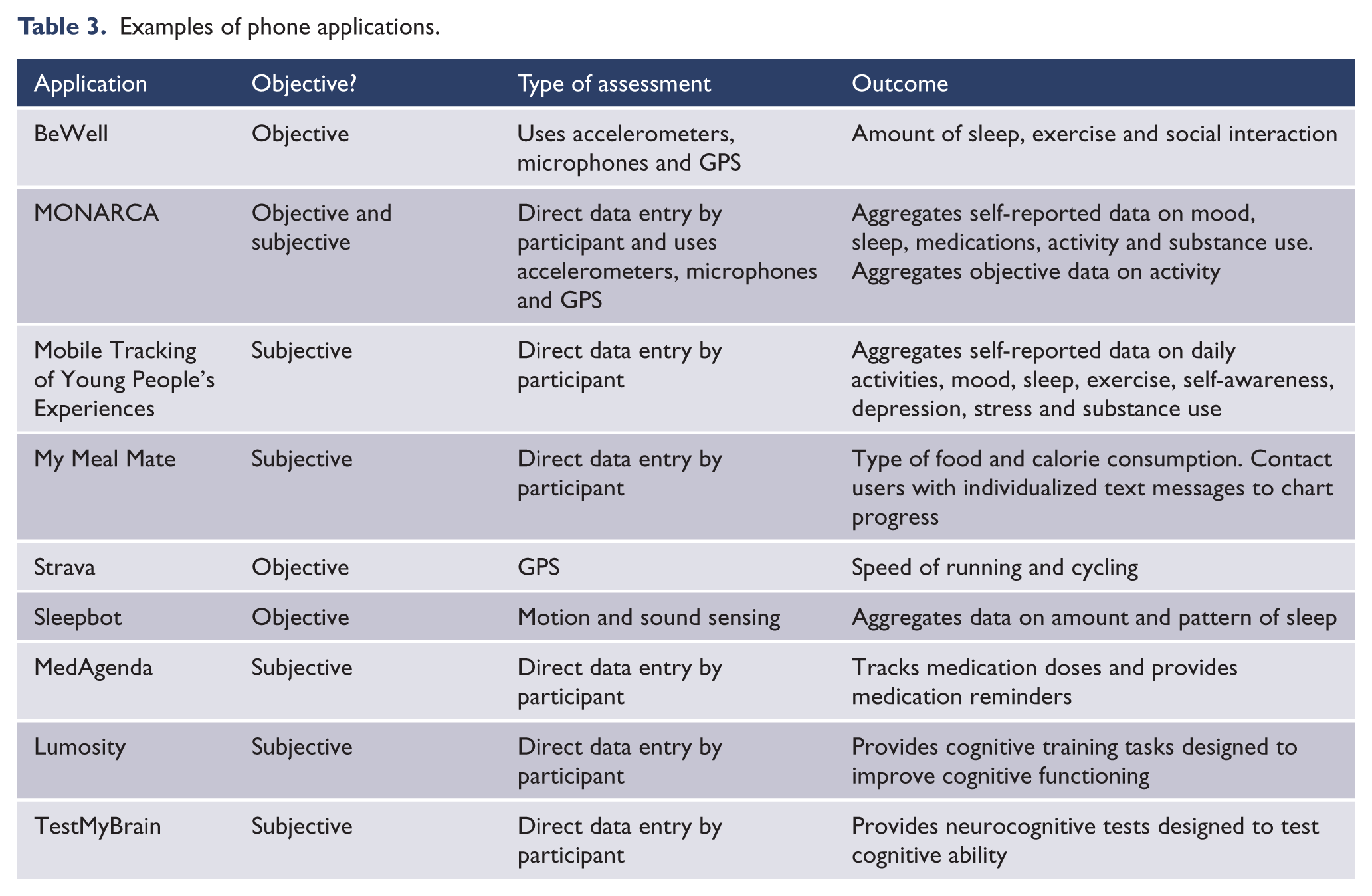
Phone applications and websites are available to track another vital area of wellness for bipolar patients, cognitive impairment. For example, TestMyBrain is a website that offers a variety of free cognitive tests. Using TestMyBrain, individuals can test their cognitive abilities using a variety of computerized brain tests. Results from these tests are stored in an online database that allows users to create a brain profile and contribute to research findings. A commercial website and phone application, Lumosity, allows users to complete a variety of cognitive tasks focused on memory, attention, speed, flexibility and problem solving. These tasks are designed to train and improve these areas of cognitive function. Using websites and applications that target cognitive functioning, such as TestMyBrain and Lumosity, patients can increase wellness (Table 3).
Examples of phone applications.
Making marginal changes with peer support
Peer support can help ease feelings of social isolation while increasing understanding of one’s situation (Davidson et al., 1999). By joining a group in which people share experiences with one another, patients can both give and receive advice about difficulties associated with their illness. Through offering advice to others, patients can feel that they are fulfilling societal roles and are given purpose. On the other hand, hearing advice can give individuals the tools to cope with difficult situations. Peer support need not come from joining groups specific to mental illnesses, but could be accomplished by joining any social endeavor in which skills and information are learned in a supportive social community (Davidson et al., 1999). Thus, the support could be instrumental in moving bipolar individuals toward marginal gains.
Peer support improves empowerment. Empowerment, achieved through sharing and hearing stories, can help people cope with changes in their lives by providing a context or feeling of collectivity to their story (Rappaport, 1995). Feelings of collectivity can help individuals manage stress-inducing changes in their own lives by making the change feel smaller when placed in a larger context (Rappaport, 1995). The Depression Bipolar Support Alliance (DBSA) and Recovery Inc. found that members had lower hospitalization rates after joining peer support groups (Galanter, 1988; Kurtz, 1988). Remarkably, the hospitalization rate of Depression and Bipolar Support Alliance (DBSA) members dropped from 82% to 33%, while that of Recovery Inc. members dropped from 52% to 7% (Kurtz, 1988). Sharing connections with others can help increase ability to cope and subsequently decrease severity of illness (Galanter, 1988). A 1% change in interaction frequency and type an individual shares could be a manageable and influential change for bipolar patients.
Discussion
Team Sky has achieved remarkable success using the concept of marginal gains and provides important lessons for how we can help our bipolar patients. In this paper, we reviewed the overall philosophy of marginal gains as well as specific techniques to help patients use this strategy to potentially improve their long-term outcomes. Future studies can assess the actual effectiveness of these strategies.
Footnotes
Declaration of interest
A.A.N. is a consultant for Brain Cells, Inc., Bristol Myers Squibb, Corcept, Eli Lilly and Company, Forest, Genentech, GlaxoSmithKline, Healthcare Global Village, Hoffman LaRoche, Infomedic, Lundbeck, Medavante, Merck, Methylation Sciences, Naurex, PamLabs, Parexel, Pfizer, Ridge Diagnostics, Shire, Sunovion, Takeda Pharmaceuticals, Targacept and Teva and has consulted through the MGH Clinical Trials Network and Institute (CTNI) for Astra Zeneca, Brain Cells, Inc., Dianippon Sumitomo/Sepracor, Johnson and Johnson and Otsuka. He has received grants and research support from the American Foundation for Suicide Prevention, Brain and Behavior Research Foundation, Forest, Marriott Foundation, PCORI, PamLabs, Takeda/Lendbeck, and Pfizer. He has received honoraria from Belvoir Publishing, Slack Publications, APSARD, ASCP, NCDEU, Rush Medical College, Yale University School of Medicine, NNDC, Nova Southeastern University, NAMI, Institute of Medicine, CME Institute and ISCTM. He has stock with Appliance Computing, Inc. (MindSite), Brain Cells, Inc., and Medavante. He has copyrights for Clinical Positive Affect Scale and the MGH Structured Clinical Interview for the Montgomery Asberg Depression Scale exclusively licensed to the MGH Clinical Trials Network and Institute (CTNI). L.G.S. was a shareholder in Concordant Rater Systems and has served as a consultant for United Biosource Corporation, Clintara, Bracket and Clinical Trials Network and Institute. She has received grant/research support from NIMH, PCORI, Takeda and AFSP. She receives royalties from New Harbinger. I.S.M. received funding from Brazil Scientific Mobility Program Coordination for the Improvement of Higher Education Personnel. C.M.H. and L.T.Y. have no competing interests to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.