
Abstract
Objectives:
Given the sensitivity of individuals with mood disorders to circadian disruption, transmeridian travel would likely be a high-risk endeavour leading to onset or relapses in mood. A systematic review was undertaken to identify the evidence of the impact of transmeridian travel on people with mood disorders.
Methods:
Databases search included the following: CINAHL, MEDLINE, PsycINFO and manual searching using the keywords jetlag, transmeridian travel, circadian rhythm disruption, mood disorder, bipolar, major depression, seasonal affective disorder, depression, mania and hypomania.
Results:
Only three studies were identified that related to transmeridian travel and jetlag in people with mood disorders. There is some suggestion that transmeridian travel does appear to precipitate mood episodes with an increased rate of episodes of depression with westward compared with an increased rate of manic/hypomanic episodes with eastward travel. Individuals with a previous history of mood disorder appear to be more vulnerable if adherence to medication is compromised.
Conclusion:
Given the limited evidence that transmeridian travel precipitates mood episodes, this poses difficulties in identifying suitable ways to mitigate the effects of transmeridian travel in mood disorders. However, in the absence of mood-specific guidelines, some guidance can be given based on our current understanding of the relevance of circadian disruption to both jetlag and mood disorders. Further research is required to identify more focused strategies to mitigate the impact of transmeridian travel for individuals with mood disorders.
Introduction
Jetlag can be understood in the context of the human circadian system and occurs as a consequence of circadian misalignment caused by crossing time zones too rapidly for the circadian system to keep pace (Sack, 2009). In humans, the circadian clock enables the organisation of metabolism and the cell cycle according to the time of day which results in reactions occurring at the time of the day when they are most needed (e.g. energy production during the activity phase, repair mechanisms during the rest phase). The strongest cue for the synchronisation of the circadian system is light, which is perceived by specialised retinal ganglion cells. These project directly to neurons within the suprachiasmatic nuclei (SCN), the main co-ordinator of the mammalian circadian system. The output from these neurons acts on various brain regions involved in hormone secretion, sleep regulation, thermoregulation and feeding/reward (Albrecht, 2010). The circadian system continuously adapts to and synchronises with the environment and the body’s internal signals to create a coherent functional network that regulates behaviour and physiology (Albrecht, 2012).
In jetlag, the circadian processes are out of alignment. This tends to occur when three or more time zones are crossed. Symptoms are due to the effects of an unadjusted body clock in the new time zone (Waterhouse et al., 2007). The circadian clock is slow to reset, requiring approximately a day per time zone for the circadian system to re-synchronise (Sack, 2009). Symptoms include poor sleep in the new night-time (including delayed sleep onset after eastward flights, early waking after westward flight and fractioned sleep), reduced performance in mental and physical tasks, increased fatigue, decreased concentration and gastrointestinal symptoms (Waterhouse et al., 2007). There are a number of factors that can influence the severity of symptoms. These include direction of travel with westward travel typically less impacting than eastward travel (as it requires a phase delay rather than a phase advance), the number to time zones crossed, the ability to sleep while travelling, the availability and intensity of local circadian time cues on arrival and individual differences in tolerance to circadian misalignment (Sack, 2009). Jetlag diminishes as the synchrony between the individual’s body clock and the new environment is re-established (Reilly et al., 2009).
Strategies for the treatment of jetlag are based around a realignment of the circadian clock, sleep stabilisation and management of insomnia and daytime drowsiness (Sack, 2009, 2010; Sack et al., 2007). The timing of exposure to light is the most important time cue for resynchronising the circadian system with exposure to light at evening shifting the clock to later and exposure to morning light shifting the clock earlier. Melatonin is also used to promote adjustment to the body clock and also has a sedative effect which can assist with insomnia. Sleep stabilisation involves scheduling sleep to more closely matched destination bedtime prior to travel and adopting destination bedtime on arrival. Hypnotics can also be used to assist with sleep while stimulants like caffeine can be used to reduce sleepiness.
Sleep and circadian disruption are known to be important in the pathophysiology of mood disorders (Germain and Kupfer, 2008). Social time cues such as the timing of work, meals and other activities act as social zeitgebers which are powerful entraining agents of the circadian system (Monk et al., 1990). The social rhythms hypothesis of depression (Ehlers et al., 1988) is based on the role these social zeitgebers have in the synchronising of the circadian system. The social zeitgeber theory identifies a cascading sequence set off by instability of social rhythms, leading to instability of biological rhythms such as sleep and the consequent development of somatic symptoms. Individuals become stuck in a state of pathological entrainment which results in the experience of major depression (Ehlers et al., 1988) and mania (Malkoff-Schwartz et al., 2000) in vulnerable individuals.
Given the sensitivity of individuals with mood disorders to circadian disruption, transmeridian travel would likely be a high-risk endeavour leading to onset or relapses in mood in addition to typical jetlag symptoms. The authors were prompted to explore the evidence for the impact of transmeridian travel and jetlag on people with mood disorders. This process involved undertaking a systematic review of the published evidence of the impact of transmeridian travel and jetlag on people with mood disorders and examining the implications of these findings for those with mood disorder who travel.
The review specifically sought to answer the following questions:
Is there good evidence that transmeridian travel precipitates episodes of mood disorder?
Is there a difference between east and west travel?
Is there research suggesting suitable ways of mitigating the effects of transmeridian travel in mood disorders?
Method
Search strategy
Databases search included: CINAHL, MEDLINE, PsycINFO and manual searching. The Keywords were: Jetlag, transmeridian travel, circadian rhythm disruption, mood disorder, bipolar, major depression, seasonal affective disorder, depression, mania and hypomania. The inclusion criteria were as follows:
Participants with mood disorder;
Where participants included those with other psychiatric morbidity, results for mood disorders were specified;
Aged 18 years of over;
Direction of travel reported.
Results
Only three studies were identified that related to transmeridian travel and jetlag in people with mood disorders. Only one study specifically focused on mood disorders with the other two including them in their samples. These studies are summarised in Table 1.
Summary of papers reviewed.
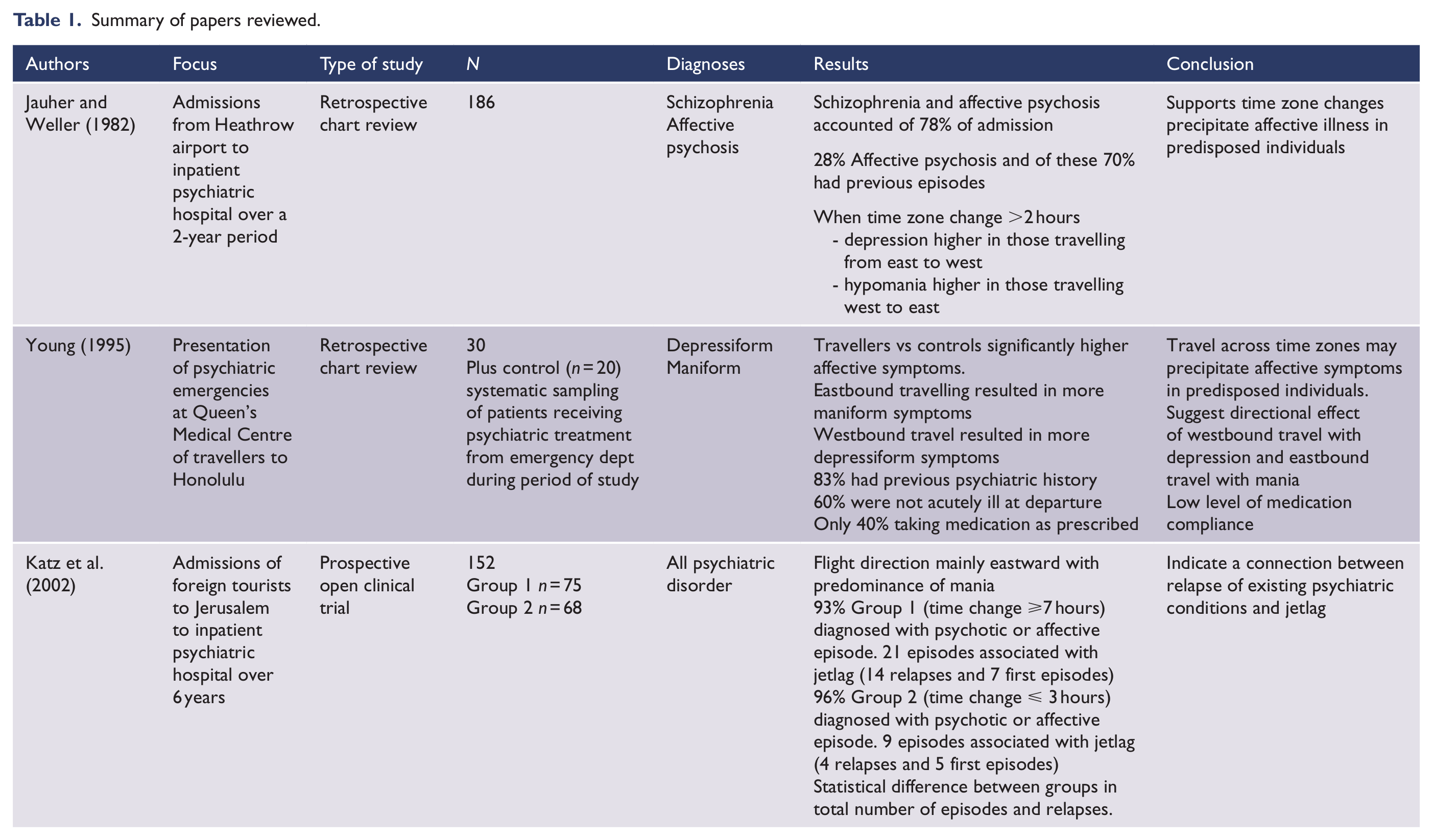
The first study was on psychiatric morbidity and time zone changes in patents from Heathrow airport (Jauhar and Weller, 1982). It included 186 individuals admitted from Heathrow airport to the nearest psychiatric hospital; however, only 89 of these had travelled (the remainder were at the airport to commence travel or for a non-travel-related reason). The primary purpose of the study was to replicate a 1976 Shapiro study (Shapiro, 1976) to determine the frequency of schizophrenia; however, they also examined mood state in relation to direction of travel and time zones crossed. The admission data over a period of 2 years (July 1976 to June 1978) were retrospectively studied. The pre- and post-travel diagnoses were determined from these records with the authors reporting use of similar criteria to those in the Syndrome Check List derived from the Present State Examination. Twenty-eight percent of individuals (n = 52 of whom 33 had travelled) were admitted with mood disorder. A high proportion of these had a history of previous episodes. Depression was significantly higher in inpatients flying east to west compared with west to east and compared with combined travel south to north and north to south. There were 24 travellers who developed hypomania of whom 15 changed time zone. The authors identified a significant difference in direction of travel between depression (east to west) and hypomania (west to east). However, this has to be viewed in the context of small numbers and multiple comparisons making a chance significant result likely.
The second study (Katz et al., 2002) reported on admissions of foreign tourists to the same mental health facility in Jerusalem (n = 152) over a 6-year period (1993–1998). Demographic and psychiatric data were collected for each patient and included diagnosis after referral (Diagnostic and Statistical Manual of Mental Disorders-IV [DSM-IV]), past psychiatric history and recent psychiatric condition 1 year prior to the journey. This study specifically focused on the association between jetlag and psychiatric morbidity and considered the impact of length of travel. To minimise the possible effect of multiple factors other than jetlag, the study was done in two stages. The study divided the group into two based on duration of travel. Group 1 (n =75) consisted of individuals who had time change of 7 hours or more and Group 2 (n=68) had time changes of 3 hours or less. The first phase of the study compared the demographic, religious background, travel history and psychiatric diagnoses of the two groups and no significant differences were found apart from religious affiliation. The criteria used for determining major mental disorder to be associated with jetlag required individuals to have had no previous psychiatric history or at least 1 year full remission prior to flight and have the appearance of psychotic or affective symptoms within 7 days after landing. The flight direction for the vast majority of individuals in both groups was eastward (89% and 86%, respectively). The predominant diagnoses were psychotic disorders (predominantly schizophrenia) and major affective disorders with no differences in rates of these conditions between the travel groups. In all, 12% (n = 10) of Group 1 and 15% (n = 11) of Group 2 were in a manic state and 2% (n = 2) of Group 1 and 5% (n = 3) of Group 2 were depressed. There was a significant difference (p = 0.02) in levels of accumulative number of first episodes and relapses presumed associated with jetlag between Group 1 (n = 21) and Group 2 (n = 9). There were also significant differences (p = 0.04) in rates of relapse probably associated with jetlag between Group 1 (n = 14) and Group 2 (n = 5). There were no differences between groups in rates of first episode illnesses. The rates were not separately analysed for mood disorders.
The sole study that focused on mood disorders was undertaken in Honolulu and investigated acute psychiatric decompensation in travellers (n = 30) seen for psychiatric emergencies at Queen’s Medical Centre emergency department (Young, 1995). All included patients had a minimum of a 2 hour time zone change and presented within 10 days of travel. Twenty non-travelling controls were selected from patients seen in the emergency department for psychiatric treatment. They were systematically (presumably randomly) sampled from the same time frame during which the travellers were recruited. Patient charts were retrospectively reviewed to determine demographic information, past psychiatric history, use of psychotropic medication, psychiatric condition at the start of travel, travel history, substance abuse and psychiatric symptoms at presentation. The travellers were classified as either depressiform (defined as having depressed mood or suicidality) or maniform (defined as having elevated or expansive mood or plus one category B DSM-III-R symptom, or two additional symptoms if mood was irritable). The authors acknowledged this classification had not been validated and had elected to use this approach to increase sensitivity to affective disturbance above DSM-III-R criteria. The study also did not account for any pre-existing differences between the groups. The majority of the travellers were westbound (63%, n = 19) with time zone changes ranging from 2 to 11 (5 ± 2.9) hours. The travellers had significantly higher presence of affective symptoms compared to controls (p = 0.01). Eastbound travellers were significantly more maniform compared to controls (p = 0.001) and westbound travellers (p = 0.05). Westbound travellers were significantly more depressiform in comparison to eastbound travellers (p = 0.05). Additionally 83% (n = 25) of travellers had a history of prior psychiatric treatment with 60% (n = 18) well at the time of departure. Prior psychiatric treatment of controls was not reported. Fifty percent (n = 15) of travellers were receiving medication for a psychiatric condition; however, only 40% (n = 6) were taking medication as prescribed. They concluded that transmeridian travel may precipitate acute mental illness in predisposed individuals. Additionally they suggested there may be a specific relationship between direction of travel and the polarity of mood disturbance with westward travel associated with depressive symptoms and eastward travel associated with mania symptoms.
Discussion
This review has highlighted the limited attention to the impact of transmeridian travel and jetlag on people with mood disorders. There is some suggestion that transmeridian travel and jetlag do appear to precipitate mood episodes. While numbers are small and studies make multiple comparisons, two separate studies do suggest an increased rate of episodes of depression with westward compared with an increased rate of manic/hypomanic episodes with eastward travel. This finding if confirmed is potentially important in recommending direction of travel (which from New Zealand to Europe, e.g., is optional). Individuals with a previous history of mood disorder appear to be more vulnerable if adherence to medication is compromised.
There are a number of limitations in comparing these studies with different samples sizes, admission facilities and diagnoses focused on. Additionally, only Katz et al. (2002) had a clear definition of the criteria for a major mental condition to be associated with jetlag. Additionally, none of the studies identified how symptoms of jetlag were distinguished from symptoms of mood episodes. It is also noteworthy that rates of psychotic disorders are much high than mood disorder and this may be a particular risk but this is outside the scope of this review.
There are many difficulties in research in this area and indeed despite the common clinical observation that time zone travel predisposes to relapse of bipolar illness in particular, this is not proven by the studies reviewed. The problems are as follows:
Long haul travel is not particularly common in the general population and because of the socio-economic disadvantages of significant mood disorder, it is probably less common in those with a mood disorder. This makes any study likely to feature small numbers and of course non-random selection.
Causality is difficult to determine. Despite the observation that patients with mania or hypomania may sometimes travel early in their illness, this is unlikely to explain an increased rate since it is a relatively uncommon phenomenon. However, attributing new episodes of mood disorder to time zone change rather than, for example, simple sleep deprivation or general stress associated with travel is difficult.
Studies have tended to identify patients based on their having had an ‘episode’ of mood disturbance. They do not identify patients with mood disorder who do not suffer such an episode. Related to this is that accessing treatment may occur at a different level of severity when patients are not at home. This may mean that patients are more likely to access care or admission because they do not have the usual supports, or less likely to because services are unfamiliar and may even use a different language.
Implications for practice
The review has identified limited guidance for mitigating the effects of transmeridian travel in mood disorders. Despite this, the findings do provide some rationale for the provision of education around the potential risks of mood disruption and the importance of maintaining medication regimes. Additionally, given circadian disruption is core to both precipitation of relapse of mood disorder (Murray and Harvey, 2010) and to symptoms of jetlag (Sack et al., 2007), the evidence-based strategies for the treatment of jetlag (Sack, 2009, 2010; Sack et al., 2007) are potentially pertinent to inform strategies for individuals with mood disorder. These strategies focus on realignment of the circadian clock, sleep management (stabilisation and scheduling) and symptomatic management of insomnia and daytime drowsiness and can be adapted to be applicable to individuals with mood disorders. Table 2 outlines recommended strategies for the management of transmeridian travel for individuals with mood disorders, although due to limited evidence these need to be considered as speculative.
Recommendations for managing transmeridian travel and jetlag for individuals with mood disorder.
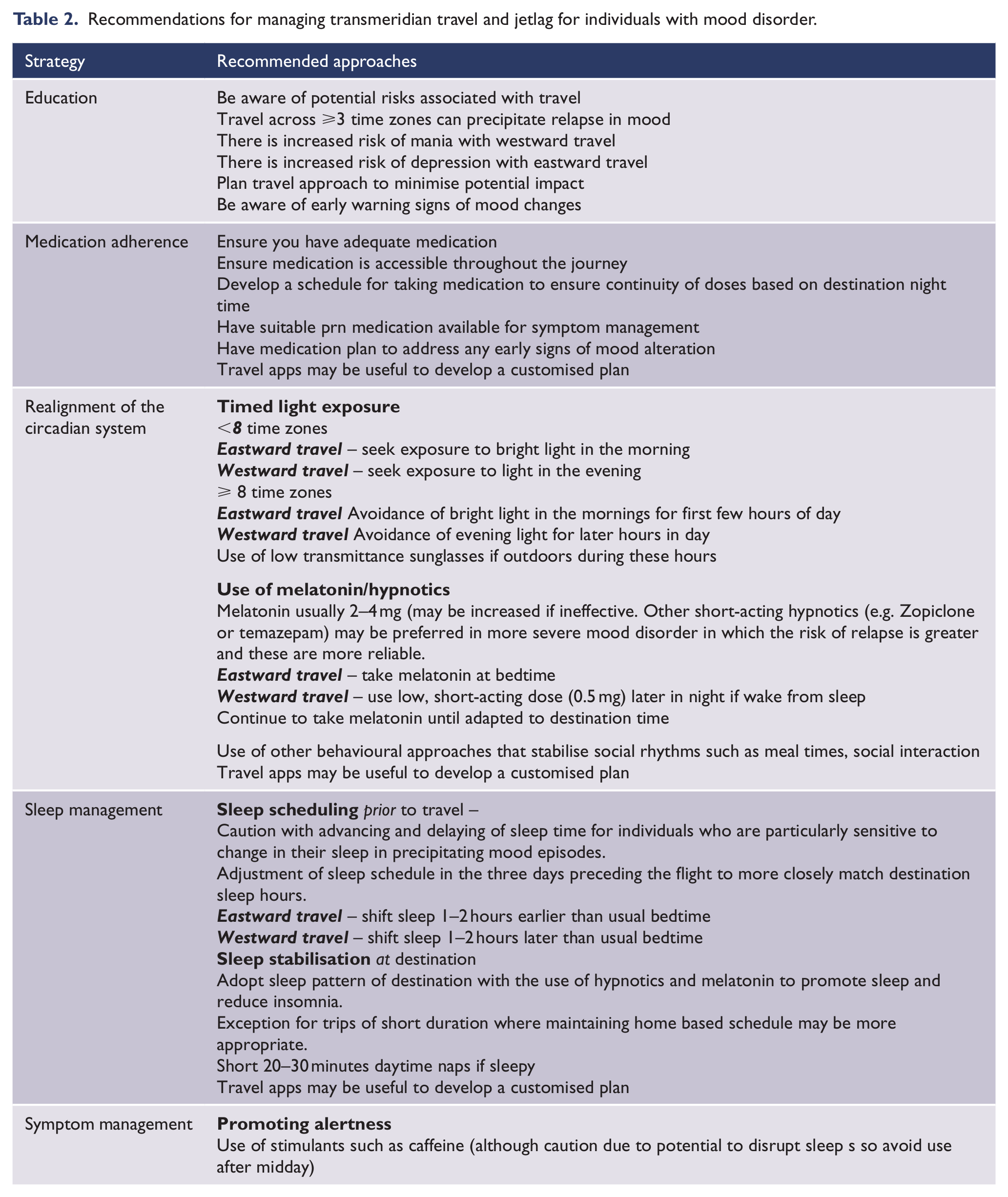
Individuals with mood disorder should be aware of the potential risks in undertaking transmeridian travel. This would enable them to be prepared and to act proactively in addressing factors that may lead to relapse, e.g., insomnia and responding to symptoms indicating a shift in mood. Relevant information would include the potential impact of travel across time zones to precipitate a mood relapse and that the direction of travel may affect the severity of jetlag symptoms and the polarity of a potential mood change. This allows an individual to plan travel schedules that take into account the timing (morning vs evening) and direction of flights (eastward or westward) and planning stopovers. In addition, individuals need to get sufficient sleep prior to travelling so they do not commence the journey in sleep debt. Travelling that allows a reclining position (such as flying first class or business class) is also likely to improve sleep quality (Sack, 2009).
Medication adherence is important in maintaining mood stability and planning a medication regime that includes the scheduling of medication while travelling is essential. Adopting the destination sleep time logically provides an anchor point for planning the medication regime over the course of the journey. Additionally, having a plan for addressing any symptoms changes such as increasing doses or use of additional prn medication may be useful to address early warning signs and further reduce the risk of a relapse. It is also important that the individual has adequate medication and to ensure medication is accessible during travel.
Timed light exposure (Sack, 2009, 2010) and melatonin (Herxheimer and Petrie, 2002; Sack, 2010) can be used to realign the circadian clock. Exposure to light at the destination facilitates adaptation to local time and can be optimised by seeking out or avoiding bright light at appropriate times depending on the direction of travel and number of time zones crossed. For travel up to eight time zones, exposure to bright light in the morning after westward travel and bright light in the evening after eastward travel is recommended. However, when eight or more time zones are crossed, exposure to light can be misinterpreted with dawn perceived as dusk (or vice versa); hence, delayed exposure to morning light after eastward flight and limited exposure to evening light after westward travel for a few days is suggested (Sack, 2009, 2010). Low-transmittance sunglasses or blue blocking glasses can be used to reduce light exposure (Wirz-Justice et al., 2013). These strategies for exposure to light are in keeping with the approach of Interpersonal and Social Rhythm Therapy (IPSRT; Frank, 2005) used for the treatment of bipolar disorder which recognises the importance of disruption in circadian rhythms precipitating mood episodes. IPSRT focuses on stabilising social rhythms such as the timing of going to bed, getting out of bed, mealtimes and going to work, and the daily social stimulation set by the level of social interaction.
Melatonin is a hormone which is used to promote realignment due to its phase-shifting effects (Herxheimer and Petrie, 2002; Sack, 2009). Melatonin has also been implicated in the pathophysiology of mood disorders with alterations in the levels and timings of melatonin secretion (Srinivasan et al., 2006). Melatonin has also been used as a treatment in bipolar disorder (Harvey, 2008). When taken in the evening, melatonin resets the body clock to an earlier time and when taken in the morning resets the clock to a later time. The dose of melatonin varies from 0.5 to 10 mg with the majority of studies using 5 mg. There are also variations in the preparation of melatonin in different countries which makes it difficult to recommend particular doses at this stage. This area requires more research. Larger doses have greater hypnotic effects and thus useful for promoting sleep in addition to its phase-shifting effects (Sack, 2010; Sack et al., 2007). There is some evidence that melatonin may be effective in reducing insomnia in individuals with major depressive disorder at doses 5–10 mg (Srinivasan et al., 2006). Melatonin can be used at bedtime up to 3 days prior to departure and a further 5 days after arrival at destination. After eastward flights, melatonin can be taken at bedtime. For westward flights (where less than 8 time zones are crossed), it is suggested to use low dose short-acting melatonin (0.5 mg or less) later in the night or if awake in early hours of morning as there will be an overlap with endogenous melatonin secretion (Sack, 2009, 2010). Melatonin has been shown to be more effective, the more time zones that are crossed and for travel in easterly direction (Herxheimer and Petrie, 2002).
Sleep disturbance is an identified precipitant to mood relapse (Harvey, 2008; Murray and Harvey, 2010) and stabilising the sleep wake cycle is a core component of IPSRT (Frank, 2005). Sleep management strategies for addressing jetlag include sleep scheduling prior to travel and sleep stabilisation at destination (Sack, 2009, 2010; Sack et al., 2007). Sleep scheduling involves adjusting sleep prior to travel to more closely align with destination sleep hours. For eastward travel, it is recommended to shift sleep 1–2 hours earlier than usual bedtime for eastward travel and delay shift for the same duration for westward travel. It is recommended to adopt the sleep pattern of destination with the use of hypnotics and melatonin to promote sleep and reduce insomnia. The exception to this is for trips of short duration where maintaining the home-based schedule may be more appropriate. For daytime sleepiness, short day naps of 20–30 minutes can be used. Daytime alertness can be promoted by the use of stimulants such as caffeine although there needs to be caution due to the potential to disrupt sleep (Sack et al., 2007). The impact of applying these sleep management strategies for individuals with mood disorder is untested and care may need to be taken with advancing and delaying of sleep time for individuals who are particularly sensitive to changes in their sleep in precipitating mood episodes. The decision regarding whether medication is necessary depends on the number of time zones crossed, degree of stress likely to be occurring on arrival, the severity of previous episodes and the general stability of the illness. In patients with evidence of previous relapses likely to have been associated with transmeridian travel or frequent relapses for other reasons, with severe episodes (in terms of symptoms and consequences) or non-response to melatonin, more aggressive pharmacotherapy, for example, with short-acting hypnotics is justified in order to maintain sleep wake cycle. Without these features, treatment with melatonin may be more appropriate. In very mild mood disorder, neither of these measures may be necessary.
Developments in technology have given rise to travel apps for cellphones to address jetlag and may be a useful tool to enable an individual to develop a customised plan. Examples include Jetlag app (www.jetlagapp.com/), Jetlag rooster (www.jetlagrooster.com/app), and Entrain (http://entrain.math.lsa.umich.edu/). All apps are based on providing a customised plan to address jetlag and focus on sleep scheduling, melatonin use and light exposure. All apps identify they are based on scientific understanding while Entrain has been developed by researchers at the University of Michigan and is the most sophisticated of the apps. While the approach used in these apps is relevant to individuals with mood disorder who travel they are not specially designed for this purpose. However, as the approach is customised, individual needs can be taken into account such as medication scheduling.
Recommendation for future research
The ideal study would randomise a group of patients with a stable mood disorder to one of three groups – fly east, fly west or stay at home. This study is unlikely to happen. We therefore have the following suggestions to advance the field.
Data are unlikely to be generated except by retrospective and careful analysis of travellers who have suffered an episode of mood disorder. Data from large numbers of such patients can still be useful if there is sufficient detail regarding past history, medication, travel, time from travel to symptoms, sleep during travel. Clinics close to International airports could, over a period of years, collect significant data particularly if they routinely use relatively systematic recording of psychiatric history.
Some areas are particularly more likely to see travel-induced episodes of psychiatric illness. New Zealand, for example, in the 4 weeks prior to 15 March 2015 received 79,000 visitors from Asia, 39,000 from the Americas and 53,000 from Europe (Statistics New Zealand, n.d.). All will have travelled across time zones to a variable extent. A system to capture presentations with psychiatric illness of all such travellers would rapidly generate useful data.
Specialist mental health services and psychiatric services worldwide have large numbers of patients with mood disorders under follow-up. A percentage of such patients will travel. These could be matched for important demographic and illness characteristics with non-travelling patients in the same service and rates of relapse compared.
Given the difficulties in this area it may be helpful to analyse in detail and prospectively, a number of patients who have planned travel. Sleep can be studied using actigraphs and mood can be carefully reported throughout the process of travel.
Conclusion
There is very limited evidence that transmeridian travel precipitates episodes of mood disorder which poses difficulties in identifying suitable ways to mitigate the effects of transmeridian travel in mood disorders. Caution needs to be taken in extrapolating the general guidelines for managing jetlag to individuals with mood disorder. However, in the absence of mood-specific guidelines, some guidance can be given based on our current understanding of the relevance of circadian disruption to both jetlag and mood disorders. Further research is required to identify more focused strategies to mitigate the impact of transmeridian travel for individuals with mood disorders.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.