
Abstract
Objective:
Even with treatment, approximately one-third of patients with bipolar disorder relapse into depression or mania within 1 year. Unfavorable clinical outcomes for patients with bipolar disorder include increased rates of psychiatric hospitalization and functional impairment. However, only a few studies have examined predictors of psychiatric hospital readmission in a sample of patients with bipolar disorder. The purpose of this study was to examine predictors of psychiatric readmission within 30 days, 90 days and 1 year of discharge among patients with bipolar disorder using a conceptual model adapted from Andersen’s Behavioral Model of Health Service Use.
Methods:
In this retrospective study, univariate and multivariate logistic regression analyses were conducted in a sample of 2443 adult patients with bipolar disorder who were consecutively admitted to a public psychiatric hospital in the United States from 1 January to 31 December 2013.
Results:
In the multivariate models, several enabling and need factors were significantly associated with an increased risk of readmission across all time periods examined, including being uninsured, having ⩾3 psychiatric hospitalizations and having a lower Global Assessment of Functioning score. Additional factors associated with psychiatric readmission within 30 and 90 days of discharge included patient homelessness. Patient race/ethnicity, bipolar disorder type or a current manic episode did not significantly predict readmission across all time periods examined; however, patients who were male were more likely to readmit within 1 year. The 30-day and 1-year multivariate models showed the best model fit.
Conclusion:
Our study found enabling and need factors to be the strongest predictors of psychiatric readmission, suggesting that the prevention of psychiatric readmission for patients with bipolar disorder at safety-net hospitals may be best achieved by developing and implementing innovative transitional care initiatives that address the issues of multiple psychiatric hospitalizations, housing instability, insurance coverage and functional impairment.
Introduction
Bipolar disorder (BD) types I and II affect approximately 2% of the world’s population (Merikangas et al., 2007). Compared to the general population, mortality among patients with BD is two to three times greater, while life expectancy is decreased by approximately 9 years (Gitlin et al., 1995; Saha et al., 2007). Even with treatment, approximately one-third of patients relapse into depression or mania within 1 year (Crump et al., 2013). Patients with BD often present with different courses of illness progression (Berk et al., 2011; Post and Kalivas, 2013), and a thorough understanding of the course of BD illness is important for therapeutic intervention and management of illness (Carlborg et al., 2015; Whiteford et al., 2013). An increased number of BD episodes has been associated with unfavorable clinical outcomes, including increased rates of hospitalization, reduced inter-episode intervals and functional impairment (Kessing et al., 2004; Magalhães et al., 2012). For example, in a naturalistic study of 1106 patients with BD, the rate of relapse leading to hospitalization was found to increase with the number of previous psychiatric hospitalizations (Kessing et al., 2004).
Nevertheless, the predictors associated with relapse and rehospitalization for patients with BD during different time periods after discharge remain largely unexplored. While psychiatric readmissions in general have been well studied, prior research has primarily been conducted in mixed-diagnosis samples (Byrne et al., 2010; Craig and Bracken, 1995; Monnely, 1997; Schmutte et al., 2010; Swett, 1995). Across diagnoses, factors such as low patient functioning and stability (Mojtabai et al., 1997; Monnely, 1997) and housing instability and homelessness (Appleby and Desai, 1987; Voineskos and Denault, 1978) have been found to increase the risk for psychiatric readmission.
Among studies that included patients with schizophrenia and/or affective disorders (Appleby et al., 1993; Monnely, 1997; Swett, 1995) as well as studies that only included patients with BD (Kessing et al., 2004; Kreys et al., 2013; Patel et al., 2005), a greater number of prior psychiatric hospitalizations was found to increase the risk of readmission.
A few studies have examined risk factors for readmission in samples that included only patients with BD (Kessing et al., 2004; Kreys et al., 2013; Patel et al., 2005; Perlick et al., 1999; Woo et al., 2014). In addition to the impact of the number of BD episodes on psychiatric readmission as reported above (Kessing et al., 2004), one prospective study examined the effect of clinical symptoms as risk factors for psychiatric readmission among 100 patients with BD (Perlick et al., 1999), and three studies examined the effect of medication differences on psychiatric readmission among patients with BD (Kreys et al., 2013; Patel et al., 2005; Woo et al., 2014). Two studies examining the effects of medication differences on psychiatric readmission for patients with BD found no relationship between medication differences and psychiatric readmission; however, both studies found a greater number of prior psychiatric hospitalizations increased readmission risk (Kreys et al., 2013; Patel et al., 2005). In contrast, the third study found treatment with valproate and an atypical antipsychotic to be more effective than treatment with lithium and an atypical antipsychotic in preventing psychiatric readmission during the first year after psychiatric hospitalization for a first manic episode in patients with BD type I (Woo et al., 2014).
Because BD has been associated with high inpatient hospital utilization and health care costs (Peele et al., 2003), additional research is needed that identifies risk factors and critical time periods for readmission for patients with BD. Such information could allow for the better identification of at-risk patients and the more efficient allocation of limited health care resources. The purpose of the present study was to examine factors associated with psychiatric readmission within 30 days, 90 days and 1 year of discharge among patients with BD treated at an academic psychiatric hospital serving as a regional safety-net provider. Readmissions occurring closer to the time of hospital discharge have been associated with the quality of care delivered during psychiatric hospitalization; however, the influence of an index hospitalization on readmission has been shown to diminish over time as additional factors including the cyclical course of illness and access to community-based services increase readmission risk (Craig et al., 2000; Durbin et al., 2007; Heggestad, 2001). Hence, our study sought to identify respective predictors for both the short-term and long-term risks of readmission for patients with BD utilizing a conceptual model of health services use. Our conceptual model was adapted from Andersen’s Behavioral Model of Health Service Use that groups factors associated with health service utilization into three categories: predisposing (characteristics of the individual, that is, age, gender, race, marital status), enabling (system or structural factors that make health service resources available to the individual) and need (severity of illness) factors (Andersen, 1995; Andersen and Newman, 1973).
The research questions were as follows: (1) What predisposing, enabling and need factors increase the risk for psychiatric readmission among patients with BD within 30 days, 90 days or 1 year of discharge? (2) What relationship does a history of inpatient psychiatric hospitalization (⩾3 prior) have with psychiatric readmission when controlling for predisposing, enabling and need factors? and (3) What relationship does a lower Global Assessment of Functioning (GAF) score (indicating functional impairment) have with psychiatric readmission when controlling for predisposing, enabling and need factors? Given our theoretical framework, we hypothesized that (1) predisposing, enabling and need factors would differentially predict psychiatric readmissions for patients with BD across the time periods examined; (2) patients with BD with ⩾3 prior psychiatric hospitalizations would be at increased risk for readmission within 30 days, 90 days and 1 year of discharge and (3) patients with BD with lower GAF scores would be at increased risk for readmission within 30 days, 90 days and 1 year of discharge.
Methods
The study was a retrospective review of electronic medical record data for adult patients with BD in an academic safety-net psychiatric hospital. The study included 2443 patients at least 18 years old consecutively admitted from 1 January to 31 December 2013. All information related to predisposing, enabling and need factors included in the analyses was obtained from the hospital electronic medical record system. Patient Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) Axis I diagnoses (Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition, Text Revision [DSM-IV-TR] codes: 296.0–296.89) and GAF score ratings were made by the attending psychiatrist responsible for the care of the patient using DSM-IV diagnostic criteria. The attending psychiatrist attempted to confirm patient diagnoses by obtaining collateral information from the patient and clinical staff and by accessing patient information from previous hospital admissions and outpatient medical records.
Using univariate and multivariate regression analysis, we examined potential predisposing, enabling and need factors during an index admission for patients with BD in order to determine whether any of these factors would differentiate between patients who were readmitted within 30 days, 90 days and 1 year and those who were not. Three multivariate models were constructed using block-wise entry to examine each readmission time period separately. The predictors were grouped into blocks based on the categories in the Andersen model theoretical framework and a stepwise selection was applied. Each block was applied separately while the other predictor variables were ignored, and variables were removed when they did not contribute to the prediction. Variables entered into the analysis included predisposing factors (age, gender, race/ethnicity, marital status), enabling factors (living situation, insurance status, 3 or more prior psychiatric hospitalizations, involuntary admission status) and need factors (current episode of mania, BD type, GAF score) (see conceptual model in Figure 1).
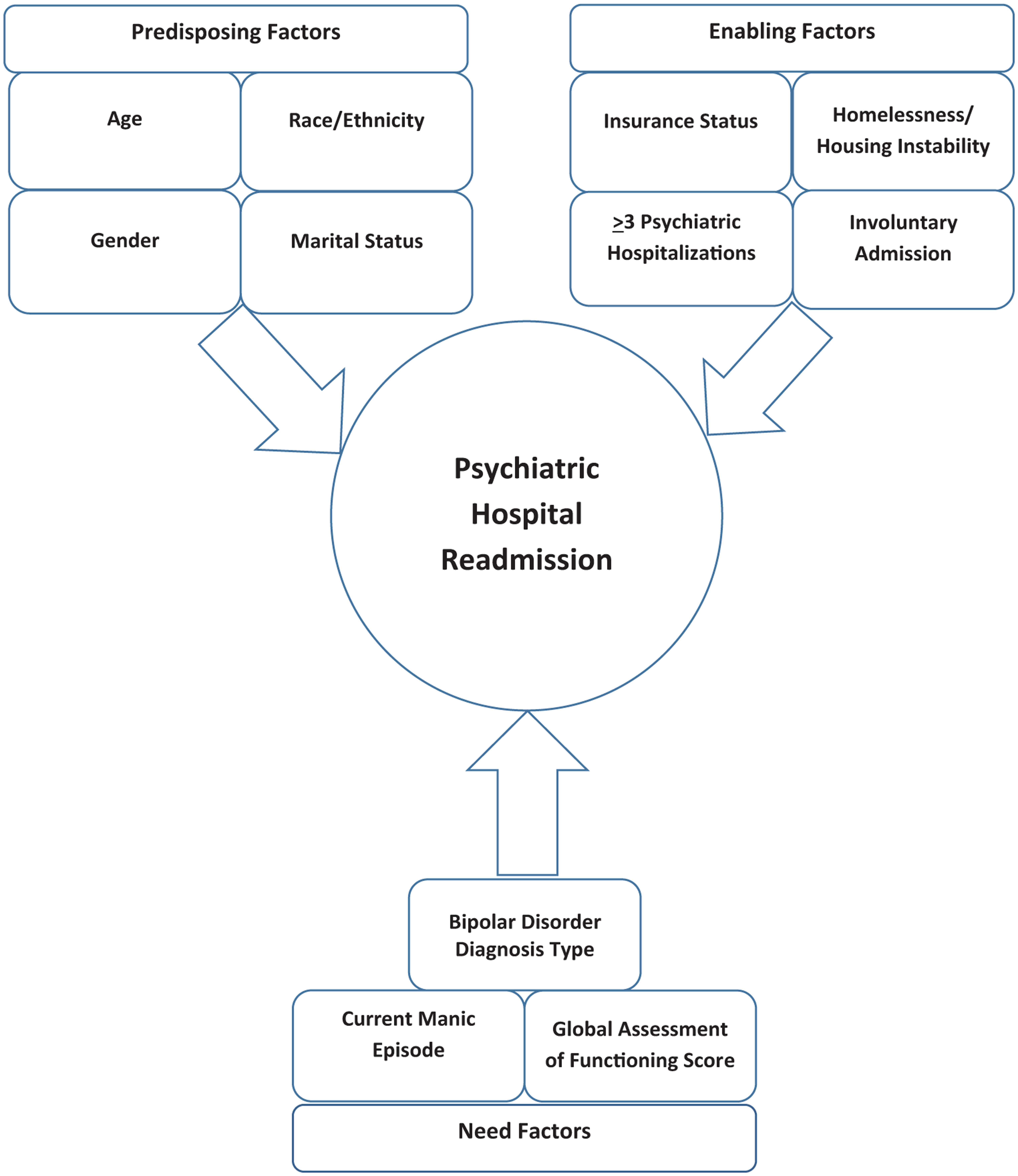
Conceptual model.
Admission age and GAF scores were included as continuous variables. Race/ethnicity was coded into four categories: non-Hispanic white, African American, Hispanic and other race/ethnicity. Marital status was dummy coded into two categories: married or unmarried. Living situation was coded into four categories: living in a home/private residence, homeless and living in a shelter, homeless and living on the streets and placement in an institution/jail. Health insurance status was coded into four categories: commercially insured, Medicare, Medicaid and uninsured. The number of prior psychiatric hospitalizations was dummy coded into two categories: having two or less or three or greater prior psychiatric hospitalizations. Involuntary status was dummy coded into two categories: involuntarily admitted or voluntarily admitted. Manic episode was coded into two categories based on the DSM diagnosis: manic episode or no manic episode. BD type was coded into two categories: BD I or BD II. All analyses were conducted in SPSS for Windows version 2.1. This study was approved by the Institutional Review Board at UT Health Science Center at Houston.
Results
Sample characteristics
A total of 2443 patients with BD met study inclusion criteria. Patient characteristics are presented in Table 1. Among the patients included in our study, 11% (n = 269) were previously admitted to our hospital within 30 days of a current hospitalization. Another 18.9% of the patients (n = 461) were admitted to our hospital during the previous 90 days, and 31.4% (n = 766) were previously admitted to our hospital during the previous year. While many hospitalizations represented a readmission, more patients (1162, 47.6%) were first-time patients at our hospital.
Sample characteristics.
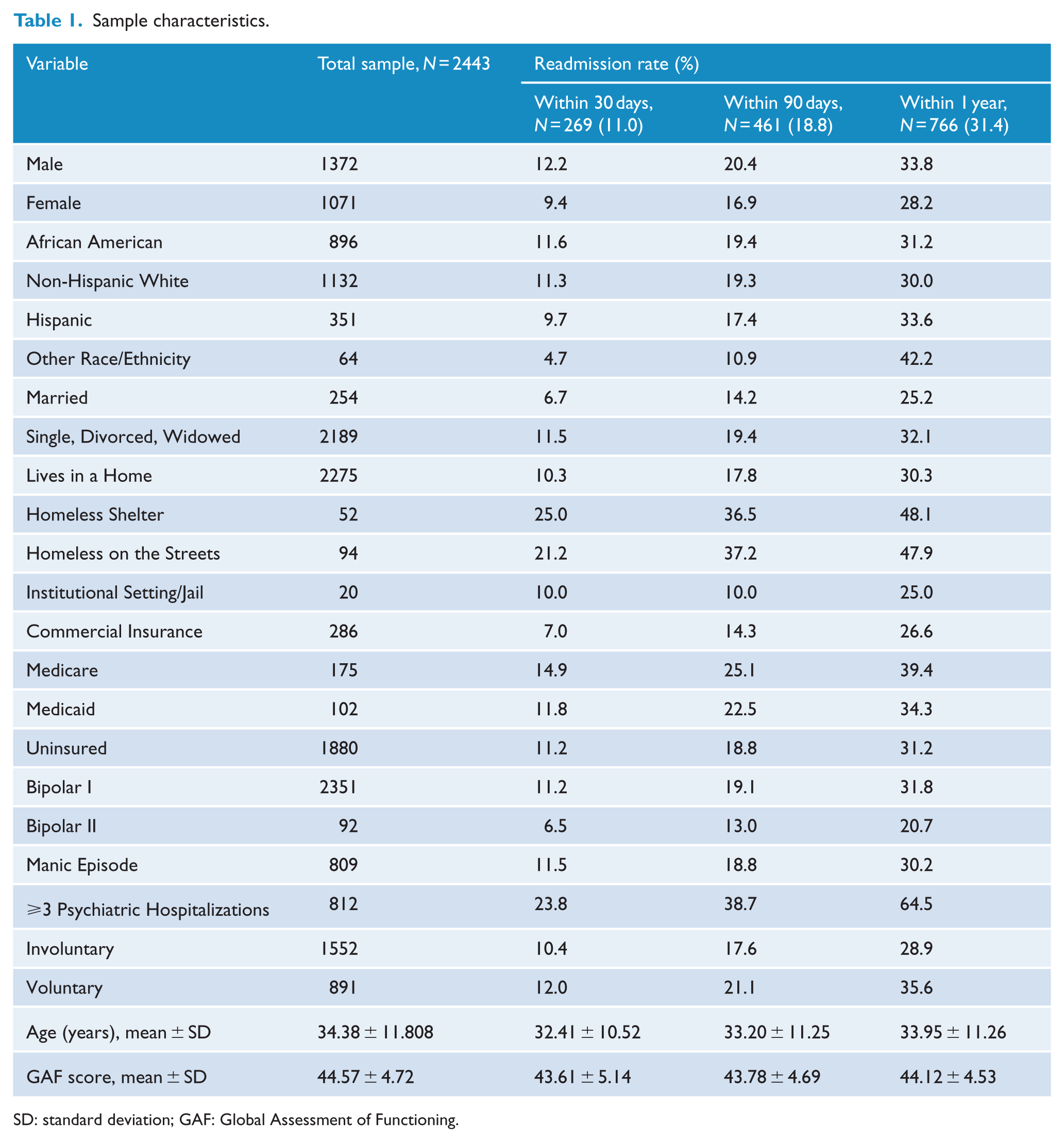
SD: standard deviation; GAF: Global Assessment of Functioning.
Univariate analyses
Readmissions within 30 days of discharge
In the univariate analyses, older age was associated with a decreased risk of readmission within 30 days of discharge (odds ratio [OR]: 0.983; 95% confidence interval [CI] = [0.983, 0.972]; p = 0.004). Additionally, patients who were male (OR: 1.340; 95% CI = [1.032, 1.740]; p = 0.028) or who had ⩾3 psychiatric hospitalizations (OR: 6.379; 95% CI = [4.815, 8.452]; p < 0.001) were also more likely to be readmitted within 30 days of discharge. In contrast, patients who were married (OR: 0.551; 95% CI = [0.331, 0.918]; p = 0.022) or had a higher GAF score (OR: 0.950; 95% CI = [0.923, 0.977]; p < 0.001) were less likely to be readmitted within 30 days of discharge. Compared to patients who were living in a home, patients who were homeless and living on the streets (OR: 2.357; 95% CI = [1.413, 3.934]; p = 0.001) or were living in a homeless shelter (OR: 2.907; 95% CI = [1.530, 5.525]; p = 0.001) were more likely to be readmitted within 30 days of discharge. Compared to patients with commercial insurance, patients who were uninsured (OR: 1.681; 95% CI = [1.044, 2.708]; p = 0.033) or who had Medicare (OR: 2.321; 95% CI = [1.253, 4.299]; p = 0.007) were more likely to be readmitted within 30 days of discharge.
Readmissions within 90 days of discharge
In the univariate analyses, older age was associated with a decreased risk of readmission within 90 days of discharge (OR: 0.989; 95% CI = [0.981, 0.998]; p = 0.017). Patients who were male (OR: 1.261; 95% CI = [1.025, 1.550]; p = 0.028) or who had ⩾3 psychiatric hospitalizations (OR: 6.365; 95% CI = [5.105, 7.936]; p < 0.001) were more likely to be readmitted within 90 days of discharge. Patients who were married (OR: 0.685; 95% CI = [0.474, 0.990]; p = 0.044), had a higher GAF score (OR: 0.955; 95% CI = [0.933, 0.977]; p < 0.001) or were involuntarily admitted (OR: 0.798; 95% CI = [0.649, 0.982]; p = 0.033) were less likely to be readmitted within 90 days of discharge. Compared to patients who were living in a home, patients who were homeless and living on the streets (OR: 2.747; 95% CI = [1.784, 4.231]; p < 0.001) or were living in a homeless shelter (OR: 2.666; 95% CI = [1.501, 4.737]; p = 0.001) were more likely to be readmitted within 90 days of discharge. Compared to patients with commercial insurance, patients who had Medicare (OR: 2.007; 95% CI = [1.248, 3.229]; p = 0.004) were more likely to be readmitted within 90 days of discharge.
Readmissions within 1 year of discharge
In the univariate analyses, patients who were male (OR: 1.301; 95% CI = [1.094, 1.548]; p = 0.003) or who had ⩾3 psychiatric hospitalizations (OR: 10.443; 95% CI = [8.565, 12.733]; p < 0.001) were more likely to be readmitted within 1 year of discharge. Compared to patients who were living in a home, patients who were homeless and living on the streets (OR: 2.114; 95% CI = [1.397, 3.200]; p < 0.001) or living in a homeless shelter (OR: 2.131; 95% CI = [1.228, 3.699]; p = 0.007) were more likely to be readmitted within 1 year of discharge. Compared to patients with commercial insurance, patients who had Medicare (OR: 1.799; 95% CI = [1.205, 2.686]; p = 0.004) were more likely to be readmitted within 1 year of discharge. In contrast, patients who were married (OR: 0.714; 95% CI = [0.530, 0.960]; p = 0.026), had BD II (OR: 0.559; 95% CI = [0.335, 0.933]; p < 0.026) or who had a higher GAF score (OR: 0.970; 95% CI = [0.952, 0.989]; p = 0.002) were less likely to be readmitted within 1 year of discharge.
Multivariate analyses
Readmissions within 30 days of discharge
In the first multivariate model examining psychiatric readmission within 30 days of discharge, older age was associated with a decreased risk of being readmitted within 30 days of discharge (OR: 0.972; 95% CI = [0.959, 0.985]; p < 0.001). Compared to patients who were living in a home, patients who were homeless and living on the streets (OR: 1.775; 95% CI = [1.021, 3.088]; p = 0.042) or living in a homeless shelter (OR: 2.659; 95% CI = [1.325, 5.337]; p = 0.006) were more likely to be readmitted within 30 days of discharge.
Compared to patients who had commercial insurance, patients who were uninsured (OR: 2.288; CI=[1.381, 3.792]; p = 0.001) or who had Medicare (OR: 2.330; 95% CI = [1.203, 4.512]; p = 0.012) were more likely to be readmitted within 30 days of discharge. Patients who had ⩾3 psychiatric hospitalizations were 6.7 times more likely to be hospitalized within 30 days of discharge (OR: 6.699; 95% CI = [5.013, 8.954]; p < 0.001).
In contrast, patients who had a higher GAF score were less likely to be readmitted within 30 days of discharge (OR: 0.952; 95% CI = [0.923, 0.983]; p = 0.002). Overall, the multivariate model showed a good fit to the data, with a Hosmer–Lemeshow goodness of fit statistic of 14.352 with 8 degrees of freedom (p = 0.073). In the final block containing all predictor variables, the Cox/Snell and Nagelkerke pseudo R-squareds ranged from 0.093 to 0.186. The results of the full model are presented in Table 2.
Readmission within 30 days, 90 days and 1 year of discharge.
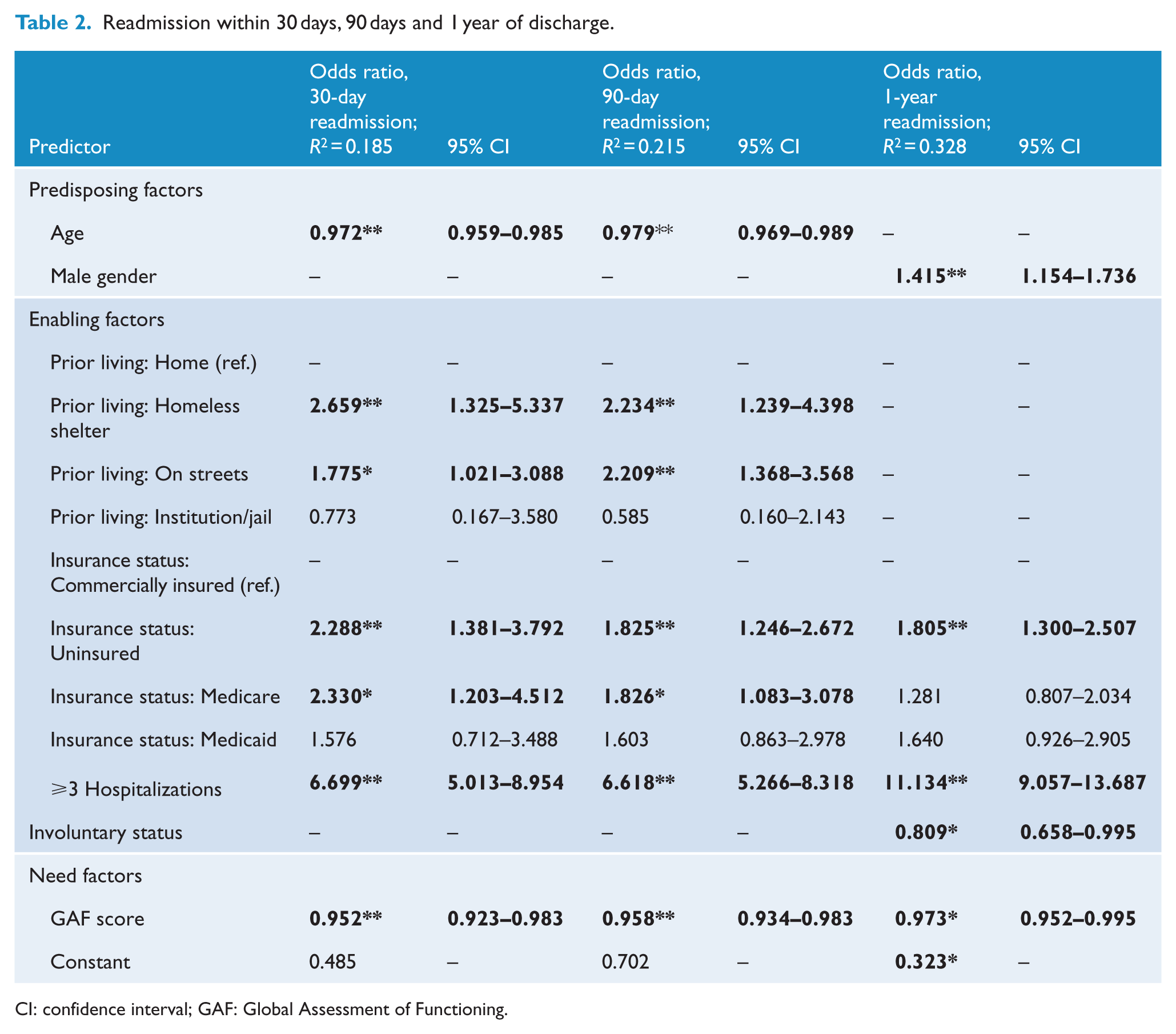
CI: confidence interval; GAF: Global Assessment of Functioning.
Readmissions within 90 days of discharge
In the second multivariate model examining psychiatric readmission within 90 days of discharge, older age was associated with a decreased risk of readmission within 90 days of discharge (OR: 0.979; 95% CI = [0.969, 0.989]; p < 0.001). Compared to patients who were living in a home, patients who were living in a homeless shelter (OR: 2.234; 95% CI = [1.239, 4.398]; p = 0.009) or who were homeless and living on the streets (OR: 2.209; 95% CI = [1.368, 3.568]; p = 0.001) were more likely to be readmitted within 90 days of discharge. Compared to patients who had commercial insurance, patients who were uninsured (OR: 1.825; 95% CI = [1.246, 2.672]; p = 0.002) or who had Medicaid (OR: 1.826; 95% CI = [1.083, 3.078]; p = 0.024) were more likely to be readmitted within 90 days of discharge.
Patients who had ⩾3 psychiatric hospitalizations (OR: 6.618; 95% CI = [5.266, 8.318]; p < 0.001) were more likely to be readmitted within 90 days of discharge. In contrast, patients who had a higher GAF score were less likely to be readmitted within 90 days of discharge (OR: 0.958; 95% CI = [0.934, 0.983]; p = 0.001). The second multivariate model showed a poor fit for the data, with a Hosmer–Lemeshow goodness of fit statistic of 18.087 with 8 degrees of freedom (p = 0.021). In the final block containing all predictor variables, the Cox/Snell and Nagelkerke pseudo R-squareds ranged from 0.133 to 0.215. The results of the full model are presented in Table 2.
Readmissions within 1 year of discharge
In the third multivariate model examining psychiatric readmission within 1 year of discharge, male patients were 1.4 times more likely to be readmitted within 1 year of discharge compared to females (OR: 1.415; 95% CI = [1.154, 1.736]; p = 0.001). Compared to patients who had commercial insurance, patients who were uninsured were 1.8 times more likely to be readmitted within 1 year of discharge (OR: 1.805; 95% CI = [1.300, 2.507]; p < 0.001). Additionally, patients who had ⩾3 psychiatric hospitalizations were 11.1 times more likely to be readmitted within 1 year of discharge (OR: 11.134; 95% CI = [9.057, 13.687]; p < 0.001). In contrast, patients who were involuntarily admitted (OR: 0.809; 95% CI = [0.658, 0.995]; p = 0.045) or had a higher GAF score (OR: 0.973; 95% CI = [0.952, 0.995]; p = 0.017) were less likely to be readmitted within 1 year of discharge. The multivariate model showed a good fit to the data, with a Hosmer–Lemeshow goodness of fit statistic of 1.530 with 8 degrees of freedom (p = 0.992). In the final block containing all predictor variables, the Cox/Snell and Nagelkerke pseudo R-squareds ranged from 0.233 to 0.328. The results of the full model are presented in Table 2.
Discussion
Several enabling and need factors increased the risk for psychiatric readmission across all time periods examined, including being uninsured, having three or more prior psychiatric hospitalizations and having a lower GAF score. The finding that patients with BD who lacked health insurance, an indicator of living in poverty and being unemployed, were more likely to be readmitted is consistent with previous research that found a relationship between poverty, unemployment and psychiatric readmission (Lin et al., 2010; Schmutte et al., 2010). This finding may indicate that uninsured patients in our study experienced difficulties accessing post-discharge outpatient services, resulting in the patients’ readmission. Prior research has shown the lack of health insurance to be a significant factor affecting whether persons receive appropriate mental health care in the United States (Mechanic, 2002). To examine the possibility that patients with Medicaid, Medicare or commercial insurance were more likely to readmit to another psychiatric hospital in our region compared to discharged patients who lacked health insurance, we examined psychiatric hospital readmissions for our discharged patients in a 2012 statewide database. The readmission rate for adult patients with BD who discharged from our hospital in 2012 and readmitted to another psychiatric hospital in our region was 5.6%. Additionally, the majority of our patients (56.2%) who were readmitted to another psychiatric hospital in our region were also uninsured (Texas Department of State Health Services [TX DSHS], 2015). Thus, it is possible that patients discharging from our hospital who lacked health insurance were unable to access outpatient services, resulting in a readmission to our hospital or to another psychiatric hospital in our region. This finding may suggest that new strategies are needed at our hospital to improve the patients’ transition from inpatient to outpatient services especially for patients who are uninsured.
As we hypothesized, having three or more prior psychiatric hospitalizations increased the risk of readmission across all time periods examined. This finding is consistent with three prior studies of patients with BD that found an increased risk for readmission among patients with prior psychiatric hospitalizations (Kreys et al., 2013; Patel et al., 2005; Perlick et al., 1999).
As we hypothesized, a lower patient GAF score was associated with a higher likelihood of being readmitted across all time periods examined, which is consistent with prior research linking lower GAF scores to psychiatric readmission (Monnely, 1997). In the present study, patients with BD with higher GAF scores may have had greater insight regarding their mental illness and may have been more compliant with psychiatric treatment. In contrast, patients with BD with lower GAF scores may have had poor insight into their mental illness, causing them to be less likely to engage in post-discharge outpatient services and to be less adherent with their discharge medications. Multiple studies conducted in mixed-diagnosis samples have found an association between poor aftercare attendance and psychiatric readmission (Byers and Cohen, 1979; Hamilton et al., 2015; Nelson et al., 2000). Prior research has also shown medication non-adherence to increase readmission risk among patients with schizophrenia and schizoaffective disorders (Bodén et al., 2011). Accordingly, additional research is needed that examines the impact of aftercare attendance and medication adherence in studies limited to patients with BD.
Additional factors associated with psychiatric readmission for patients with BD within 30 and 90 days of discharge, controlling for other factors, included living in a homeless shelter or living on the streets prior to readmission. Prior research has found an association between current or recent homelessness and hospital readmission (Kushel et al., 2001). In the present study, the increased risk of living in a homeless shelter and psychiatric readmission may be partially explained by the policy of many of the homeless shelters in our region to have a maximum stay of 30 days during which a resident is not required to pay rent. It is possible the lack of stable housing faced by homeless patients after shelter discharge exacerbated the patients’ mental health conditions, resulting in the patients’ psychiatric readmission. Additional research is needed to study the outcomes of homeless psychiatric patients discharged into shelters that examines the effects of housing instability and homelessness on mental health outcomes.
In the univariate analyses, males in our sample were more likely to be readmitted across all time periods examined and within 1 year of discharge in the multivariate model. These findings are consistent with prior research that has associated male gender with readmission (Lin et al., 2006, 2010). Individuals with BD have been shown to display greater rates of anger and aggressive behaviors, especially during acute and psychotic episodes (Ballester et al., 2012). Male patients displaying anger and aggression in particular may have been perceived as threatening by patient caregivers who may have facilitated the patients’ rehospitalization. Because the multivariate analyses showed that patients with BD readmitting within 1 year were also less likely to be involuntarily admitted, more research is needed to examine the relationship between being male, having a BD diagnosis and psychiatric readmission within 1 year of discharge.
In the univariate analyses, BD II was associated with a decreased chance of readmission within 1 year of discharge; however, this relationship did not remain significant in the multivariate model when controlling for other factors. Prior research has found BD II to be associated with lower rates of inpatient hospitalization (Bega et al., 2012; Vieta et al., 1997); therefore, additional research is needed to examine the relationship between BD type and readmission risk.
In the present study, patient race/ethnicity was not found to predict readmission across the time periods examined. This finding is consistent with previous research that found no relationship between race/ethnicity and psychiatric readmission (Appleby et al., 1993; Kreys et al., 2013; Schmutte et al., 2010).
While the multivariate models examining readmissions within 30 days and 1 year of discharge showed good fit for the data, the multivariate model examining readmissions within 90 days of discharge showed poor fit for the data. The rate of psychiatric patients readmitted within 30 days of discharge is an established behavioral health system performance measure (Hermann et al., 2006) linked to the quality of inpatient psychiatric care (Craig et al., 2000), patient functioning and a greater number of prior hospitalizations (Monnely, 1997). Thus, it is possible that discharging patients were influenced by additional factors from 31 to 90 days post hospital discharge that we could not examine in medical record data.
The strengths of this study include the large and diverse sample of consecutively admitted patients with BD during a 1-year period at an academic safety-net psychiatric hospital. Additionally, the effect sizes measured by the pseudo R-squareds indicate sufficient power to detect differences across time.
Our study is novel in that it uses a conceptual model for predicting psychiatric hospital readmission risk within 30 days, 90 days and 1 year of hospital discharge. Limitations of our study include incomplete data on patient substance use, which impeded our ability to examine its effect on psychiatric readmission. Future studies should consider substance abuse after hospital discharge as a predictor of psychiatric readmission for patients with BD as one prior study has found a relationship between substance abuse and 30-day psychiatric readmission for patients with schizophrenia (Boaz et al., 2013). Additional study limitations include the use of retrospective data, which limited our ability to examine engagement in aftercare services and medication adherence after psychiatric discharge.
Controlled prospective studies are needed to track patients with BD after discharge to further elucidate factors associated with psychiatric readmission. While the total number of the patients’ prior psychiatric hospitalizations was used to examine readmission risk, we have controlled for patient age to take into account that older patients are potentially more likely to have multiple hospitalizations. The use of GAF scores to examine the effect of functional impairment on psychiatric readmission is also a limitation of this study. While one prior study has examined the relationship between GAF scores during hospitalization and readmission risk (Monnely, 1997), additional studies have found problems with both the reliability and validity of GAF (Aas, 2010). While the GAF has been recommended for routine clinical use (Salvi et al., 2005), GAF scoring reliability has been shown to be lower in clinical settings (Burlingame et al., 2005; Hilsenroth et al., 2000; Vatnaland et al., 2007). Both concurrent validity (Burlingame et al., 2005; Hilsenroth et al., 2000; Niv et al., 2007; Salvi et al., 2005) and predictive validity (Niv et al., 2007) have also been shown to be problematic with the GAF. However, while further development of the GAF to improve its validity and reliability is indicated (Aas, 2010), the use of the GAF across our hospital for scoring the severity of illness enabled us to examine the relationship between patient functioning and increased risk of psychiatric readmission in a large, hospital-wide study. Accordingly, the significant relationship we found between low patient functioning and psychiatric readmission within 30 days, 90 days and 1 year of discharge is a strength of this study.
Conclusion
Our study found enabling and need factors to be the strongest predictors of psychiatric readmission. Therefore, the prevention of psychiatric readmissions for patients with BD at safety-net hospitals may be best achieved by developing and implementing innovative transitional care initiatives that address the issues of multiple psychiatric hospitalizations, housing instability, insurance coverage and functional impairment.
Footnotes
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.