
Abstract
Objective:
This review aimed to draw on published literature to identify the prevalence rates of psychiatric disorders in Australia’s Indigenous populations, Aboriginal and Torres Strait Islander peoples.
Method:
A systematic review following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) model was conducted using the following electronic databases: PubMed, Scopus, Web of Science, MEDLINE, PsycINFO, PsycARTICLES, and Informit Indigenous and Health Collections. Studies were included for analysis if they were empirical quantitative studies reporting prevalence rates for any psychiatric disorder in Indigenous people.
Results:
Of the 1584 papers extracted by the search strategy, 17 articles met the eligibility criteria and were reviewed in detail. Methodology, sampling strategy and study design varied greatly across these 17 studies. Prevalence rates varied by disorder and are as follows: major depressive disorder (4.3–51%); mood disorders (7.7–43.1%); post-traumatic stress disorder (14.2–55.2%); anxiety disorders (17.2–58.6%); substance dependence (5.9%–66.2%); alcohol dependence (21.4–55.4%); and psychotic disorders (1.68–25%). While the number of studies on community-based Indigenous populations was limited, available evidence suggested that prevalence rates are higher in prison populations compared with community-based studies.
Conclusions:
It was identified that there is limited evidence on the occurrence of psychiatric disorders for Indigenous people in the general community. More research in this area is essential to provide accurate and reliable estimates and to provide a baseline for evaluating the effectiveness of programs aimed at reducing the high mental health burden experienced by Indigenous Australians. Future research needs to ensure that standardised and validated methods are used to accurately estimate the prevalence of psychiatric disorders among Indigenous Australians.
Keywords
Introduction
Australia’s Indigenous populations, consisting of Aboriginal and Torres Strait Islander peoples, form approximately 2.5% of Australia’s overall population (Australian Institute of Health and Welfare, 2011). It is well established that there is a disparity in health outcomes for Indigenous people compared to the general Australian population, with a greater burden of disease and injury (Vos et al., 2009; Zhao et al., 2004). This is largely due to significantly higher rates of chronic illnesses such as respiratory disease, hearing loss or ear disease, heart and circulatory diseases, diabetes, obesity, and higher blood pressure (Australian Bureau of Statistics (ABS), 2014). Further, life expectancy for an Indigenous person is shorter: estimations include 67.2 years for Indigenous males compared to 78.7 years for non-Indigenous males (a discrepancy of 11.5 years), and 72.9 years for Indigenous females compared to 82.6 years (a discrepancy of 9.7 years), according to the Australian Institute of Health and Welfare (2011).
In all the discussions about health outcomes, however, there is little information on psychiatric disorders in Indigenous Australians. There have been several population studies examining psychological distress and/or social and emotional well-being in Indigenous people (see ABS, 2006; Australian Institute of Health and Welfare, 2011; Cunningham and Paradies, 2012; Gubhaju et al., 2013), or the risk of clinical emotional and behavioural difficulties in Indigenous children and young people (Zubrick et al., 2005). These studies have found that Indigenous Australians tend to have higher levels of psychological distress than the rest of the population, with high or very high psychological distress occurring with at least double the rate in Indigenous people as compared to non-Indigenous people (Australian Institute of Health and Welfare, 2011; Gubhaju et al., 2013). One study found that the occurrence of very high psychological distress was nearly triple the rate in Indigenous people (Cunningham and Paradies, 2012).
A population-based study of Indigenous children and adolescents in Western Australia (WA) found that 24% of Indigenous children in the sample (n=5289) were at high risk of clinically significant emotional or behavioural difficulties, and a further 11.4% were at moderate risk (Blair et al., 2005; Zubrick et al., 2005). In the age range of 12–17 years, 20.5% of Indigenous young people were at high risk of clinically significant difficulties (emotional or behavioural) as compared to 7% of their non-Indigenous peers (Blair et al., 2005). Further, Blair et al. reported that of the Indigenous young people surveyed, 9% of females and 4.1% of males reported they had attempted suicide in the prior 12 months, a concerning statistic.
The population studies discussed above (ABS, 2006; Australian Institute of Health and Welfare, 2011; Blair et al., 2005; Cunningham and Paradies, 2012; Gubhaju et al., 2013) have indicated that Indigenous people experience greater psychological distress and have a greater likelihood of psychiatric difficulties than their non-Indigenous counterparts. These studies, however, do not comment on nor do they explore the actual rates of psychiatric disorder in Indigenous people. This type of exploration is warranted given that the health outcomes are worse for this population. Further, population statistics show that in the period 2008–2009, Indigenous people accessed community mental health services almost three times more than non-Indigenous Australians (Australian Institute of Health and Welfare, 2011). These figures could be higher, however, as these statistics represent the contacts where Indigenous status was actually recorded; one study’s audit of health records at one location indicated that only 84.8% of Indigenous people were correctly identified as such (Haswell et al., 2013).
The primary objective of this review is to determine the prevalence rates of psychiatric disorder in Australia’s Indigenous populations. This is achieved by examining published literature on the rates of Axis I disorders from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR; American Psychiatric Association, 2000), the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013), or the International Classification of Diseases, 10th Revision (ICD-10; World Health Organization, 1992) in Indigenous groups. This includes psychiatric disorders under the following categories: mood, substance use, psychotic, anxiety, somatoform, eating, and adjustment disorders.
Method
Search strategy
The Preferred Reporting Items for Systematic reviews and Meta-Analyses model (PRISMA; Moher et al., 2009) was followed (Figure 1). Articles published between January 1994 and July 2014 were included. The following search terms were used to search electronic databases.
‘Indigenous’ AND ‘Mental Health’ AND ‘Prevalence’ AND ‘Australia’.
‘Aboriginal’ AND ‘Psychiatric’ AND ‘Prevalence’ AND ‘Australia’.
A MEdical Subject Heading (MESH) term search was also conducted specifically in PubMed’s MESH databases, using the following terms: ‘Australia’ AND ‘Indigenous Population’ AND ‘Psychiatric Diagnosis’.
Flow chart of the literature search strategy.
The following databases were searched: PubMed; Scopus; PsycINFO and PsycARTICLES; Web of Science; MEDLINE (via EBSCOHOST); and Informit Health and Indigenous Collections. Results were retrieved on 28 July 2014 and imported into an Endnote X7 database (Thomson Reuters, 2013). Duplicate entries were identified and deleted with Endnote’s duplicate identification function (n=434). The remaining articles were sorted alphabetically and then visually scanned to identify any missed duplicates: a further 55 papers were removed following manual inspection. Titles and abstracts were reviewed to exclude non-relevant papers, followed by full-text review (Figure 1). Two authors (EB and SK) reviewed potential papers for inclusion. The reference lists of included articles were inspected to identify potential additional relevant studies (snowball sampling). At this point the search was widened to include governmental reports, as these can involve large-scale community surveys of health indicators that are not necessarily published in peer-reviewed or indexed journals. A further targeted search was completed using the ABS, Australian Institute of Health and Welfare, and Cochrane Library sites to further add any reports that may not have been mentioned in reference lists. Full reports of the studies and reports identified from snowballing and targeted searches were reviewed to determine eligibility.
Inclusion criteria consisted of the following:
Peer-reviewed journal articles of empirical quantitative studies published in English-language journals. During the snowballing phase, it was decided to widen this to include reports and statistics provided by government organisations and reports.
Australian Aboriginal or Torres Strait Islander Indigenous populations used in the sample.
Prevalence data for any Axis I psychiatric disorder reported. This includes mood, anxiety, substance use, psychotic, eating, and adjustment disorders.
Studies recruiting participants across the lifespan.
Studies were excluded if:
The focus was not Indigenous Australians.
The sample consisted of non-Indigenous participants combined with the Indigenous sample and it was not possible to directly identify prevalence rates for the target group.
Psychiatric illness was not considered (e.g. the paper examined tobacco smoking, completed suicide data, primary health data, or dementia).
No prevalence statistics for psychiatric illnesses were reported.
Substance use and abuse was not considered by the current review (although substance dependence was included due to the focus being on disorders).
Studies used measures or assessments of mental health that did not provide a diagnosis due to diagnosed disorders being the focus of the current paper.
Study quality
Study methodology was assessed by two authors (EB and SK) using Loney et al.’s (1998) method. This uses an eight-point scale covering the following areas: sampling method, frame, and size; measures used; potential assessor bias; response rate and influences; confidence intervals and subgroup analyses; and participant description. The higher the score obtained, the stronger the methodology.
Results
Studies identified
A total of 17 studies that examined the prevalence rates of psychiatric disorder in Australia’s Indigenous people were identified (search strategy presented in Figure 1). The majority of these (n=14) were published within the last 5 years, demonstrating increasing interest in recent times. Sample sizes across studies varied greatly, from 34 participants up to 10,588 participants. Participants were at varying stages of lifespan, from 10 years up to 89 years of age. Sample types also varied broadly, including community samples (n=4), Aboriginal Medical Service (AMS) users (n=4), incarcerated samples (n=8), and people in contact with a mental health service (n=1). Methodology, sampling strategy, and study design varied greatly between studies, evidenced by methodology ratings from 2 to 7 (Table 1); one study was unable to be ranked due to a lack of information provided. Further, the way disorders were determined also varied between studies, with assessment methods including: structured diagnostic interview schedules administered by clinicians (n=4); screening tools followed by medical interview (n=2); questionnaires or rating scales administered in writing or verbally via interview (n=5); clinician interview based on diagnostic criteria (n=1); psychiatrist assessment (n=1); diagnosis entered on a medical database (n=2); self-report of diagnosis (n=1); or the assessment of the disorder not being reported (n=1).
Information and description of studies included in the review.
Sample characteristics described, including ethnicity, sex, age (range and mean), and location.
The sampling and recruitment strategy used by the study are briefly described, as well as the location of the study and sample type.
This column considers how the disorders were assessed or measured, and the tools used for this.
Loney et al.’s system for scoring study methodology, previously described in the Results section.
AHW: Aboriginal health worker; AMS: Aboriginal Medical Service; AUDIT: Alcohol Use Disorders Identification Test; BDI-II: Beck Depression Inventory-II; CIDI: Composite International Diagnostic Interview; DD: depressive disorder; GP: general practitioner; ICD-9: International Classification of Diseases, 9th Revision; ICD-10: International Classification of Diseases, 10th Revision; IHD: ischaemic heart disease; KICA-dep: Kimberley Indigenous Cognitive Assessment of Depression; MDD: major depressive disorder; NSW: New South Wales; NT: Northern Territory; OCD: obsessive-compulsive disorder; PHQ-9: Patient Health Questionnaire-9; PTSD: post-traumatic stress disorder; QLD: Queensland; SDS: Severity of Dependence Scale; SSRI: selective serotonin re-uptake inhibitor; TSI: Torres Strait Islander; WA: Western Australia; WHO: World Health Organization.
Analysis
The diversity of methodologies and settings, as well as missing data, meant that statistical pooling was neither possible nor appropriate; results are therefore restricted to a narrative synthesis. Findings are therefore charted and summarised consistently with Arksey and O’Malley’s (2005) recommendations for scoping reviews.
Indigenous prevalence rates of psychiatric disorder
Major depressive disorder
Twelve studies were identified that examined the rates of major depressive episodes (MDE) and major depressive disorder (MDD), which involves single or recurrent episodes of MDE (American Psychiatric Association, 2000) (Table 2). MDD rates varied between 4.3% and 51%. The lowest rates were found in community samples (n=3), ranging between 4.3% and 22.3%. Samples recruited through Aboriginal Medical Services (AMS; n=3) showed slightly higher ranges, from 8.8% up to 26.7%. Prison samples (n=6) had the highest prevalence rates and greatest variability of MDD, between 12.4% up to 35.4% for sexes combined (sex-specific rates are reported in Table 2). When sex was considered, one study found the prevalence of MDD reached 51% in females for 1-year prevalence (Indig et al., 2010).
Prevalence rates of major depressive and mood disorders.
Disorder present within the last month.
Disorder present within the last year.
Disorder present at any point over someone’s lifetime.
Prevalence rate for both males and females.
Mood disorders
Four studies were identified that considered mood disorders as a group, which included MDD, manic episodes, mixed episodes, bipolar disorders, dysthmic disorder, depressive disorder not otherwise specified, and adjustment disorder with depressed mood (Table 2). Only one community study was available, which identified the current prevalence of mood disorders at 7.7% (Almeida et al., 2014); not all of the mood disorders listed above were assessed in this study, however. Three studies involved prison samples, which found prevalence to vary from 10.4% (in males) up to 43.1% (in females). Variability was quite wide between studies, sex, type of prevalence considered, and assessment of diagnosis.
Post-traumatic stress disorder
Four studies measured PTSD (Table 3). Three of these used prison samples, where rates varied between 14.2% (in males, current prevalence) up to 49.2% (in females, for 1-year prevalence). The highest rate of PTSD obtained was in the only community study identified (Nadew, 2012), which found PTSD to be 55.2%; Nadew’s study was also the only one to employ lifetime prevalence.
Prevalence rates of anxiety disorder diagnoses (PTSD, OCD, GAD, panic disorder, social phobia, agoraphobia, specific phobia).
Panic disorder, social phobia, agoraphobia, specific phobia, obsessive-compulsive disorder, generalised anxiety disorder, anxiety disorder not otherwise specified.
Includes all the above plus PTSD.
GAD: generalised anxiety disorder; OCD: obsessive-compulsive disorder; PTSD: post-traumatic stress disorder.
Anxiety disorders
Four studies considered anxiety disorders, which included: PTSD; obsessive-compulsive disorder (OCD); generalised anxiety disorder (GAD); panic disorder; social phobia; agoraphobia; specific/simple phobia; and anxiety disorder not otherwise specified (ADNOS) (Table 3). Of these, one was a community study that found lifetime prevalence to be 17.2%. Three prison studies obtained much higher prevalence rates; for example, one that used lifetime prevalence found this to be 34.3%. Other prison samples found anxiety disorders to be higher in females (up to 58.6%, for 1-year prevalence) than in males (up to 24% for current prevalence).
Substance dependence
This included the diagnoses of dependence for the following substances: cannabis; alcohol; amphetamines; opioids; sedatives; or ‘other’. Five studies provided prevalence data on substance dependence (Table 4). Two community studies found rates of 5.9% (lifetime prevalence) and 32.3% (current prevalence). This indicates that substance dependence can vary widely depending on the substances assessed, location, and community itself. Three studies recruited prison samples, which found rates of 46.8% up to 66.2%.
Prevalence rates for alcohol and substance dependence.
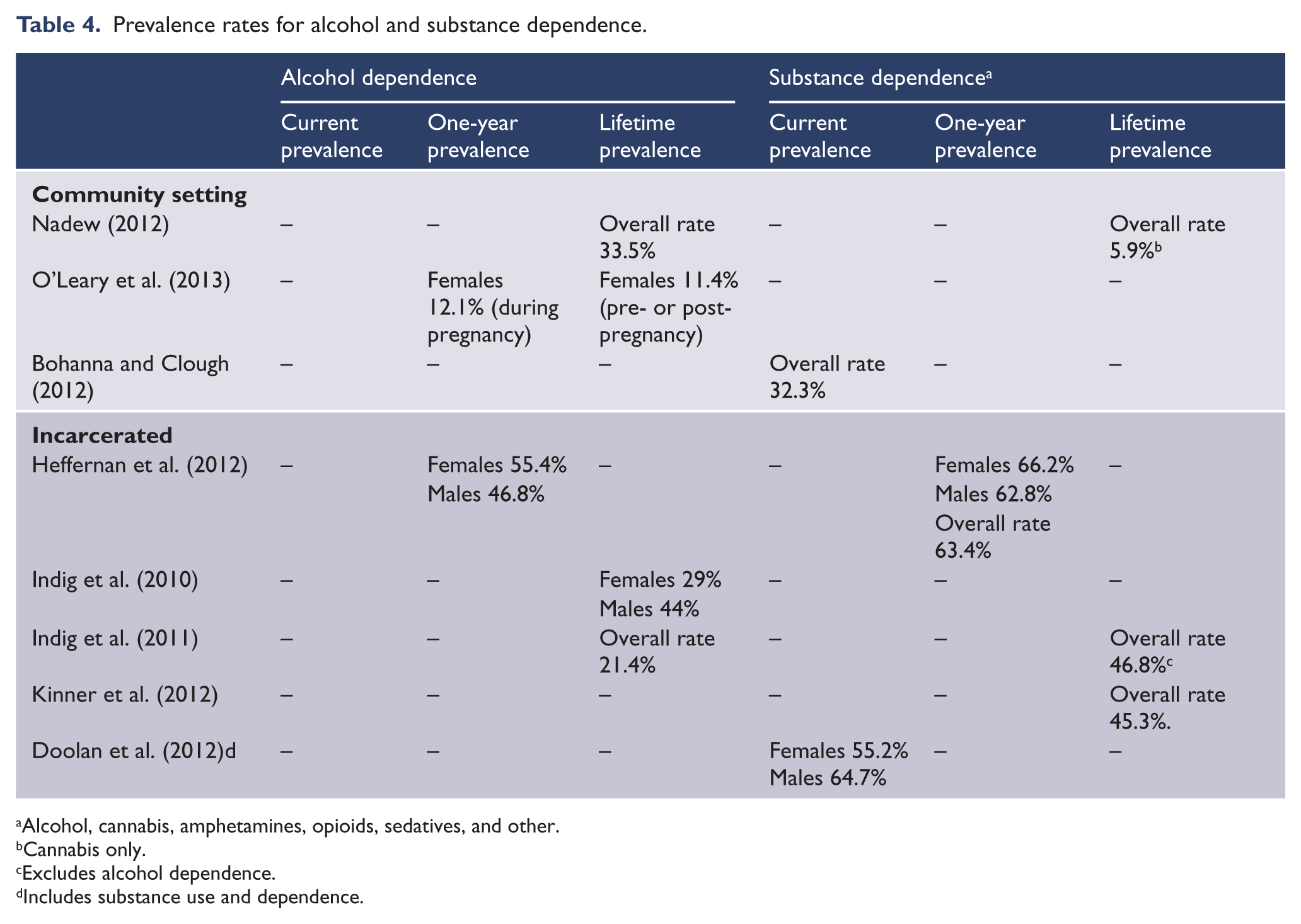
Alcohol, cannabis, amphetamines, opioids, sedatives, and other.
Cannabis only.
Excludes alcohol dependence.
Includes substance use and dependence.
Alcohol dependence
Six studies were available that provided prevalence data (Table 4). The lowest rate obtained was in the health records of pregnant Indigenous women, at 11.4% (O’Leary et al., 2013); the authors do note, however, that this may not be an accurate finding due to significant variability in whether health providers assessed alcohol use or not. One community study found lifetime prevalence of alcohol dependence to be at 33.5% (Nadew, 2012). Four studies used prison samples, which tended to find much higher rates generally, from 21.4% up to 55.4%.
Psychotic disorders
Three studies were available regarding psychotic disorders (Table 5). Under this category, the following were included: psychotic symptoms; schizophrenia/schizophrenia-related disorders; substance-induced psychotic disorder and substance use-related psychosis; schizoaffective disorder; mood disorder-related psychosis; psychotic disorder not otherwise specified; organic-related psychosis; acute and transient psychoses/brief psychotic disorder. One study provided data on people living in the community who were already engaged with a mental health service for treatment of their disorder (Hunter et al., 2012); current prevalence was estimated at 1.68%, which was determined by considering the number of service users against the number of people living in the communities considered. This, however, would miss people who may have psychotic symptoms or disorders who were not engaged with the mental health service.
Prevalence rates for psychotic disorders.
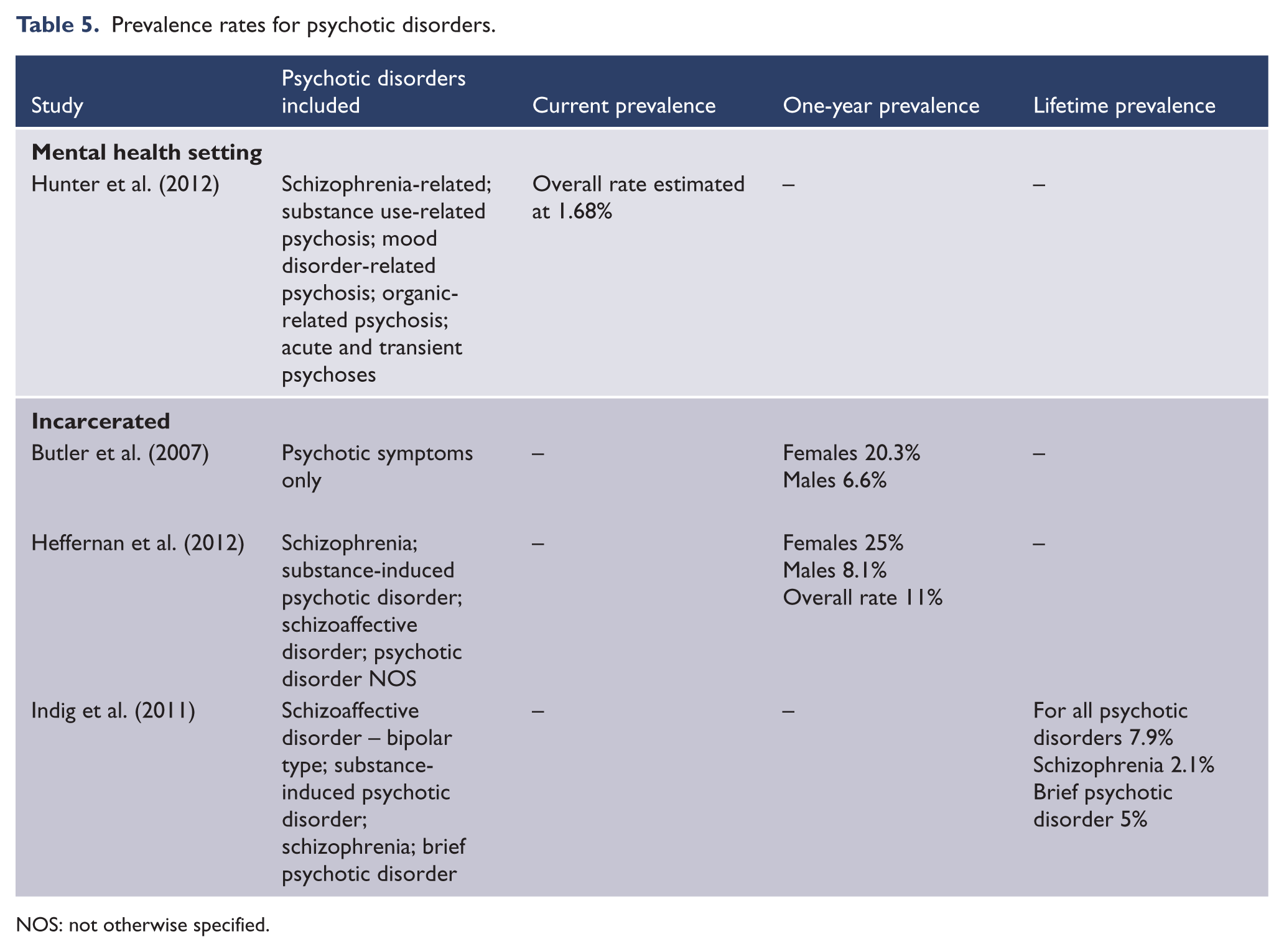
NOS: not otherwise specified.
Two prison studies found prevalence to vary between 7.9% up to 11%; when sex was separated, one study found a 1-year prevalence rate of 25% in females. Lifetime prevalence of schizophrenia was found to be 2.1% and 5% for brief psychotic disorder in one prison study (Indig et al., 2011).
Adjustment disorders
One study was identified that had considered adjustment disorder with depressed mood (Almeida et al., 2014); however, this was done in the context of assessing major depression. Therefore, this study was included in the mood disorders section. No research was identified that assessed adjustment disorders as a whole.
Eating disorders
No studies were identified that assessed eating disorders.
Somatoform disorders
No studies were identified that assessed somatoform disorders.
Discussion
Overall, these findings demonstrate quite high rates of psychiatric disorder in Indigenous participants, with some studies finding approximately half of participants experiencing disorders such as major depression, PTSD, anxiety, and alcohol or substance dependence. As would be expected, psychotic disorders had the lowest prevalence (with the highest rate at 25%). As noted, these elevated prevalence rates found across the disorders typically employed samples of incarcerated Indigenous people.
Prison and detention samples were the most commonly used sample in the literature; only three studies were identified that recruited community samples. It is likely that there are a greater number of studies available using samples of incarcerated people (as opposed to community studies), as essentially this poses a simpler sampling strategy with a contained recruitment pool. Although easier to conduct, they may not be representative given the increased prevalence of mental disorders amongst inmates overall (e.g. Butler and Allnutt, 2003; Prins, 2014). The only exception to this was one community study which found the highest rate of PTSD (55.2%; Nadew, 2012). This is likely to be the result of several factors; for instance, lifetime prevalence was used, whereas the prison studies examining PTSD employed current or 1-year prevalence. Further, there was potential bias influencing in this study as one of the criteria used to select the three Indigenous communities for this study included exposure to observable traumatic events: 97.35% of participants in these communities reported experiencing a trauma. Therefore, even though this study recruited a community sample, it may not be a representative one.
The most commonly researched disorders were depression, followed by alcohol dependence. This may be due to depression being a leading burden of disease for health in Australia generally (Begg et al., 2008; Mathers et al., 2000). Alcohol use may have been focused on in this population due to it being identified as one of the main risk factors contributing to the disparity in health outcomes for Indigenous people (Vos et al., 2009). This is despite evidence that Indigenous people report drinking at risky or high risky levels at an equivalent rate to non-Indigenous people (post-age adjustment): 15% and 14%, respectively (ABS, 2006). Further, in this survey, 10% of Indigenous people reported never having consumed alcohol and 14% reported not having consumed alcohol in the year prior to the survey. The ABS classified 32% of Indigenous people’s alcohol consumption as being in the low-risk range (the authors report this was determined by guidelines from the National Health and Medical Research Council). Therefore, it appears that whilst alcohol is not being consumed at risky levels any more than in the general population, when alcohol is consumed it has a much greater health impact on Indigenous people.
Limitations
Several Axis I disorders were not considered in the literature: eating disorders, somatoform disorders, and adjustment disorders. One study did consider adjustment disorder with depressed mood; however, this was part of their exploration of depressive disorders (Almeida et al., 2014), and not types of adjustment disorder. One study was identified that did examine disordered eating behaviours in Indigenous people (Hay and Carriage, 2012), but it did not meet inclusion criteria due to not being a diagnostic study. A variety of factors may explain why eating, somatoform, and adjustment disorders are missing from the literature, such as likelihood of occurrence: eating and somatoform occur less frequently than disorders such as MDD (American Psychiatric Association, 2000, 2013). The assessment tools used could also explain why these disorders are absent from the literature; for example, the Composite International Diagnostic Interview (CIDI) does not assess eating, somatoform, or adjustment disorders. Further, as previously noted, most studies were focused on assessing major depression and alcohol use disorders, for which targeted measures exist. Another potential influence may be that these disorders are not seen as culturally relevant or appropriate; for example, given the poor health outcomes for Indigenous people, to be exploring somatoform disorders may result in misdiagnosis of genuine physical conditions and therefore poorer treatment outcomes. These hypotheses are speculation, however, as there is no evidence as to why some Axis I disorders have not been assessed in this population. It is to be expected that there are gaps in the literature, given that there is not a strong evidence base to begin with for the occurrence of any psychiatric disorder in Indigenous community populations.
The studies reviewed used methods of varying quality and standardisation to determine psychiatric disorder, including clinical assessment, self-report instruments, and diagnostic interviews. These various methods are also likely to contribute to inconsistency in findings. Further, the type of prevalence employed was not consistent across studies, with studies using current, 1-year, or lifetime prevalence of disorder. This will also contribute to variability in results, as using narrower criterion (current prevalence) versus broader criterion (lifetime prevalence) will produce different rates of occurrence.
Some research acknowledged that the assessment tools used had not been validated for use with Indigenous people (e.g. see Kinner et al., 2012). This is a major concern as it may not be appropriate to apply Western nosology to a native population. If the tools used to determine psychiatric illness are not valid, then this is likely to be over-, under-, or misdiagnosed, resulting in inaccurate results. Two studies were identified in this review that aimed to validate the measures employed: the Kimberley Indigenous Cognitive Assessment of Depression (KICA-dep; Almeida et al., 2014) and a modified Patient Health Questionnaire-9 (PHQ-9) (Esler et al., 2008) both aimed at identifying depressive symptoms. Esler’s study provided only preliminary support for the PHQ-9 due to the small sample size (n=34); both validation studies identified their measures as having a strong negative predictive value, rather than positive prediction. That is, these measures were better at identifying people without depression than they were at identifying people with depressive symptoms. Further, the PHQ-9 and KICA-dep tools are not diagnostic ones (i.e. they cannot be used to diagnose depression); rather, they are both screening measures that may identify some symptoms of depression. Therefore, validation of diagnostic tools (such as the CIDI) is required in Indigenous people to determine whether they can accurately diagnose psychiatric illness, or not. This gap in the literature needs to be addressed as a priority in order to ensure further research into the prevalence of psychiatric disorders in Indigenous people is actually valid.
Sample sizes varied broadly between studies, with one study utilising 34 participants (Esler et al., 2008), and another having 10,588 (O’Leary et al., 2013). Regarding prevalence and incidence statistics, it has been recommended as a general rule of thumb in order to obtain adequate data and error sizes that the sample size is at least 300 participants (Loney et al., 1998). The current review only identified four studies with sample sizes greater than or equal to 300 Indigenous participants; three of these were prison samples (Doolan et al., 2012; Heffernan et al., 2012; Indig et al., 2010), and the remaining studies involved data pulled post hoc from medical databases (O’Leary et al., 2013; Si et al., 2011). It is worth noting, however, that some of the community samples used in studies may not have a population of 300 people living in the community. This is not possible to determine for some studies, however; for example, the Nadew (2012) study kept the communities sampled confidential, and as response/refusal rates were not reported, the overall population of these communities is not able to be determined.
Studies varied greatly in methodology: as previously discussed, there have been wide variations in ascertainment, sample size, and sample type. One study (Egger and Butler, 2000) was unable to be rated on their methodology due to a lack of information provided. The research studies with the strongest methodology (reaching 7/8) were all prison studies (Heffernan et al., 2012; Kinner et al., 2012); as previously noted, this, however, is not representative of the general population and is likely to present inflated prevalence rates. Community studies with stronger methodology (Almeida et al., 2014; O’Leary et al., 2013) also cannot be used as representative of Indigenous people generally, due to the specific samples recruited (aged people and expecting mothers, respectively). Studies which did occur in communities (Bohanna and Clough, 2012; Nadew, 2012) were not as strong in their methodology (see Table 1) and involved potential bias in their recruitment strategies: Bohanna and Clough’s study involved opportunistic sampling at various locations (with a small sample recruited, n=133), relying on participants being at these locations during the sampling time; and potential bias has previously been discussed for Nadew’s study. Therefore, these studies may also not be representative of Indigenous communities/populations as a whole.
This review highlights that existing studies do not provide accurate and generalisable estimates on rates of psychiatric disorder in Indigenous Australians. This is due to the limitations of existing studies, variable methods and therefore findings, and the use of specific subgroups not representative of the broader population. Further, it is to be noted that even if a range of methodologically sound community prevalence studies were available, that rates of psychiatric disorder would likely vary across communities. This is because Australia’s Indigenous populations are not a homogenous group, but rather encompass a diverse array of cultures, languages, countries, and histories. Given the diversity that exists, each community group will have their own varying challenges, difficulties, and rates of disorder. This hypothesis has some preliminary indications of support through population research which has found that Indigenous people living in non-remote areas are more likely to report higher rates of mental illness than people living in remote locations (Australian Institute of Health and Welfare, 2011). It has also been shown that there is a greater burden of disease experienced by Indigenous people for psychiatric disorder (included substance use disorders) in non-remote locations versus remote locations (14% and 4%, respectively; Vos et al., 2009). Further, Indigenous people living in remote locations report greater positive well-being than other locations, despite being more likely to experience life stressors such as higher rates of deaths of family or close friends, overcrowding, and alcohol-related difficulties (Australian Institute of Health and Welfare, 2011). Determining prevalence rates in future research across Indigenous people will likely obscure diversity between communities, groups, or areas; regional analysis may also need to be employed.
In recent years, the quality and accountability of codes of good research practices among Indigenous health are improving. For instance, both the National Health and Medical Research Council (NHMRC) and The Australian Institute of Health and Welfare have developed ‘Best Practice Guidelines’ for health data collection. These national standards are aimed at ensuring consistency in methodologies applied when collecting and recording data. Even though such guidelines are available from national agencies, no national studies on mental health among Indigenous Australians have been done so far. Apart from costs, the reasons can be multifactorial, including the lack of coordinated approaches to ‘closing the gap’, the logistics of conducting mental health surveys in regional and remote areas and a lack of experienced mental health professionals to conduct structured diagnostic interviews. However, with the recent successes in conducting the National Aboriginal and Torres Strait Islander Health Survey (NATSIHS, 2012–2013), including complex biomedical components (blood and urine tests), it is feasible to incorporate mental health interviews as part of such national health surveys. It will be cost-effective if standardised mental health assessments are carried out in conjunction with the next wave of the NATSIHS (planned by the ABS for 2018–2019). Such a conjoint survey will be culturally appropriate in Indigenous settings and avoid the traditional siloed approaches to mental and physical health. Moreover, such an approach will not only illuminate the prevalence of mental health conditions among Indigenous Australians, but also help understand the link between mental and physical health conditions at the same time. This will inform national policies and help develop a coordinated approach to ‘close the gap’ by 2030.
Conclusions
The current review has identified that there are large gaps in our knowledge of psychiatric morbidity among Indigenous Australians. Further research is needed to determine the rates of psychiatric disorder in Indigenous people in the general community, with attention paid to standardised and validated methods and tools. Obtaining accurate and reliable prevalence estimates will help identify priority areas and provide baselines measures for evaluating the effectiveness of programs aimed at reducing the high mental health disease burden experienced by Indigenous Australians.
Footnotes
Funding
This study was partly funded by NHMRC grant #APP1061963, and the Rural Clinical Training and Support program from the Australian Government Department of Health (previously Department of Health and Ageing).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.