
Abstract
Objective:
To examine the evidence for non-pharmacological interventions in the treatment of moderate to severe depression in an inpatient setting.
Method:
An integrative review of original research papers was conducted. The electronic databases CINAHL, MEDLINE and PsychINFO were searched using the following search terms: depression, psychosocial, psychosocial intervention, therapy, and inpatient.
Results:
Twelve studies were identified in the search for non-psychopharmacological interventions for depression commenced in an inpatient setting. The interventions included psychotherapies, behavioural activation, and chronotherapeutic interventions (controlled exposure to environmental stimuli). These studies suggest it is possible to engage severely depressed inpatients in structured interventions in an inpatient environment. The majority of studies reported favourable outcomes for the interventions compared to a control, but methodological issues were common.
Conclusions:
A diverse range of treatment strategies has been identified in this review. These studies provide evidence that non-pharmacological treatments for depression can be given to enhance outcomes and that research can be undertaken in inpatient settings. Whilst the evidence base has limitations, this review also highlights therapeutic and research opportunities in this area.
Introduction
Depression is a leading cause of disease burden worldwide (Murray et al., 2012). Whilst the majority of depressive episodes are managed in the community, mood disorders including depression are one of the most common diagnostic categories in inpatient services in New Zealand and the United Kingdom (29% and 40%, respectively) (Thompson et al., 2004; Wheeler et al., 2011). In most jurisdictions, the inpatient environment is a limited resource that is reserved for occasions when treatment in the community is no longer feasible. As a consequence, inpatient treatment of depression is generally recommended when other resources (staying with friends, family or respite accommodation) are unable to be utilized and the severity of depression requires a hospital setting for reasons of suicidality, self-neglect, or severe distress (Ellis et al., 2004). However, in some health systems, inpatient management of depression may also service a wider population and act as an alternative to community treatment as opposed to an intervention of last resort (e.g. Germany) (Sitta et al., 2006).
Acute inpatient services are often criticized for being inadequate in providing therapeutic environments (Walsh and Boyle, 2009). Surveys of mental health inpatient consumers consistently highlight a range of concerns about inpatient environments including the lack of people to talk to, an over-reliance on medication, and boredom (O’Hagen, 2006). These concerns have emerged as the focus has shifted to non-acute community-based services following the deinstitutionalization of large psychiatric hospitals. Over this period there has also been a drive to reduce inpatient admissions and find alternate models of care; as a consequence, inpatient services have been relatively neglected for service development and research initiatives (Bowers et al., 2009).
The deinstitutionalization process coupled with a focus on improving community services now means that inpatient services provide care for those with complex needs and challenging behaviour, often under mental health legislation (Lelliot and Quirk, 2004). Providing care in this environment is challenged by competing imperatives of financial restraint, risk management and therapeutic treatment. It has been suggested that in many cases the sole focus of psychiatric inpatient treatment has become safety and crisis stabilization rather than therapeutic benefit (Glick et al., 2011), and that this emphasis has provided the context for clinicians to perceive inpatient treatment as driven by the needs of the organization rather than the patient (Fourie et al., 2005).
Despite these concerns, most commentators still regard inpatient services as a necessary part of a comprehensive health care system (Bowers et al., 2009; Glick et al., 2011; Lelliot and Quirk, 2004). Guidelines propose that inpatient treatment of depression consists of pharmacological strategies with or without the addition of adjunct psychotherapy (typically cognitive behavioural therapy (CBT) or interpersonal psychotherapy (IPT)) (Ellis et al., 2004). However, there is clearly a need to improve care because of the criticisms outlined above, as well as other factors such as high readmission rates to psychiatric hospitals and low application of strategies such as psychotherapy in inpatient settings (Sainsbury Centre for Mental Health, 2010). Treatments in inpatient settings are a relatively undeveloped area of psychiatry (Crowe and Porter, 2014). In this paper, we review non-medication treatment strategies for inpatient depression in order to provide guidance to clinicians and services planning inpatient care of depression and to guide future research.
Method
The aim of this paper is to review whether non-pharmacological interventions for depression, delivered in an inpatient environment, are effective in improving symptoms of depression.
We searched CINAHL, MEDLINE and PsychINFO using the following terms: depression, depressive disorder, psychotherapy, chronotherapy, exercise, inpatient, and hospitalization to identify papers for review. We cross-referenced studies found by this strategy to identify further papers for review. The inclusion criteria for the review were:
interventions for the treatment of depression;
interventions commenced in an inpatient setting;
moderate to severe depression as inclusion criterion;
adult participants (age 18–65 years);
measurement of mood severity as outcome;
depression severity on entry to study provided;
any date of publication before July 2014;
English language.
The exclusion criteria were:
outcomes not separated by diagnosis (i.e. studies presenting results in relation to all inpatients irrespective of diagnosis);
highly select inpatient groups (e.g. those with depression and co-morbid alcohol dependency);
elderly patients within a geriatric context.
The quality of the identified trials was assessed using the Cochrane Collaboration’s tool for assessing risk of bias (Higgins and Green, 2011):
sequence generation;
allocation concealment;
blinding of participants;
incomplete outcome data;
selective outcome reporting;
other sources of bias.
Studies were then assessed as low risk of bias, unclear risk of bias, or high risk of bias.
A second assessment of quality involved examining the process of ensuring the fidelity in the delivery of interventions – training, manualization, adherence to model, competence in delivery. Figure 1 illustrates the search process as a flow diagram.
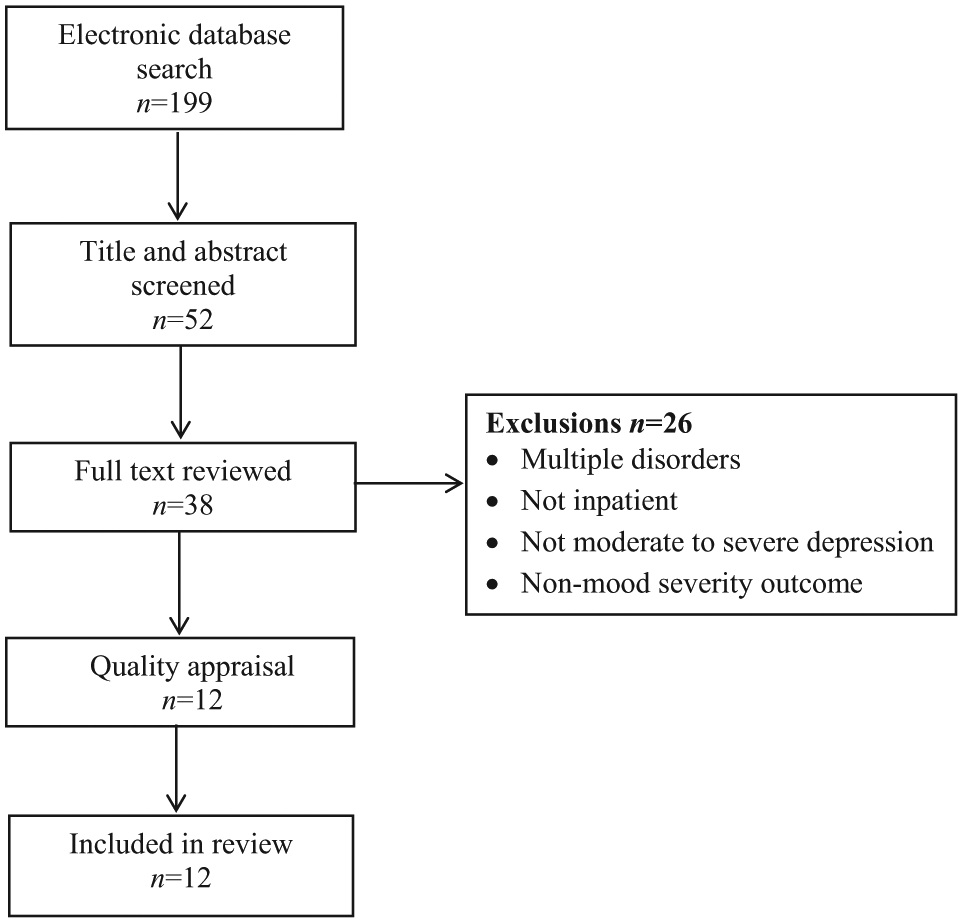
Flow diagram of search process.
Results
Twelve studies were included in the review, with their key features summarized in Table 1, including the intervention, inclusion and exclusion criteria, sample size, baseline measure of severity, and main outcomes. The number of participants in each study ranged from 20 to 432. Most studies recruited patients with very severe or severe depression (n=8) and the other studies recruited participants with moderate to severe depression. The majority of studies were randomized controlled trials although two were pre- and post-intervention naturalistic studies. Most studies were conducted in Europe, with one conducted in Australia and one in the United States.
Characteristics of the included studies.
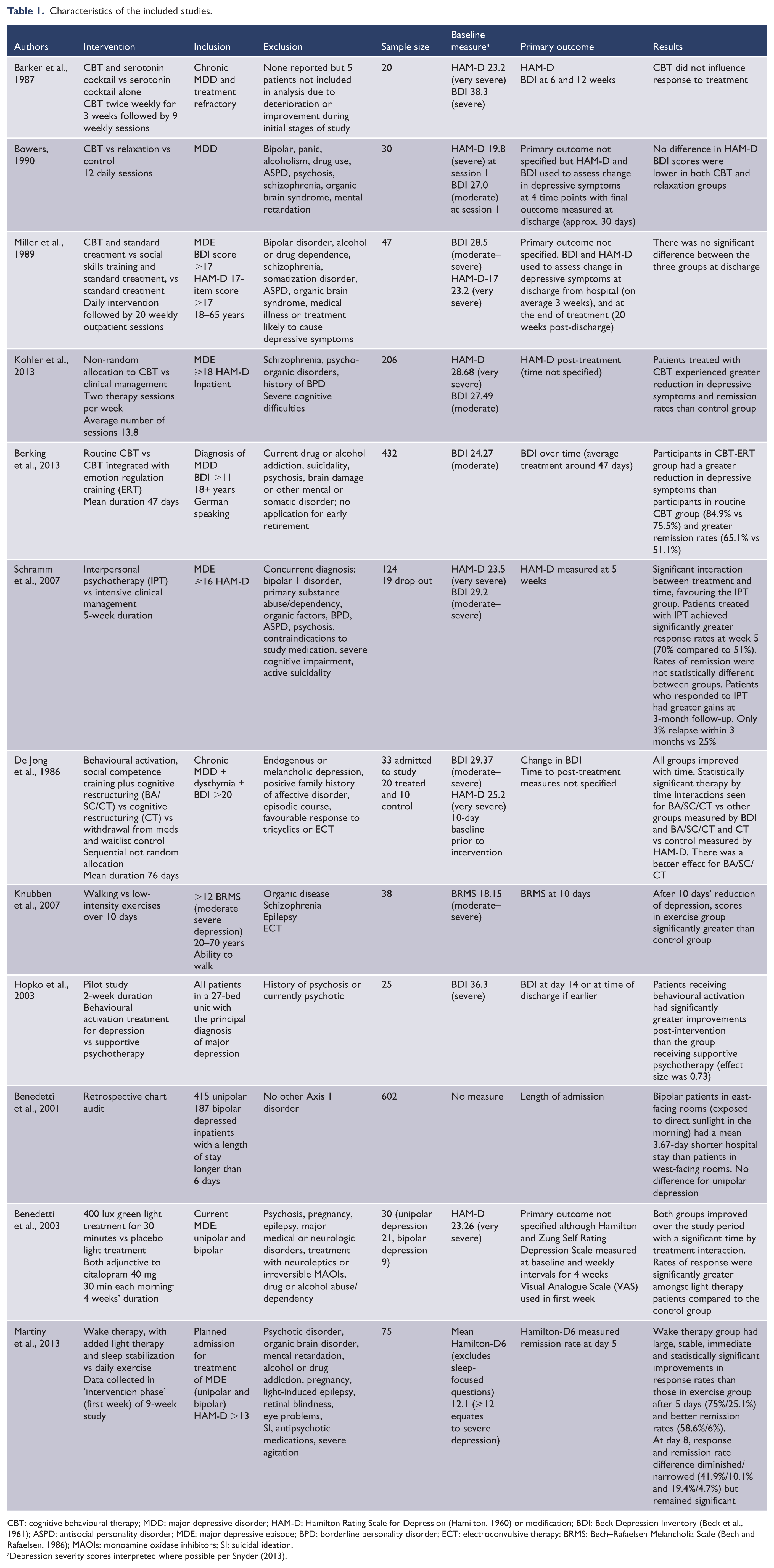
CBT: cognitive behavioural therapy; MDD: major depressive disorder; HAM-D: Hamilton Rating Scale for Depression (Hamilton, 1960) or modification; BDI: Beck Depression Inventory (Beck et al., 1961); ASPD: antisocial personality disorder; MDE: major depressive episode; BPD: borderline personality disorder; ECT: electroconvulsive therapy; BRMS: Bech–Rafaelsen Melancholia Scale (Bech and Rafaelsen, 1986); MAOIs: monoamine oxidase inhibitors; SI: suicidal ideation.
Depression severity scores interpreted where possible per Snyder (2013).
In six studies, the intervention studied was a psychotherapy, in three of the studies the intervention was activation oriented, and in two of the studies the intervention was chronobiological in nature. The duration of the interventions ranged from 8 days to 10 weeks. The Hamilton Rating Scale for Depression (HAM-D) (Hamilton, 1960) and/or the Beck Depression Inventory (BDI) (Beck et al., 1961) were the principal depression rating scales used to judge entry severity and outcome in the majority of the studies. Most studies had extensive exclusion criteria that varied but these included psychosis, personality disorder, substance abuse, suicidality and bipolarity. Outcome was measured either at the time of discharge from hospital, or at the end of treatment. The studies are discussed in greater detail below.
Quality appraisal
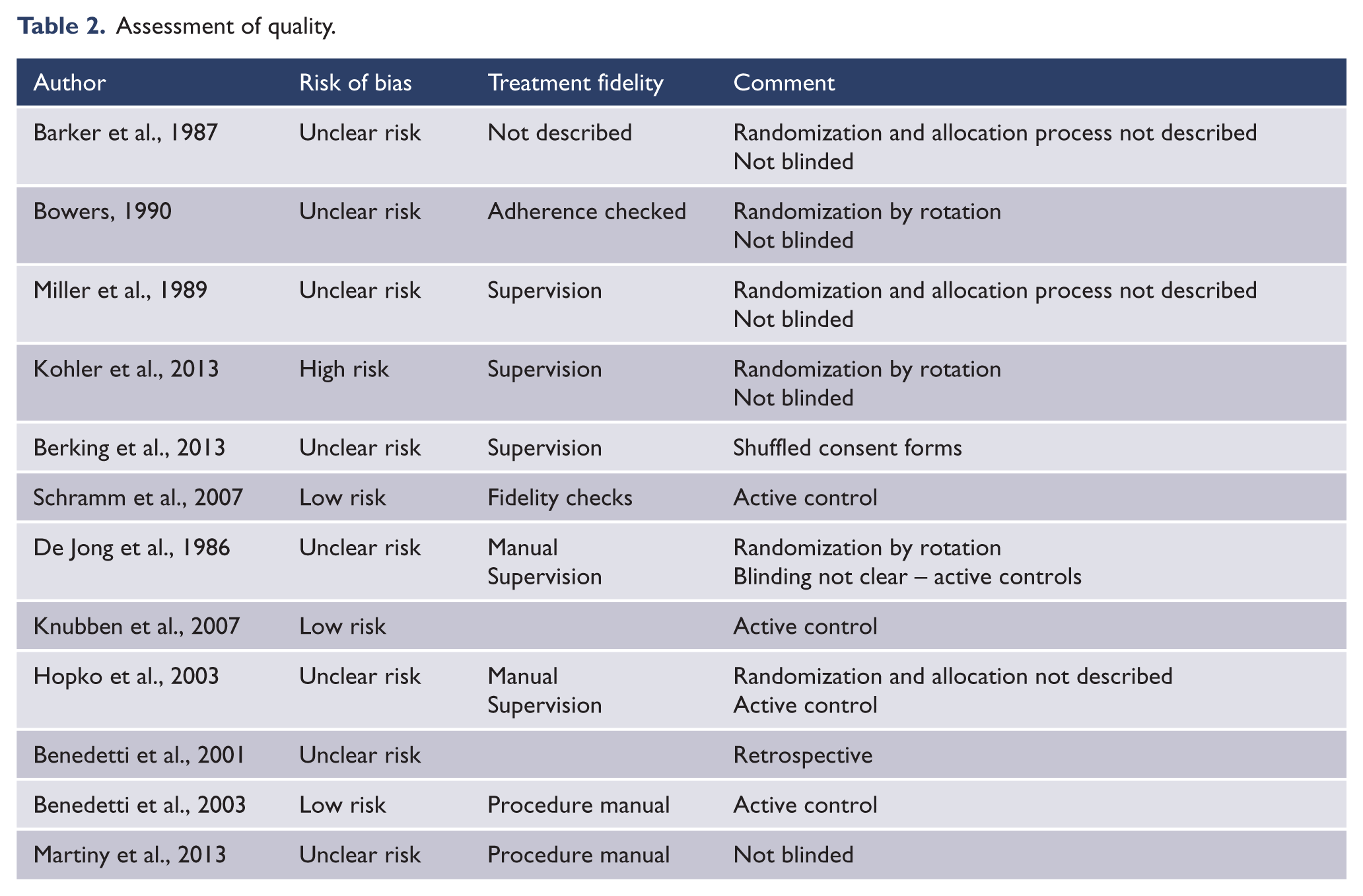
Only two studies (Knubben et al., 2007; Schramm et al., 2007) were assessed as having a low risk of bias. Most of the other studies were assessed as high or unclear risk of bias due to randomization, allocation and blinding processes (Table 2). Very few psychotherapy studies employed comprehensive fidelity checks, with most describing supervision as the only fidelity check. Only one study described comprehensive fidelity checks (Schramm et al., 2007).
Assessment of quality.
Psychotherapy trials
The majority of psychotherapy trials were conducted using CBT or a variant (n=5). The psychotherapy studies were diverse conducted over several decades in American, British, and European psychiatric hospitals. Four out of the six psychotherapy studies reported statistically significant benefits for the active psychotherapy as determined by the principal outcome measure, whereas three did not.
Cognitive behavioural therapy
Barker et al.’s (1987) trial studied 20 patients with a minimum of 2 years’ treatment-resistant depression. The patients were admitted to a specialist inpatient unit after the study group requested referrals from the local region. They received intensive pharmacotherapy with phenelzine,
In an RCT of 30 patients with unipolar major depressive disorder (MDD), Bowers et al. (1990) compared cognitive therapy (CT), relaxation therapy (RT), and a medication arm that received treatment as usual (TAU). Patients were assigned to treatment on a rotating basis and therefore clinicians in the unit would have known the next allocated treatment. A positive effect of treatment on BDI was reported with reduced scores in the CT and RT groups compared with the TAU group but this was measured using an average of scores over four time periods, including at session 1, which was higher in the TAU group – possibly creating a bias. In addition, this finding was not seen when outcome used was the HAM-D. In one of several secondary analyses, remission (HAM-D score <7) was achieved at discharge from hospital in 8/10 CT subjects, 1/10 relaxation subjects and 2/10 TAU subjects, a difference which was statistically significant. Overall, this study’s findings are limited by small group size and divergent results amongst different outcome measures.
Miller (1989) recruited 47 patients into three arms of an inpatient study: Standard Treatment, Social Skills Training plus Standard Treatment, and Cognitive Therapy plus Standard Treatment. Sessions were given daily during the inpatient phase then weekly for 20 weeks as an outpatient. The mean length of hospital stay was approximately 25 days. There were no differences between the groups in response rate or HAM-D scores at discharge from hospital. At the time of completing treatment (20 weeks after discharge), the Social Skills + Standard Treatment arm improved significantly compared with Standard Treatment. Cognitive Therapy + Standard Treatment showed a non-significant trend towards improvement over Standard Treatment. There were no significant differences between the active arms. However, the sample size of the study was probably too underpowered to show statistically significant effects between the three treatment arms.
Kohler et al. (2013) completed a relatively large study of CBT delivered in a German inpatient setting to 206 participants. Allocation to groups was not randomized as the attending psychiatrist decided whether the participant should receive CBT or clinical management (CM). All patients received pharmacotherapy and those in the CBT group received an additional two individual sessions of therapy per week. CM was not well described but appears to involve usual treatment in the inpatient setting. The results showed significant improvements in both groups, although patients who were treated with CBT in addition to medication had a greater reduction in depressive symptoms (HAM-D: 22.21 vs 19.86 and BDI: 15 vs 11.4) and higher remission rates (HAM-D: 72% vs 51% and BDI: 58.8% vs 43.1%) following treatment. Although demographic and clinical characteristics were similar between groups, the lack of random allocation to groups raises the possibility of bias and makes interpretation of these results difficult. In addition, the statistical analysis was not by intention to treat, with approximately 25% dropouts in each arm not being included in the analysis.
Berking et al. (2013) completed a German study of 432 inpatients with a mean baseline BDI score in the moderate range who were randomized to either CBT of at least one individual and four groups sessions per week, or CBT with enhanced emotion regulation training (CBT-ERT) that involved four 1.5-hour sessions and two 45-minute sessions. Medications were only used if non-pharmacological strategies appeared to be insufficient to treat depression. Patients were recruited from a routine clinical care sample and it is likely they were admitted electively for treatment of depression. Exclusion criteria were relatively broad including suicidality, psychosis and current severe alcohol or drug addiction.
CBT-ERT is a modification of CBT that incorporates mindfulness-based interventions, self-compassion training, emotion-focused therapy and problem-solving skills. The mean number of sessions that participants received was 83.56 for CBT and 83.44 for CBT-ERT. Participants in the CBT-ERT group demonstrated a significantly greater reduction in depression scores (response rates – CBT: 75.5%, CBT-ERT: 84.9%; remission rates – CBT: 51.1%, CBT-ERT: 65.1%). The paper does not identify the number of sessions patients received but they were delivered over a mean duration of 47 days. Whilst these were positive findings, the limited role of medication, the exceptionally intensive nature of treatment and the patient sample suggest these results cannot be generalized to many inpatient settings.
Interpersonal psychotherapy
Schramm et al.’s (2007) study tested the efficacy of interpersonal psychotherapy (IPT) and clinical management (CM) as adjunctive treatments to pharmacotherapy in an inpatient setting. The IPT was modified for an inpatient setting with a higher frequency of individual sessions, eight group sessions, and the inclusion of significant others in some sessions. Participants in the intervention group received 15 individual sessions of approximately 50 minutes three times a week for 5 weeks. CM involved psychoeducation and support three times per week for 20–25 minutes. Both groups received standardized pharmacotherapy. Patients were severely depressed with a HAM-D score of 25 in the IPT group compared with 22 in the CM group.
The results favoured treatment with IPT over CM, with a significant interaction between treatment and time favouring IPT on the HAM-D but not the BDI after 5 weeks. There was also a statistically significantly higher response rate of 70% for the IPT group compared with 51% with CM at 5 weeks as measured by the HAM-D. The positive findings were only found when measured by the HAM-D and not the BDI. This study also reported on longer-term outcomes after discharge from hospital. At the 3-month follow-up, in completers, IPT-treated patients continued to have a greater reduction in HAM-D. Of responders to treatment, one of 39 patients who responded in the IPT group relapsed compared with seven of 28 responders in the CM group. The difference was statistically significant.
However, this study excluded anyone with bipolar depression, antisocial or borderline personality disorder and active suicidality, suggesting that the sample was not representative of usual patients with depression on an acute inpatient ward. It was also in a German setting with a longer length of stay than some other settings (the key outcome was measured after the first 5 weeks of inpatient treatment, although length of stay for each group was not reported). An additional limitation was the difference in time provided for each intervention, with those receiving CM having approximately half the input of the IPT arm – meaning that the positive effects observed may not have been specific to IPT itself.
Behavioural activation
These studies either focused on behavioural activation or exercise interventions. De Jong et al. (1986) compared an intervention that combined behavioural activation, social competence training and cognitive restructuring with cognitive restructuring, and a control arm. The control arm was informed that an admission for treatment would be possible in about 2 months’ time. All groups were required to stop medication at least 7 days prior to starting the study. The patients in all groups met criteria for severe depression at baseline. Positive findings were found for the active treatment arms but this study is limited by the difficulty in interpreting positive effects when the control arm were withdrawn from active treatment and told that an admission may be possible at a later date, and the likelihood that patients referred for an inpatient admission who can wait 2 months do not generalize to patients utilizing most modern inpatient settings.
Knubben et al. (2007) evaluated the short-term effects of exercise on patients with major depression in a prospective randomized controlled trial. This study compared the therapeutic effects of exercise (walking) and placebo (relaxation techniques and stretching) over 10 days for inpatients with a current major depressive episode undergoing pharmacotherapy. Thirty-eight patients were randomly assigned to either exercise or placebo groups. Patients in the exercise groups walked on a treadmill daily in an interval training pattern. The placebo group carried out a 30-minute daily programme comprising of light stretches and relaxation exercises.
The exercise group had a significantly greater reduction in depression severity (measured by the Bech–Rafaelsen Melancholia Scale (BRMS), an instrument developed from the HAM-D) (Bech and Rafaelsen, 1986). After 10 days in the exercise group, depressive symptoms had decreased by 36% compared to 18% for the placebo group. A clinical response (reduction in BRMS score of 6 or more) was observed in 65% of patients in the exercise group and only 22% in the placebo group. No negative effects of the intervention were reported. This study had a number of positive attributes including a high intake of eligible participants (39/45 patients), an active comparator arm that provided similar input with respect to time, and blind raters of depression. However, the average length of admission (47 days in the exercise arm and 58 days in the control group) was longer than is typical in many settings.
Hopko et al. (2003) conducted a pilot study of brief behavioural activation treatment for depression (BATD) in an American hospital setting. This therapy is based on the premise that increased activity and resulting contact with positive consequences are sufficient to alleviate depression and increase positive thoughts and feelings. Twenty-five patients with a primary diagnosis of clinician diagnosed major depression were randomized into either the BATD (n=10) group or a supportive psychotherapy control group (n=15). All patients were treated with anti-depressant medication (tricyclic or SSRIs). The length of treatment was 2 weeks or until discharge, whichever came first. Patients in the BATD group received three 20-minute sessions per week. The initial sessions were for assessment, rapport building and introducing treatment rationale. Following these sessions, the patients were supported to make an activity hierarchy in order of easiest to most difficult that they moved through in a systematic fashion. The activity table was examined and discussed at each session to check progress and adjust goals as required. Positive progress was reinforced by the provision of tokens which could be exchanged for privileges such as off-unit passes, long-distance phone cards, snacks, or permission to participate in other community activities. Inpatients in the standard supportive psychotherapy group were also seen individually three times a week for 20 minutes, where they were encouraged to share their experiences and have non-directive discussions with a therapist. They also received tokens they could exchange for privileges but these were given in a non-contingent way and were not based on progress.
The post-treatment outcome for patients in the BATD group was a decrease in mean BDI scores from 35.1 to 19.1 that was significantly greater than the control group (37.1 to 30.2). The average length of stay for inpatients in this study was approximately 25 days, suggesting similarities with standard psychiatric units.
Chronotherapeutics
Psychiatric chronotherapeutics is the controlled exposure to environmental stimuli that act on biological rhythms in order to achieve therapeutic effects in the treatment of psychiatric conditions (Benedetti et al., 2007).
Benedetti et al. (2003) studied 30 consecutive inpatients (21 with DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) MDD and nine with DSM-IV bipolar disorder) with a current major depressive episode who were treated with 40 mg citalopram and randomized by a 3:2 ratio into either light treatment or a placebo. A lighting device was used to expose light treatment patients to 400 lux green light for 30 minutes in the morning; the placebo group was exposed to 30 minutes of a deactivated ion generated light. In order to avoid the placebo group benefitting from earlier exposure to natural light, they were treated at 07:45 instead of 06:00 as in the active group. The results found light therapy to be superior to the placebo in augmenting the antidepressant effects of citalopram. Both groups improved over the study period and there was a significant time by treatment interaction with the group receiving light therapy showing statistically significantly better scores at every time point from baseline. At 4 weeks the active group had a reduction in HAM-D of 16.3 compared with 9.5 in the placebo group.
This study followed one of the first explorations of chronotherapeutics in an inpatient setting consisting of a retrospective chart review of non-psychotic depression over a 3-year period (Benedetti et al., 2001). Patients had been assigned an east or west-facing room according to availability of space. East rooms received direct sunlight in the morning while west rooms received it in the evening. Ambient light intensity in the two conditions (avoiding direct sunlight) showed wide differences in lux. Patients with bipolar disorder who were experiencing a major depressive episode who had been located in the east rooms had a mean 3.67 days shorter duration admission than patients in west rooms. This effect was only present in summer and autumn. No effect was found in unipolar patients.
Martiny et al. (2013) conducted a wake therapy intervention in patients taking the antidepressant duloxetine; 38 patients were randomized to wake therapy and 36 patients were randomized to an exercise control group. The intervention involved wake therapy (sleep deprivation) every second night for 6 days with light therapy (daily 30-minute use of a light box at 04:00 hours) and sleep stabilization (patients were encouraged to keep a stable sleep–wake cycle and if a nap was required it was limited to no more than 30 minutes at 16:00 hours). The control group was involved in a daily exercise programme of at least 30 minutes. The acute phase treatment was followed by a 7-week continuation phase in which the intervention group had daily light therapy and sleep stabilization and the exercise group continued to have daily exercise and weekly sessions with physiotherapists. Patients in the intervention group had an immediate, large, stable and statistically significant better antidepressant effect at day 5. The response rate was diminished at day 8 but their 9-week follow-up data (Martiny et al., 2012) showed statistically significant differences between groups in response rate (wake therapy 71%, exercise control 47%) and remission rate (wake therapy 46%, exercise control 23%). Patients who had a positive diurnal variation (mood better in the evening) did better and patients who napped on days after the intervention had a poorer response. Whilst patients were admitted for the intervention, the severity of depression at baseline was moderate (HAM-D ⩾13) and the 6-day planned admission for study purposes suggests that this group of patients were not typical of patients admitted acutely for depression.
Discussion
This paper reviews studies that assessed non-pharmacological interventions for depressed inpatients. The treatments identified for inpatient depression were grouped into the following categories: psychotherapies, behavioural/ activation programmes, and chronotherapeutic interventions. The success in recruiting and retaining patients confirms that it is possible to engage moderate and severely depressed patients in structured interventions within an inpatient environment.
All studies demonstrated improvements arising from treatment in the inpatient setting. The majority of the studies also reported favourable outcomes for the intervention of interest compared to the comparator. However, there are a number of methodological issues that are useful to consider further.
Severity of inpatient population
In the studies reviewed, there were two pathways to inpatient treatment for depression: (1) it is decided that it is too unsafe to treat the patient in a community setting because of the severity of his/her symptoms; (2) the patient is admitted to an inpatient setting in order to receive treatments only available in that setting.
In the first situation, patients are often suicidal or have greater symptom severity, sometimes including psychomotor retardation, poor self-care or inadequate food and fluid intake. In many countries, this is the only situation which will result in admission. In the second situation, patients will often have relatively less severe depression and can be admitted electively. Some of the studies appraised in this review were elective admissions for treatment of depression (Barker et al., 1987; Martiny et al., 2013) or admissions to a private hospital (Miller et al., 1989), suggesting that in these patients the inpatient environment was used for therapeutic reasons and not only as a place of last resort. The remaining studies were all of usual inpatients with depression, albeit with a range of exclusion criteria.
In our own practice, depressed inpatients from a public inpatient unit had a mean Montgomery–Asberg Depression Rating Scale (Montgomery and Asberg, 1979) score of 36 (Douglas et al., 2011). Using the formula of Zimmerman (2004), this equates to a HAM-D score of 24.5. It probably also equates to a score of
Length of stay
The length of stay as inpatients differed significantly between the different study groups reviewed. This is likely to reflect more than just the severity of patients admitted for inpatient treatment of depression. For example, insurance companies may set a maximum permitted stay in private settings and while relatively milder patients are admitted, they do not stay long. Clearly, historical, cultural, and financial influences will also play a part in influencing length of stay. The average length of inpatient psychiatric stay varies greatly around the world. In the United States, the average length of stay is 6.5 days (Centre for Disease Control and Prevention, 2010), while in Germany (where four of the nine studies were conducted) it is between 36.8 and 64.3 days (Sitta et al., 2006). In the United Kingdom, the median length of stay is 15 days (Thompson et al., 2004). The mean duration of hospitalization in an Australian study was also 15 days (Zhang et al., 2011). The duration of the interventions reviewed in this article ranged from 10 days to 10 weeks. The interventions that had the longest duration were in trials in countries that have the longest average length of admission. It is unlikely that some of these interventions could be easily provided in units with shorter average lengths of stay and a more pragmatic approach to translating research into practice may be to commence the intervention in an inpatient setting and continue this on discharge to community mental health teams or primary care.
Representativeness of patient groups
Related to the issue of severity, not all patients in these trials were representative of inpatients in settings for which an admission is reserved for occasions when community care is no longer feasible. Many of the studies had extensive exclusion criteria. For example, de Jong et al. (1986) excluded patients with melancholic depression, a family history of affective disorder and episodic course.
Study findings
The psychotherapy studies had mixed results but overall provide provisional evidence that the delivery of psychotherapy to patients with both moderate and severe depression in an inpatient environment can be beneficial. However, significant limitations already discussed, such as non-random allocation to treatment and differences in the amount of input given to the comparator arm, mean that interpreting findings as specific and generalizable to the therapies reviewed is not yet possible.
Exercise treatment and behavioural activation showed positive benefits over comparators in the inpatient environment. Studies of exercise for depression in outpatient settings have shown that exercise seems to improve depressive symptoms across a range of depression severities. However, when only methodologically robust trials were included in a meta-analysis, the effect sizes were only moderate and not statistically significant (Mead et al., 2009). Given the small sample size of Knubben et al.’s (2007) study, their findings should be regarded as preliminary.
Behavioural activation also warrants further investigation as a treatment for severe depression. This intervention is based on evidence that the behavioural component may be the active mechanism of change in CBT treatments of depression (Lejeuz et al., 2001). It is also a pragmatic and simple intervention which could be cost-effective within an inpatient environment. A recent meta-analysis conducted by Cuijpers et al. (2007) concludes that it is an effective treatment for depression and that improvements are sustained at follow-up. This was supported in a subsequent meta-analysis published by Mazzucchelli et al. (2009). However, the nature of the wait-list control in De Jong’s et al.’s (1986) study suggests that caution is required before attributing specific positive effects to behavioural activation in inpatient settings.
Although the Benedetti et al. (2003) trial had a relatively small sample size, it was able to demonstrate a significant difference in antidepressant effect between those patients exposed to a 400 lux green light device and those exposed to deactivated ion generated light. The study duration of 4 weeks was closer to the more common length of stay figures and this is a treatment that could be continued after discharge. No switches to mania or hypomania were observed in the sub-group with bipolar depression, although the sub-type of bipolar disorder was not specified and a larger sample would clarify whether or not switching is a side effect of concern. Similarly, a repeat study with a larger sample would also help determine whether or not light therapy has an enduring role in the treatment of major depression.
Research implications
The studies show that it is possible to provide and study non-pharmacological interventions for depression on an inpatient ward. Whilst many findings should be regarded as preliminary, they are also supportive of further research and interest in this area. We suggest that future studies of inpatient interventions for the treatment of moderate to severe depression need to provide a flexible model of delivery that can cross between inpatient and outpatient services. This approach seeks to avoid artificial constraints on length of stay as an inpatient for the purposes of treatment completion and better suits settings where a long stay is not an option.
In addition to demonstrating clinical efficacy, we also propose that future studies utilize a methodology that incorporates the features of clinical effectiveness studies proposed by Bauer and colleagues (2001). They identified key principles for the design of an effectiveness study to ensure external and internal validity which were:
The sample should reflect the target population to which the results will be generalized. Exclusion criteria should be limited and the intervention should be delivered in the inpatient setting.
The intervention should be widely implementable in the target practice venues, with careful attention to feasibility in terms of resources, system characteristics and staff training. Fidelity checking needs to be included in psychotherapy description.
The research data collection load should be as low and as flexible as possible and data collection procedures should not be linked to clinical interventions.
Data analysis procedures should account for data not missing at random and take into account sample heterogeneity: Because of the nature of clinical effectiveness trials (i.e. not tightly controlled under experimental conditions), it is likely that there will be missing data; however, every effort will be made to evaluate this to ensure bias is not occurring.
Conclusion
Psychiatric inpatient units should not just be regarded as places of containment where the administration of medication occurs. Improving the care that inpatient settings provide has the potential to improve the experiences of patients who use psychiatric inpatient services, improve patient outcomes, and prevent relapse.
A diverse range of treatment strategies have been identified in this review including therapy, behavioural activation, and chronotherapeutic interventions. These studies provide evidence that non-pharmacological treatments for depression can be given to enhance outcomes and that research can be undertaken in inpatient settings. Given the restrictions on inpatient admissions it may also be worthwhile trialling these interventions for patients with moderate to severe depression in outpatient settings. Whilst the evidence base has limitations, this review also highlights therapeutic and research opportunities in this area.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.