
Abstract
Objective:
To examine the uptake, population reach and outcomes of primary mental healthcare services provided to Indigenous Australians via the Access to Allied Psychological Services (ATAPS) program between 2003 and 2013, with particular reference to enhanced Indigenous ATAPS services introduced from 2010.
Method:
Utilising ATAPS program data from a national minimum data set and comparative population data, we conducted descriptive analyses, regression analyses and t-tests to examine the uptake of ATAPS services, provider agency level predictors of service reach, and preliminary outcome data on consumer level outcomes.
Results:
Between 2003 and 2013, 15,450 Indigenous client referrals were made that resulted in 55,134 ATAPS sessions. National Indigenous service volume more than doubled between 2010 and 2012, following the introduction of enhanced Indigenous ATAPS services. Non-Indigenous ATAPS service volume of primary care agencies was uniquely predictive of Indigenous service reach. Preliminary analysis of limited consumer outcome data indicated positive treatment gains and the need to enhance future outcome data collection.
Conclusions:
Concerted national efforts to enhance mainstream primary mental healthcare programs can result in significant gains in access to mental healthcare for Indigenous populations.
Introduction
The mental health of Indigenous Australians
According to the 2011 Australian census, there were 548,370 Indigenous people living in Australia, comprising around 2.5% of the total population (Australian Bureau of Statistics, 2012a). Of these, 90% were of Aboriginal origin, 6% were of Torres Strait Islander origin and 4% of both Aboriginal and Torres Strait Islander origin. Indigenous Australians, who are on average younger than non-Indigenous Australians (with a median age of 21 vs 37 years), have been found to have a significantly lower life expectancy and to face proportionally greater challenges and disadvantage in terms of a variety of socio-economic, health and mental health related indicators than non-Indigenous Australians (Australian Bureau of Statistics, 2010; Vos et al., 2009; Anderson et al., 2006).
In 2008, a national survey indicated that nearly one-third (31%) of Indigenous Australians aged 15 years and over had experienced high to very high levels of psychological distress, representing more than twice the rate for non-Indigenous people (Australian Bureau of Statistics, 2010). Suicide is a significant issue within Indigenous communities, with a least 996 Indigenous suicide deaths registered in Australia between 2001 and 2010. In 2010, suicide accounted for 4.2% of registered deaths for Indigenous Australians, compared with only 1.6% for all Australians (Australian Bureau of Statistics, 2011). Indigenous suicide rates have been found to be significantly elevated among young people (aged 15 to 19 years) and to be highest overall for young Indigenous males aged 25 to 29 years (Australian Bureau of Statistics, 2012b). Suicide rates for male and female Indigenous Australians in 2011 were 2.5 and 3.4 times higher than for respective non-Indigenous cohorts. Moreover, in 2011 suicide ranked as the fourth and 15th leading cause of death for Indigenous Australians and all Australians, respectively (Australian Bureau of Statistics, 2013).
The comparatively high rates of psychological distress and suicide encountered among Indigenous Australians have been attributed to a complex set of factors which not only include disadvantage and risk factors shared by non-Indigenous Australians, but also a broader set of social, economic and historic determinations that impact on Indigenous social and emotional wellbeing (Australian Government Department of Health and Ageing, 2013), including racism (Priest et al., 2011). Efforts to address existing health disparities and improve mental health outcomes of Indigenous Australians have therefore increasingly recognised the need to reflect broader determinants of Indigenous health that are commonly encapsulated within a framework of social and emotional wellbeing (Holland et al., 2013; Social Health Reference Group, 2004). This framework recognises the important place of culture, spirituality, connections to family, kin and land as foundations of Indigenous health. Moreover, the need for access to culturally appropriate health services was highlighted in both the Fourth National Mental Health Plan 2009-2014 (Australian Health Ministers’ Conference, 2009) and the National Strategic Framework for Aboriginal and Torres Strait Islander Health 2003-2013 (Australian Government Department of Health and Ageing, 2007) as vital to improving Indigenous health outcomes.
Primary care based mental healthcare
Primary healthcare agencies and providers such as Aboriginal community controlled health services (ACCHS) and family physicians (known in Australia as general practitioners, or GPs) play key roles in advancing Indigenous mental health by facilitating access to appropriate mental healthcare. Nevertheless, Indigenous Australians have been found to have overall lesser access to GPs (Holland et al., 2013; Bywood et al., 2011) and to consult GPs more frequently for mental health problems than non-Indigenous Australians (Australian Institute of Health and Welfare, 2012). The task of improving access to culturally appropriate primary mental healthcare for Indigenous Australians has therefore been recognised as a key priority for mental health policy.
The Access to Allied Psychological Services program
As a pillar of the Australian primary mental healthcare system, the Access to Allied Psychological Services (ATAPS) program was introduced by the Australian Government in 2001 in response to low treatment rates for common mental disorders in the general population. The program was originally implemented through regional fundholding primary care agencies, known as Divisions of General Practice (‘Divisions’), which transitioned to 61 Medicare Locals in three consecutive funding rounds or ‘tranches’ in 2011-12 (i.e., in July 2011, January 2012, and July 2012). The ATAPS program supports GPs and mental health professionals to provide optimal primary mental healthcare. More specifically, ATAPS enables GPs and other eligible referrers to refer consumers with high prevalence disorders (e.g., depression and anxiety) to mental health professionals for up to 12 individual sessions (or 18 in exceptional circumstances) and/or 12 additional group sessions of evidence-based mental healthcare (predominantly cognitive behavioural therapy (CBT)). Review by the referring GP is essential after each block of six sessions and/or the final session (Hickie and Groom, 2002).
From 2008, several ATAPS initiatives were introduced that focussed on particular hard-to-reach or at-risk populations (e.g., women with perinatal depression, people at risk of suicide or self-harm, children with mental disorders, people in rural and remote locations, people experiencing or at risk of homelessness) and/or which trialled new modalities of service delivery, such as telephone- or web-based CBT (Reifels et al., 2013). These so-called ATAPS Tier 2 initiatives aimed to enhance service capacity and flexibility to address the needs of specific target groups. The original ATAPS arrangements are now called the Tier 1 ATAPS initiative.
Enhanced Indigenous ATAPS services
As part of a mental health reform package, ATAPS funding was significantly increased in the 2011-12 Federal Budget (by AU$36.5 million over five years) to expand and enhance ATAPS mental health and suicide prevention services with a view to supporting an additional 18,000 Indigenous Australians. As a result, two dedicated Tier 2 ATAPS initiatives specifically aimed at Indigenous Australians were introduced (hereafter referred to as enhanced ‘Indigenous ATAPS services’). These included the Indigenous mental health service from July 2010 and the Indigenous suicide prevention service from July 2011. Both services incorporated specific enhancements and flexibilities to improve equitable access to and cultural appropriateness of ATAPS services for Indigenous Australians (Australian Government Department of Health and Ageing, 2012a; Australian Government Department of Health and Ageing, 2012b; Reifels et al., 2014).
Service establishment by administering primary care agencies involved: development of formal linkages and referral pathways with stakeholders in Indigenous mental health (e.g., Indigenous health organisations; ACCHS; emergency departments); up-skilling of mental health professionals (e.g., cultural competency, or suicide prevention training); establishment of supervision, support and clinical governance arrangements; and service promotion. Non-Indigenous providers and administrators complete mandatory Indigenous cultural competency training, and full professional registration and completion of suicide prevention training are mandatory for suicide prevention service providers.
The Indigenous mental health service aims to provide Indigenous Australians with an ‘increased level of access to evidence based short-term focussed psychological strategies services that are culturally appropriate, within a primary care setting’ (Australian Government Department of Health and Ageing, 2012a). The service is targeted at Indigenous people who have, or are at risk of developing, a mild to moderate mental disorder (most commonly, anxiety and depression). Indigenous clients can be referred by their GP or psychiatrist, or via provisional referral from an ATAPS mental health professional, an Indigenous health organisation, ACCHS, or a paediatrician. Where provisional referrals are made, consumers must have a mental health treatment plan prepared in consultation with a GP or psychiatrist preferably within two weeks of the first session, or as soon as practical where GP access is not readily available. The applicable session limit and intervention types are largely consistent with the broader ATAPS program. Interventions are tailored to the needs and cultural requirements of Indigenous clients, including through provision of therapy involving the whole family, as required. The Indigenous mental health service became a mandatory ATAPS initiative for all Medicare Locals in July 2012.
The Indigenous suicide prevention service is designed to provide priority access to ATAPS for Indigenous Australians who have attempted or are at moderate risk of suicide, family members and friends of people who have died by suicide and who are at risk themselves, and other Indigenous people with mental health problems at risk of suicide or self-harm (Australian Government Department of Health and Ageing, 2012b). This includes Indigenous people who have: been discharged from a hospital or emergency department into the care of GPs or ACCHS; presented to GPs or ACCHS after an incident of self-harm; or expressed strong suicidal ideation to their GP, ACCHS, community Elders, or drug and alcohol service. The service is not intended for people at acute risk of suicide or self-harm, or those experiencing recurrent thoughts of self-harm, who are more appropriately treated by state and territory mental health services. Consumers can be referred through their GP or via provisional referral from an emergency department, hospital ward, acute mental health team, Indigenous health organisation, ACCHS, paediatrician, ATAPS mental health professional, or drug and alcohol service. An unlimited number of sessions can be provided over the course of three months, and a diagnosis and GP mental health treatment plan are not required at referral. The mental health professional is required to make client contact within 24 hours and provide the first session within 72 hours of referral, or earlier as required. Interventions are consistent with the broader ATAPS program, tailored to the needs of Indigenous clients, and include focussed psychological strategies, narrative therapy, proactive case management, client follow up support, and GP- or ACCHS-led care coordination. Additional client support is available through an ATAPS After Hours Suicide Support Line and referral to other appropriate services. The service is not currently considered mandatory for Medicare Locals.
This study is the first to examine the uptake and outcomes of enhanced Indigenous ATAPS services specifically, the uptake of ATAPS services provided to Indigenous clients between 2003 and 2013 more generally, and key factors underpinning Medicare Local service reach to Indigenous Australians. As such, this research makes a vital contribution to addressing a gap in the broader debate about evidence-based mental health services reform in Australia (Jorm and Malhi, 2013).
Method
Data sources
Minimum dataset
Data for Indigenous ATAPS services and mental health care provided to Indigenous Australians via other ATAPS initiatives were derived from a purpose-designed, national, web-based minimum dataset. The minimum dataset captures de-identified, consumer- and session-level information, including pre- and post-treatment scores on standardised outcome measures, which are routinely entered by local users (i.e., Medicare Local staff, ATAPS providers). Data for the period from 1 July 2003 to 30 June 2013 were downloaded on 28 October 2013.
Medical Local-level population data
The Australian Government Department of Health provided us with 2012 Australian Bureau of Statistics Estimated Resident Populations for each Medicare Local (including total and Indigenous populations), based on 2011 Australian Census data. The data were disaggregated by the Socio-Economic Indexes for Areas (SEIFA), the Index for Relative Socio-Economic Disadvantage (IRSED, in quintiles) and the Australian Standard Geographical Classification Remoteness Area (ASGC-RA) classifications (major cities, inner regional, outer regional, remote and very remote), also derived from the 2011 census data. Together with the ‘tranche’ (or funding round) of each Medicare Local, these data were used to explore factors contributing to levels of service delivery by Medicare Locals.
Data analyses
Descriptive analysis
Using SPSS v21, simple frequencies and percentages were calculated from data in the minimum dataset to report on: trends in the uptake of Indigenous ATAPS services and uptake of other ATAPS initiatives by Indigenous consumers; demographic and clinical characteristics of Indigenous ATAPS services consumers; and the types of services delivered.
Regression analysis
A standard multiple regression analysis was performed in SPSS v21 to explore factors associated with differential service reach to Indigenous clients by Medicare Locals via the entire suite of ATAPS initiatives. More specifically, the regression examined the relationship between the rate of unique Indigenous clients referred to any ATAPS initiative as a proportion of the total Indigenous population in each Medicare Local area (dependent variable) and each of the following independent (predictor) variables at a Medicare Local-level: the proportion of Indigenous people in the population in the two most disadvantaged quintiles; the proportion of Indigenous people residing in outer regional, remote and very remote locations; the rate of non-Indigenous client referrals to ATAPS; and the tranche in which each Medicare Local was funded to replace Divisions (i.e., tranche one - July 2011, tranche two - January 2012, tranche three - July 2012).
Paired t-tests
Outcomes for consumers of Indigenous ATAPS services were analysed using paired t-tests to examine the difference between mean pre- and post-treatment scores on consumer outcome measures. Consumers who did not have a ‘matched pair’ of pre- and post-treatment scores were excluded. As were outcome measures for which there were fewer than 30 observations and those for which pre- and post-treatment scores were ‘zero’. It was assumed that where pre- and post- treatment scores were ‘zero’ that the outcome measure was not actually administered and that matched pre- and post-treatment scores in the absence of recorded sessions were invalid. Due to the limited scope of available outcome data, existing data for both Indigenous ATAPS services were combined for the purpose of analysis.
Results
Service uptake
Service provider involvement
Fifty-eight of 61 existing Medicare Locals were involved in the Indigenous mental health service and 16 Medicare Locals were involved in the Indigenous suicide prevention service during the 2011-12 and 2012-13 financial years. The vast majority of 1,484 unique referrers involved in Indigenous ATAPS services were GPs (96.2% overall). In the 2012-13 financial year, the referrer profile diversified slightly with increasing involvement of those new referrer types that were only recently enabled on the minimum dataset in May 2013. These included Indigenous health organisations and ACCHS (1.2%), NGOs (1.1%), and mental health professionals (0.8%). A total of 713 unique mental health professionals had delivered Indigenous ATAPS services during the analysis period.
Referrals
Figure 1 shows the number and proportion of Indigenous client referrals made to enhanced Indigenous ATAPS services and all other ATAPS initiatives between July 2003 and June 2013, by financial year. In total, 15,450 Indigenous client referrals were made through ATAPS during the analysis period. Indigenous client referral numbers showed large increases each financial year, rising from 219 referrals in 2003-4 to 4,758 referrals in 2012-13. The financial years 2011-12 and 2012-13 saw the largest increases in Indigenous client referrals from previous years with 756 and 2,039 additional referrals, respectively. Simultaneously, the proportion of Indigenous client referrals of all ATAPS referrals (3.9% overall, not shown), rose steadily from 2.2% in 2003-4 to 6.8% in 2012-13.
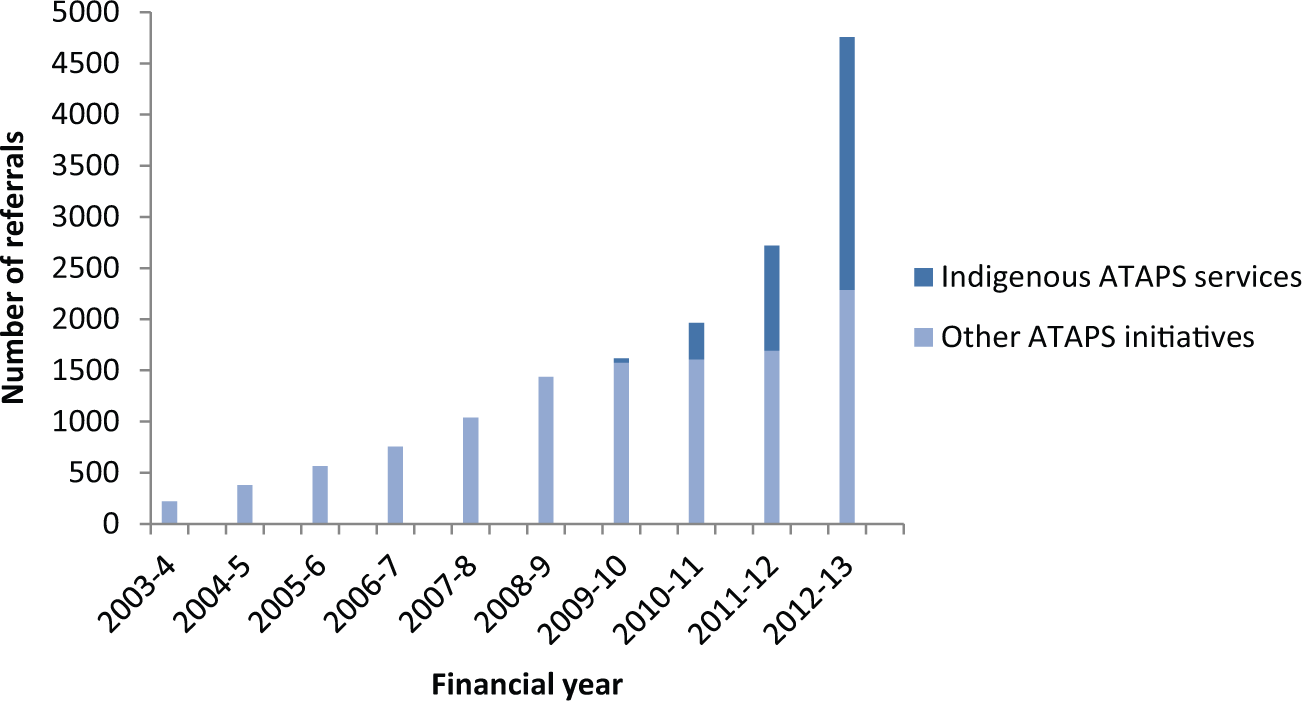
Number of Indigenous client referrals made via ATAPS initiatives (July 2003 to June 2013), by financial year.
Overall, the general Tier 1 ATAPS initiative (9,876, 63.9%) accounted for the majority of Indigenous client referrals to ATAPS. However, since their introduction, Indigenous ATAPS services accounted for a rapidly increasing proportion of Indigenous client referrals to ATAPS (25.2% overall), rising from 18.0% in 2010-11 to 52.0% in 2012-13. In other words, as of the most recent financial year, more than half of all Indigenous client referrals to ATAPS are now being made via Indigenous ATAPS services. The vast majority of these referrals were made through the Indigenous mental health service (3,827, 98.3%) and only a small proportion through the Indigenous suicide prevention service (68, 1.7%). Other ATAPS initiatives attracting Indigenous client referrals included the suicide prevention (491, 3.2%), child (431, 2.8%), perinatal depression (376, 2.4%), homelessness (185, 1.2%) and rural and remote (156, 1.0%) initiatives.
Sessions
In total, 3,057 (79.9%) Indigenous mental health service referrals and 55 (80.9%) Indigenous suicide prevention service referrals resulted in one or more sessions with a mental health professional, compared to 78.9% for all ATAPS referrals. Consistent with the referral pattern, the vast majority of Indigenous ATAPS services sessions were delivered through the Indigenous mental health service (13,197, 98.6%) and 194 (1.4%) sessions through the Indigenous suicide prevention service. The rapidly increasing proportion of Indigenous ATAPS services sessions accounted for 53.0% of all Indigenous client sessions delivered via ATAPS in 2012-13. Referrals to the Indigenous mental health and Indigenous suicide prevention services resulted in a mean of 4.6 and 4.4 sessions per consumer, respectively, compared to an average of 5.2 sessions for all ATAPS consumers. A total of 55,134 Indigenous client sessions were delivered via ATAPS during the analysis period.
Demographic and clinical consumer profile
Table 1 shows that the majority of Indigenous ATAPS services consumers were female (63.7%), Indigenous Australians (83.8% Aboriginal, 10% Torres Strait Islanders) with a mean age of 34.2 years (SD 15.3). About three quarters (73.5%) were on a low income, eighty percent spoke English at home (79.6%), and about two-thirds (67.4%) were rated as understanding English either well or very well. Consumers of Indigenous ATAPS services were predominantly based in major Australian cities (45.3%) followed by regional Australia (41.3%), then remote and very remote Australia (5.8%). The clinical consumer profile shown in Table 2 indicates that one-third (34.0%) of Indigenous ATAPS services consumers had a history of previous psychiatric care and that the majority were diagnosed with depression (57.5%), and/or anxiety disorders (40.1%), followed by alcohol and drug use disorders (11.0%), and psychotic disorders (1.7%).
Demographic consumer profile of enhanced Indigenous ATAPS services.
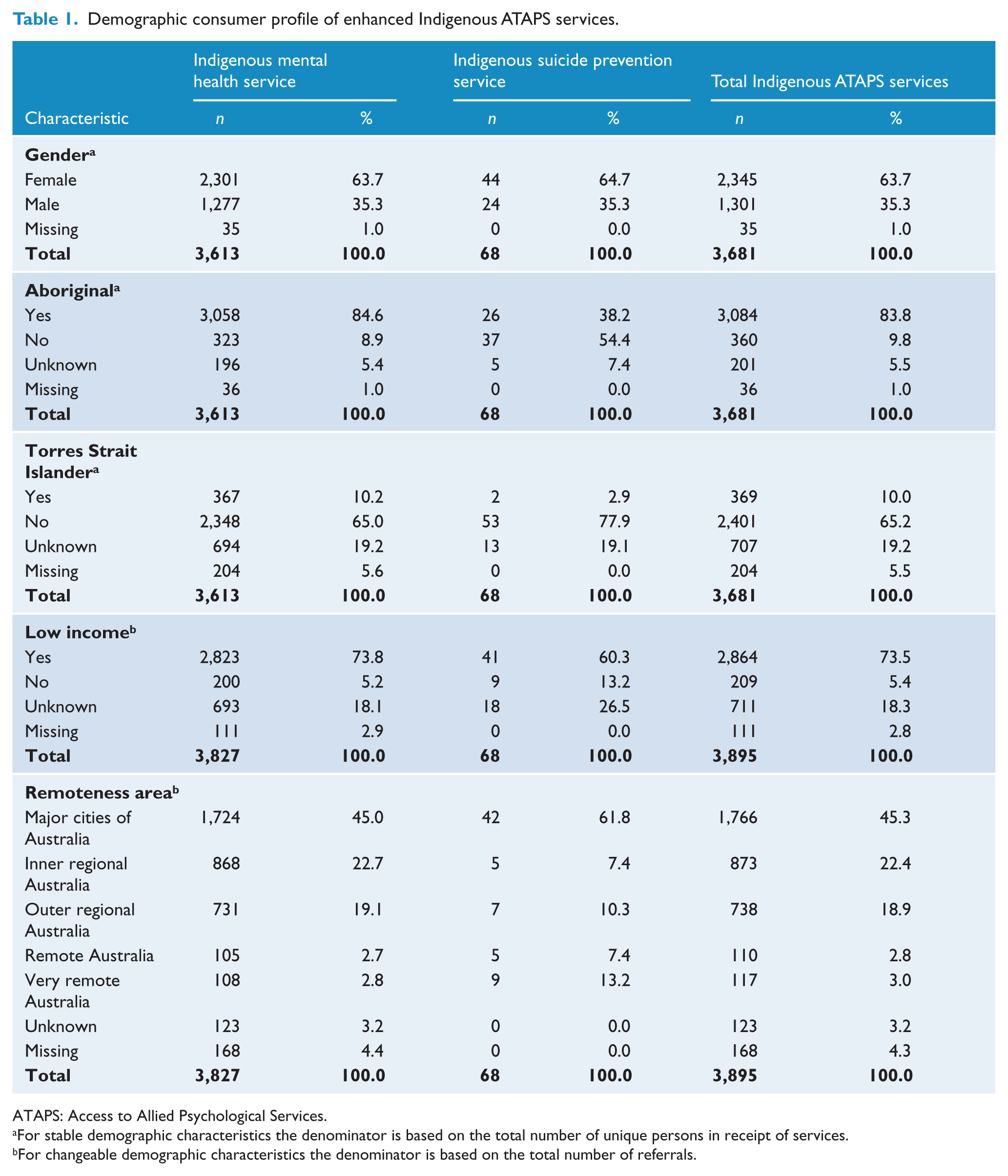
ATAPS: Access to Allied Psychological Services.
For stable demographic characteristics the denominator is based on the total number of unique persons in receipt of services.
For changeable demographic characteristics the denominator is based on the total number of referrals.
Clinical consumer profile of enhanced Indigenous ATAPS services and interventions delivered.
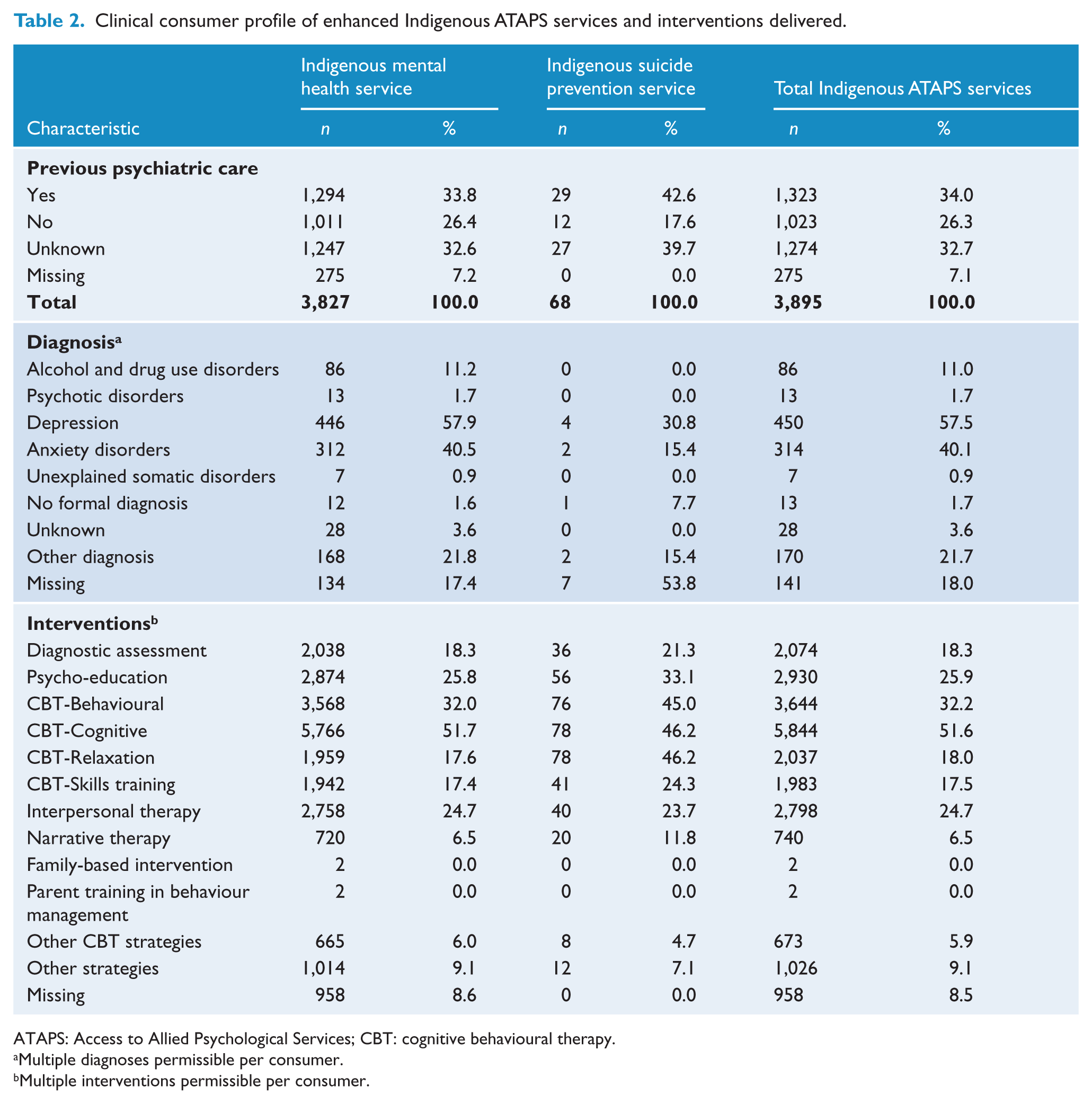
ATAPS: Access to Allied Psychological Services; CBT: cognitive behavioural therapy.
Multiple diagnoses permissible per consumer.
Multiple interventions permissible per consumer.
Treatment characteristics
The majority of Indigenous ATAPS services consumers participated in individual sessions (91.8%) that were face to face (88.8%) and of between 46 and 60 minutes duration (84.6%). Group sessions comprised 7.2% of Indigenous ATAPS services sessions delivered (compared with 1.3% for all ATAPS sessions in 2012-13). The most common interventions delivered were CBT-cognitive (51.6%) and CBT-behavioural (32.2%) interventions, followed by psycho-education (25.9%) and interpersonal therapy (24.7%). Only 1.4% of Indigenous mental health service consumers and none of the Indigenous suicide prevention service consumers were charged a co-payment. The rate of unattended Indigenous ATAPS services sessions was 15.5%.
Consumer outcomes
In total, only 109 (3.5% of) Indigenous ATAPS services consumers had pre- and post-treatment outcome scores available on the minimum dataset for outcome measures with at least 30 matched pre- and post-treatment scores. Over two-thirds of these had been assessed using the Depression Anxiety and Stress Scales (DASS)-Anxiety (69.7%), DASS-Depression (69.7%) or DASS-Stress (68.9%) scale (Lovibond and Lovibond, 1995). The Kessler-10 (K-10) was used with 33.9% of consumers (Kessler et al., 2002).
Table 3 shows mean pre- and post-treatment scores and mean differences for Indigenous ATAPS services consumers with available outcome data. A positive difference for measures is indicative of symptom improvement. Mean pre- to post-treatment differences on all measures were statistically significant (p < .001) and indicative of clinical improvement. Mean differences in DASS-Anxiety scores were equivalent to a shift in symptom severity from the ‘extremely severe’ to the ‘severe’ range. Mean symptom reductions on the DASS-Depression scale indicated a shift from the ‘severe’ to ‘moderate’ range. Mean DASS-Stress scores improved from the ‘moderate’ to ‘mild’ symptom range. Mean K-10 scores indicated a reduction from ‘very high’ to ‘high’ levels of distress. However, due to the very small proportion of Indigenous consumers with available outcome data, these preliminary findings should be interpreted with considerable caution.
Mean pre- and post-treatment consumer outcome scores and differences for enhanced Indigenous ATAPS services.
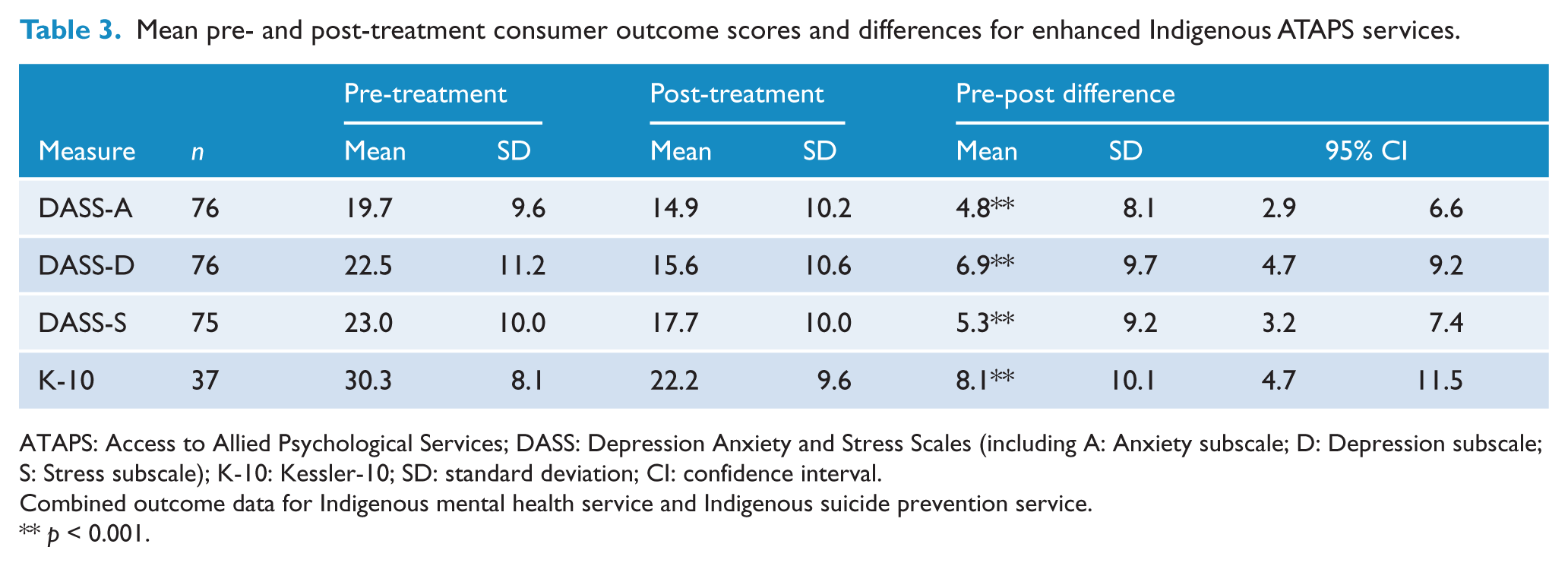
ATAPS: Access to Allied Psychological Services; DASS: Depression Anxiety and Stress Scales (including A: Anxiety subscale; D: Depression subscale; S: Stress subscale); K-10: Kessler-10; SD: standard deviation; CI: confidence interval.
Combined outcome data for Indigenous mental health service and Indigenous suicide prevention service.
p < 0.001.
Predictors of Medicare Local service reach to Indigenous Australians
The regression analysis examined the association between the rate of unique Indigenous people referred to the entire suite of ATAPS initiatives as a proportion of the population of Indigenous people in each Medicare Local (dependent variable) and each of the following potential predictors at a Medicare Local level (independent variables): the proportion of Indigenous people in the two most disadvantaged quintiles; the proportion of Indigenous people residing in outer regional, remote and very remote locations; the rate of referrals for non-Indigenous people (per 100 non-Indigenous people in the population) to ATAPS; and the tranche in which each Medicare Local was funded to replace Divisions. Table 4 displays the correlations between the independent variables and the rate of unique Indigenous people referred to ATAPS as a proportion of the population of Indigenous people in each Medicare Local (dependent variable) and the standardised regression coefficients (β) for the independent variables.
Simple correlations between predictor variables and rate of Indigenous people referred to ATAPS, and standard regression coefficients (β).
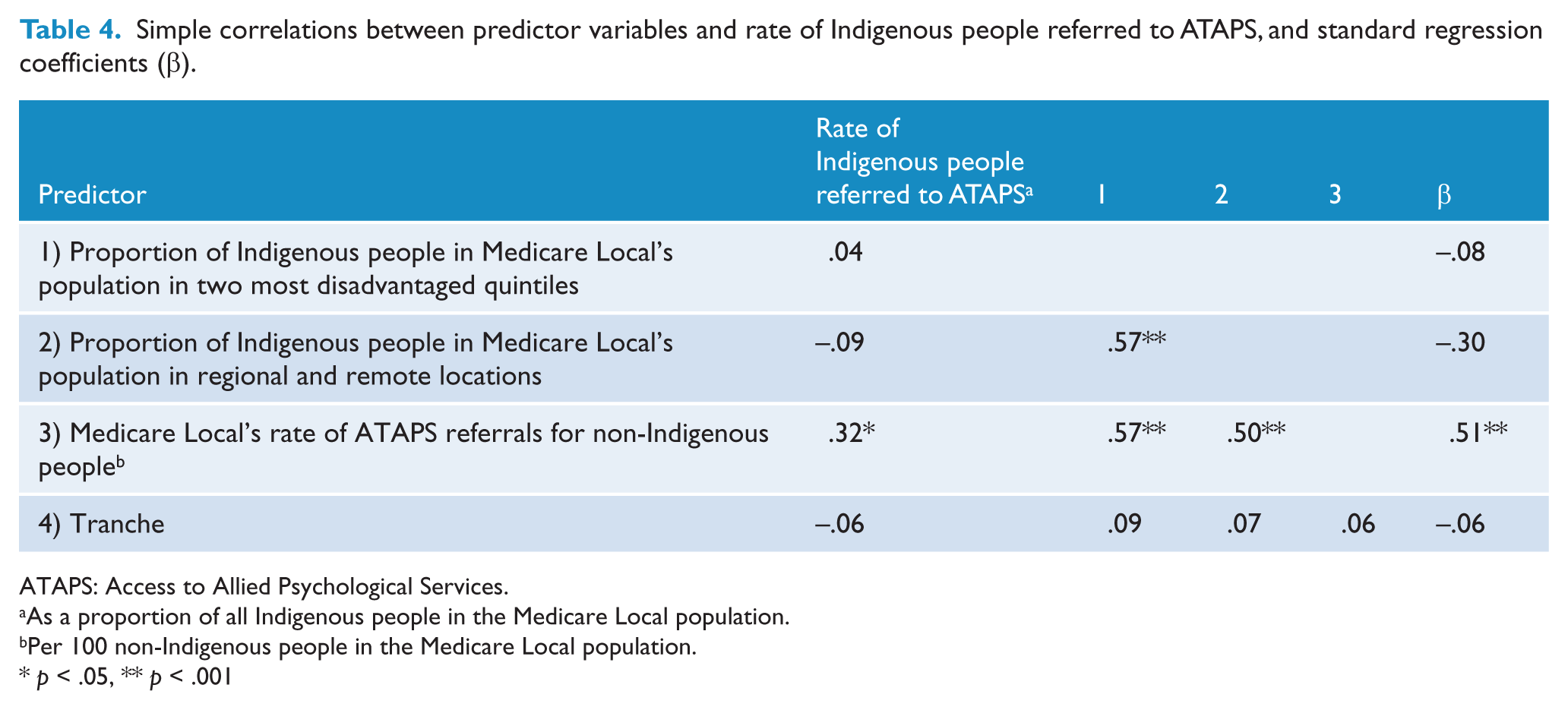
ATAPS: Access to Allied Psychological Services.
As a proportion of all Indigenous people in the Medicare Local population.
Per 100 non-Indigenous people in the Medicare Local population.
p < .05, ** p < .001
As shown in Table 4, at a Medicare Local level there was a significant positive relationship between the rate of Indigenous people referred to ATAPS (as a proportion of Indigenous people in the population) and the rate of referrals for non-Indigenous people, although the magnitude of this association was low to moderate. In other words, referral of Indigenous people to ATAPS was moderately higher in Medicare Locals with a higher rate of referrals for non-Indigenous people. There were relatively stronger positive associations between disadvantage and each of remoteness and rate of referrals for non-Indigenous people, and between remoteness and rate of referrals for non-Indigenous people.
The combination of all four predictor variables in the regression model accounted for a significant percentage of variance (19%) in the rate of Indigenous people referred to ATAPS, R = .44, F(4,56) = 3.30, p = .017. However, only the rate of referrals for non-Indigenous people made a significant independent contribution to the prediction of the rate of referral of Indigenous people to ATAPS. These findings indicate that the rate of Indigenous people referred to ATAPS is associated with the rate of referrals for non-Indigenous people; for every standard deviation increase in the rate of referrals for non-Indigenous people in a Medicare Local, the referral rate for Indigenous people increases by 0.51 standard deviations. However, remoteness was also close to reaching statistical significance (p = 0.054) as a predictor, thus suggesting that in practice, the greater the proportion of Indigenous people in outer regional and remote locations, the lower the proportion of Indigenous people referred to ATAPS.
Discussion
This study demonstrates that the introduction of enhanced Indigenous ATAPS services accounted for substantial increases in the number ATAPS services provided to Indigenous Australians. Between 2010-11 and 2012-13, the overall Indigenous service volume more than doubled, while the volume of enhanced Indigenous ATAPS services increased eight-fold. The fact that Indigenous people accounted for 6.8% of all ATAPS referrals in 2012-13 (compared to 2.5% in the total population) is encouraging in view of the greater mental health burden experienced by Indigenous Australians (Vos et al., 2009; Whiteford et al., 2013).
Nationally, the increased access of Indigenous Australians to ATAPS was primarily driven by growth in the Indigenous mental health service; uptake of the Indigenous suicide prevention service remained limited. Potential reasons for lesser uptake of the latter initiative include its non-mandatory nature, its later introduction, and limited primary care agency awareness of the service. Simultaneously, the pre-existing general ATAPS suicide prevention initiative, which is mandatory for all Medicare Locals, also accommodated a growing number of Indigenous clients, as indicated by a 3.4 fold increase in Indigenous client referrals between 2010-11 and 2012-13.
Rapid early Indigenous ATAPS services growth was achieved without utilisation of the full range of flexibilities afforded to the two initiatives. Overall referral patterns were predominantly reliant on GP referrals and marked by recent diversification. The treatment profile of Indigenous ATAPS services was similar to that of the broader ATAPS program in 2012-13 in terms of the most common interventions and session formats utilised (Bassilios et al., 2013). Notable exceptions included the greater use by Indigenous ATAPS services of narrative therapy interventions (6.5% vs 2.4%) and group session formats (7.2% vs 1.3%), with the latter the highest rate of all ATAPS initiatives. Consistent with the broader ATAPS program, most commonly assigned consumer diagnoses were depression, anxiety, and alcohol and drug use disorders, with the latter more prevalent among Indigenous than non-Indigenous ATAPS consumers (11.0% vs 5.3%).
Compared to national Indigenous population statistics, the distribution of Indigenous ATAPS services consumers indicated good Indigenous service coverage for regional Australia (41.3% vs 43.0%), some overrepresentation of major cities (45.3% vs 32.0%) and some underrepresentation of remote and very remote locations (5.8% vs 14.0%) (Australian Bureau of Statistics, 2010). Remoteness as a near significant predictor of Medicare Local service reach further underpins the persistent challenge of Indigenous service coverage in geographically vast countries like Australia (De Coteau et al., 2006; Hunter, 2007). A potential explanation of non-Indigenous service volume as a predictor of Indigenous service reach may be that agencies with overall greater service volume have developed more efficient service systems, partnerships, and processes for targeting services to the local population, including to relevant subgroups.
ATAPS service uptake findings need to be viewed in the broader context of Indigenous access to other government-funded primary mental healthcare services, such as the much larger Better Access program, which provides similar services funded through Medicare (Bassilios et al., 2010). Despite the lack of direct comparison data on Indigenous Better Access use, the vastly greater service volume of this program, illustrated by 1,130,384 Better Access recipients in 2009 alone (Harris et al., 2010) compared to 277,307 ATAPS referrals with resulting sessions between 2003 and 2012 (Bassilios et al., 2013), suggests that an overall much larger number (albeit probably a relatively smaller proportion) of Indigenous Australians receive mental healthcare through Better Access. Indigenous Australians have been found to have overall lesser access to primary healthcare and certain Medicare services (Kehoe and Lovett, 2008), as indicated by Medicare expenditure of less than half the non-Indigenous average (Deeble et al., 2008). Recent findings from the BEACH survey, which monitors Australian general practice activity, indicate that Indigenous people accounted for 2.2% of mental health related general practice encounters in 2010-11 (Australian Institute of Health and Welfare, 2012). Thus, despite evident gains in the access to ATAPS, it is likely that we may still have a fair way to go in terms of improving Indigenous access to primary mental healthcare in Australia more generally.
While preliminary outcome data analysis on the basis of limited outcome data indicated positive treatment gains, relatively high mean post-scores on some outcome measures indicate further scope for clinical improvement and/or sessions with a mental health professional. In this context, it is noteworthy that Indigenous ATAPS services consumers had slightly elevated mean pre-treatment DASS-Anxiety scores compared to Tier 1 ATAPS consumers (19.7 vs 16.3). Furthermore, a doubling in the rate of unattended sessions for Indigenous versus non-Indigenous clients (15.5% vs 7.1%) poses a particular challenge for effective mental healthcare that is not necessarily confined or unique to the ATAPS program.
The study findings should be interpreted in light of several important limitations. Firstly, it is possible that the limited scope of consumer outcome data introduced a systematic bias, such that consumers without available outcome data may have had poorer outcomes (if, for instance, outcome data were unavailable because they dropped out of treatment). Additional analyses indicated some differences in the profile of consumers with and without available outcome data. The former were more likely than the latter to be older (38.7 vs 34.0 years), male (38.5% vs 35.4%), living in major cities (58.7% vs 45.0%), diagnosed with depression (74.1% vs 54.3%), anxiety (62.0 vs 39.0%) and alcohol and drug use (22.2% vs 11.4%) disorders, and to have received more sessions per referral (mean 7.0 vs 4.5). These differences therefore limit the representativeness of the sample with outcome data and the generalizability of preliminary outcome data findings. Our findings further highlight the importance of future efforts to enhance outcome data collection in regard to Indigenous ATAPS services.
Secondly, the population denominators used in this study did not take into account the proportion of those in the population with mental health problems, or whether those in need of care were the ones receiving treatment. Similarly, this study did not examine the impact of other locally existing Indigenous health services on ATAPS service reach, or the merit and acceptability of specific implementation and cultural adaptation mechanisms employed by agencies and providers (Chowdhary et al., 2014).
Thirdly, the fidelity of psychological interventions (e.g., whether practitioners actually provide the CBT-based strategies they say they do in practice) was not examined (Allen and Jackson, 2011). Finally, the extent of the common problem of non-identification of Indigenous people in healthcare services remains unknown (Australian Institute of Health and Welfare, 2013; Kelaher et al., 2012).
Overall, study findings showcase the substantial gains in access to mental healthcare for Indigenous populations that can be achieved by concerted national efforts to enhance mainstream primary care services (Jorm and Malhi, 2013; Whiteford et al., 2013). The ATAPS program, through its enhanced Indigenous ATAPS services, provides a successful model to increase Indigenous mental healthcare access by fostering collaboration between mainstream and Indigenous primary healthcare sectors (Holland et al., 2013). This model is of particular relevance to countries with Indigenous and minority populations in which primary care systems provide critical pathways to mental healthcare.
Key strategies to improve future service delivery should focus on enhancing: primary care agency and stakeholder awareness of the full range of flexibilities available through Indigenous ATAPS services (e.g., in terms of provisional referral pathways); service delivery in remote areas; and consumer outcome data collection, including through utilisation of culturally validated outcome measures (Jorm et al., 2012), such as the Kessler 5 which is already available on the minimum dataset. Future longer term research is required to examine consumer uptake and clinical outcomes, as well as key factors underpinning successful implementation and cultural adaptation of Indigenous ATAPS services.
Conclusions
Study findings indicate that concerted national efforts to enhance primary mental healthcare programs can significantly facilitate access to mental healthcare for Indigenous populations.
Footnotes
Acknowledgements
An earlier version of this paper was presented at the 15th International Mental Health Conference at the Gold Coast, Australia, in August 2014.
Funding
This work was supported through funding from the Australian Government Department of Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.