
Abstract

To the Editor
A 46-year-old woman was admitted to our intensive care unit for a inaugural episode of mania (Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV]); the episode was characterized by agitation, irritability, logorrhoea, reckless spending associated with delusional ideas and hallucinations (Positive and Negative Syndrome Scale [PANSS] = 76 and Young Mania Rating Scale [YMRS] = 28). The patient had, 15 days earlier, undergone a subtotal gastrectomy for morbid obesity. The pre-operative psychiatric evaluation revealed no personal or familial psychiatric history. On admission, the neurological examination was normal with no signs of encephalopathy or Wernicke–Korsakoff syndrome. The body mass index (BMI) was 36 kg/m2 on admission and remained stable. Post-operative serum levels of vitamins D and B, folates and zinc were normal excluding the possibility of post-gastrectomy syndrome (by deprivation). Full blood count and brain magnetic resonance imaging were also normal, and serology for hepatitis B/C and HIV were negative.
There is substantial evidence that bipolar disorder can be associated with an abnormal immuno-inflammatory background (Goldstein et al., 2009); therefore, we suspectedthat this inaugural manic episode occurring shortly after gastrectomy could have been induced by altered gut microbiota and intestinal barrier dysfunction (Collins and Bercik, 2009). Consequently, we hypothesized that activated charcoal, a potent adsorbent of inflammatory cytokines (Howellet al., 2006) that neutralizes the effect of inflammatory mediators in the gut, may improve both systemic inflammation and manic symptoms.
After obtaining written informed consent, we collected samples from the patient for immuno-inflammatory testing and prescribed oral activated charcoal treatment at 1 g/day on the basis of calculated adsorption potential (Howell et al., 2006) without any adjunctive psychotropic treatment.
The following markers were tested before treatment and confirmed acute inflammation: (a) circulating pro-inflammatory cytokines (tumour necrosis factor [TNF-α], interleukin [IL]-6, IL-1β and IL-17) and chemokines (IL-8, macrophage inflammatory protein [MIP]-1α and MIP-1β); (b) soluble CD14 isoform (Presepsin®, sCD14-subtype), a pattern recognition receptor that senses and reacts to lipopolysaccharide (LPS) and an inflammation process inducer produced by the commensal gut microflora (Gram-negative bacteria); (c) immunoglobulin-A (IgA) that is directed against mucosal microbiota (Tlaskalová-Hogenová et al., 2004); and (d) monocyte chemoattractant protein 1 (MCP-1), a key regulator of the immune cells involved in inflammatory processes.
Fifteen days after the initiation of charcoal treatment, the patient became asymptomatic (PANSS = 45 and YMRS = 8). The improvement of manic symptoms was substantial and persisted during follow-up (PANSS = 33 and YMRS = 0 at 4 and 8 months) during which the same charcoal treatment was maintained without any psychotropic drugs (Figure 1(a)). In parallel, the titers of all the immuno-inflammatory markers listed above progressively normalized (Figure 1(b)).
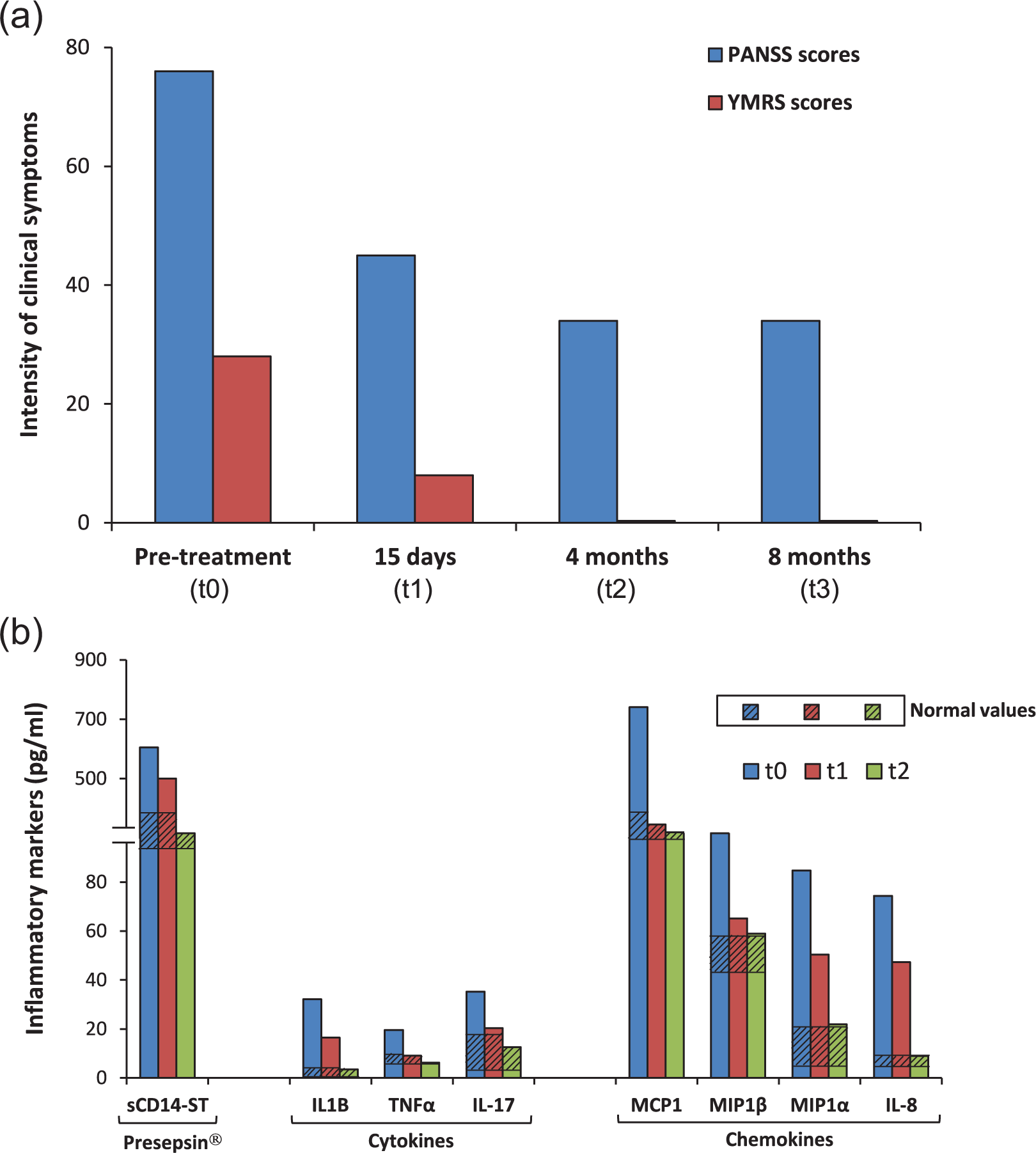
Analyses of (a) manic (YMRS) and delusional symptoms (PANSS) and (b) immuno-inflammatory markers (soluble CD14; cytokines: TNF-α, IL-1, interferon γ and IL-17; chemokines: IL-8, MIP-α, MIP1-β and MCP-1), before treatment (T0) and 2 weeks (T1) and 4 months (T2) after the initiation of charcoal treatment. A fourth time point has been included, showing the clinical assessments at 8 months (T3).
In the present case, severe disruption of the local beneficial commensal equilibrium following gastrectomy may have led to a pro-inflammatory ‘cytokine storm’; inflammatory mediators may have been adsorbed by the activated charcoal, consequently reducing local cytokine transfer from the gut to the bloodstream circulation and thereby to the brain.
To our knowledge, this is the first unambiguous evidence of the efficacy of a non-psychotropic treatment for a manic episode targeting the gut–brain axis, based on monitoring the immuno-inflammatory profile to follow the efficacy of the treatment according to objective biological criteria. Treatment of this manic episode was, thus, both personalized and pathway designed.
Footnotes
Acknowledgements
M.L. and R.T. are co-senior authors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.