
Abstract

Pridmore, in his Viewpoint in this issue, asserts that experts in the field of suicidology and public health place undue emphasis on the role of mental disorder in the causation of suicide and that this leads to the majority of suicide prevention funding being spent on measures to improve the detection and treatment of mental disorder (Pridmore, 2015). But is this really so? Insel states that ‘the presence of mental illness is a risk factor, but it is not universally present or identified in those who attempt suicide’ (Insel, 2014), a view with which others concur. Regarding funding for suicide prevention, consider the example of the UK where, although some suicide prevention funds have been directed towards reducing risk of suicide in certain high-risk groups, including patients with psychiatric disorders, and improving the detection and treatment of mental disorder in primary care, there has also been investment in other key areas; for example, in reducing access to lethal means, reducing inequalities in certain disadvantaged groups and increasing the availability of psychological therapies.
Systematic reviews have indeed demonstrated that the majority of people who die by suicide or engage in non-fatal self-harm have a mental disorder. The findings of studies examining the prevalence of psychiatric disorders in people dying by suicide in the non-Western world have varied widely, sometimes being lower than those conducted in the West and sometimes being comparable. Interestingly, in a meta-analysis of studies from around the world of self-harm patients presenting to general hospitals, the reported prevalence of psychiatric disorders in non-Western countries was slightly lower than in the West but still high (71% vs 90%; Hawton et al., 2013b).
Regarding the risk of suicide in specific psychiatric disorders, in a recent meta-review of meta-analyses of suicide risk in mental disorders, particularly high rates of suicide were found in borderline personality disorder, where the risk was estimated at 45 times that of the general population, depression (20-fold risk), bipolar disorder (17-fold risk), opioid use (14-fold risk) and schizophrenia (13-fold risk), as well as in anorexia nervosa (31-fold risk) and alcohol misuse or dependence in females (16-fold risk) (Chesney et al., 2014). It is therefore undeniable that there is a strong association between suicide and psychiatric disorders.
So is it important to identify whether or not patients potentially at suicide risk, including those who have self-harmed, have an underlying psychiatric disorder? A primary aim of all mental health services is to alleviate suffering and enhance recovery. The UK government has adopted the slogan ‘No health without mental health’ for its strategy to improve well-being and services for people with mental health problems. Identification of specific psychiatric disorders in patients at risk should then lead to targeted evidence-based therapies aimed at preventing suicide and self-harm, as well as improving mental well-being. For example, there is evidence that a specific form of talking therapy, dialectical behavioural therapy, for people with borderline personality disorder may reduce the frequency of self-harm and the amount of hospitalisation for suicidal ideation when compared with non-behavioural psychotherapy delivered by expert therapists. Regarding the effectiveness of pharmacotherapy in suicide prevention, it was initially thought that clozapine exerted a specific anti-suicidal for people with schizophrenia but in a more recent and large-scale study several other second-generation antipsychotics were found to exert a similar effect in reducing suicides compared to controls (odds ratio (OR), 0.29; 95% confidence intervals (CIs), 0.09, 0.97) (Reutfors et al., 2013). The use of lithium to reduce suicide in bipolar disorder now has a reasonably strong evidence-base. However, the potential role of antidepressants in diminishing the risk of suicide and of self-harm in patients with depression is not established. There is evidence, especially in young people, that initiating these drugs may in a few cases precipitate suicidal ideation, although current thinking is that the reaction of regulatory agencies to this finding may have caused more harm than good.
It is obvious that the majority of people with a psychiatric disorder do not engage in suicidal behaviour, so clearly other risk and protective factors are also in operation. A great deal of research in this field has focused upon identifying and understanding the multiple psychological factors, life events and chronic problems that contribute to suicidal behaviour. Pridmore (2015) rightly highlights the variation in suicide rates between countries and genders, but there are many other important social variables. These include age, ethnicity, employment status, childhood abuse and adversity, social disadvantage, occupation, smoking status and exposure to suicidal behaviour, both within the family and in friends and via the media. A further key risk factor is previous self-harm. In a systematic review and meta-analysis of risk factors for suicide in depression, a past history of self-harm was found to be the strongest predictor of subsequent suicide and substantially elevated the risk of subsequent suicide compared with controls (OR, 4.84; 95% CIs, 3.26, 7.20) (Hawton et al., 2013a). It has been suggested that an episode of self-harm brings about neurobiological, emotional and/or cognitive changes in an individual that directly increases his or her risk of further suicidal behaviour in a process known as ‘kindling’. A similar phenomenon of ‘differential activation’ of suicidal thought across depressive episodes in vulnerable individuals has been described. In older adults, physical illness, bereavement, loneliness and loss of independence are additional important factors.
Pridmore (2015) criticises psychological autopsy methodology and suggests that it is deeply flawed and that this approach should be abandoned. It is certainly true that psychological autopsy studies have some methodological limitations, but the detail, quality and consistency of information collected through interviews with relatives and other informants well acquainted with the deceased, together with details from coroners’ and medical records, is substantially greater than in studies limited to examination of coroners’ or medical records alone, where the information recorded is often selective and limited. Psychological autopsy studies have done much more than just determine whether or not a person who died by suicide was suffering from a mental disorder. They have provided valuable insights into the role that adverse life events, especially inter-personal difficulties, play in the pathway to suicide and have contributed important information that has assisted in the development and testing of psychological factors and theories of suicidal behaviour.
The complex interplay of psychiatric disorders and personality factors with some of the more important psychological and social factors in the development of suicidal behaviour is illustrated in Figure 1. Gender is also an important variable, with suicide being more common in males than females in almost all countries. There are several possible explanations for this finding: males are more vulnerable to socio-economic adversity and to having drug and alcohol problems; they also tend to use more highly lethal and violent methods than females. Additionally, genetic and biological contributions to suicide risk are substantial. It is thought that about 50% of the risk of suicide due to diathesis is inherited and that this percentage may be higher in females than males. Environmental factors such as economic downturn are also important, particularly for males, and it is thought that the increased risk of suicide during economic recession is mediated mainly through the associated increases in unemployment, although threats to financial and work stability may be important in those who remain in employment.
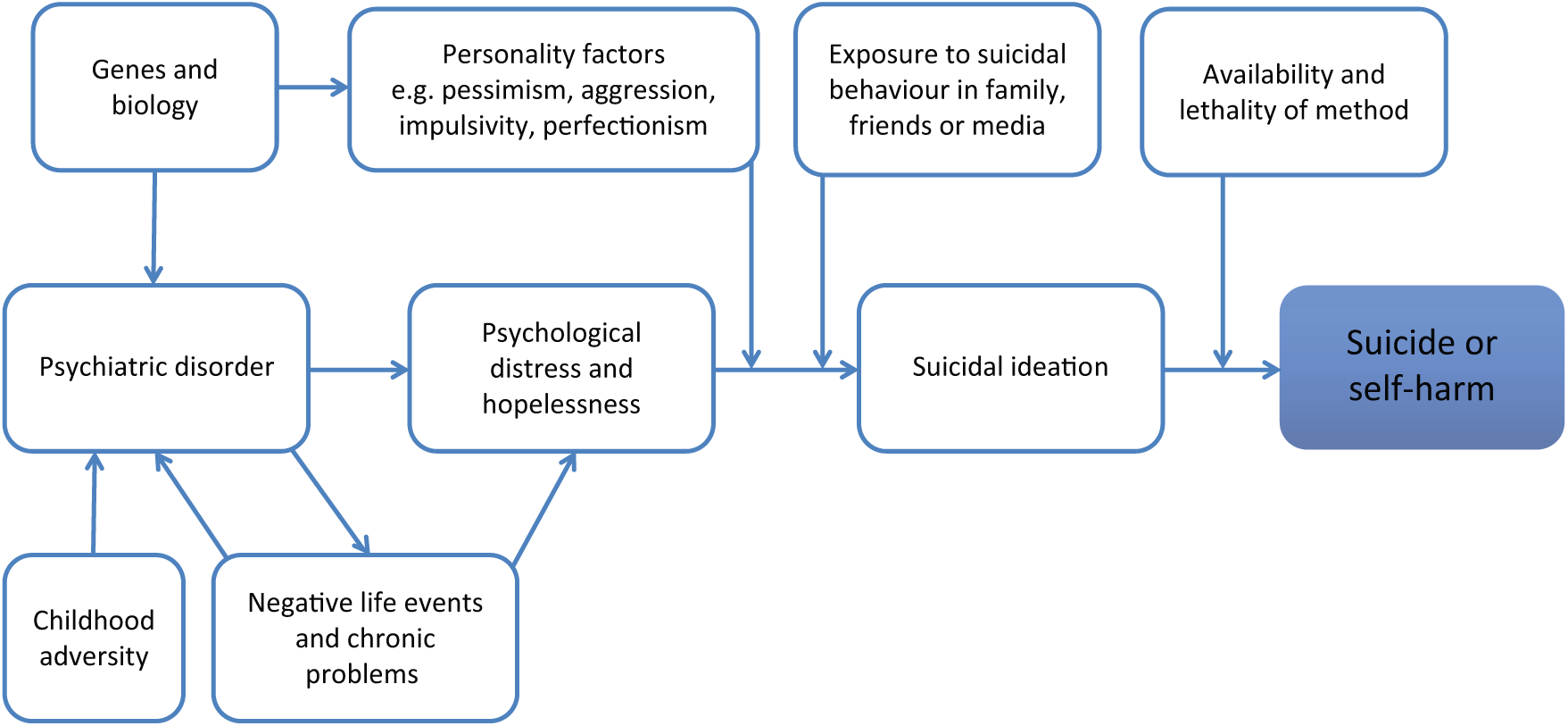
Model of the interplay between psychiatric disorder and some of the bio-psycho-social factors leading to suicidal behaviour.
In planning suicide prevention policies it is crucial that all these factors are addressed if the potential for prevention is to be maximised. To concentrate solely on psychiatric disorders will clearly be insufficient, but their effective treatment and prevention must be an essential component. It is indisputable, therefore, that this be included in all national suicide prevention strategies.
In summary, the causes of suicidal behaviour are complex. They are also not fully understood. Psychiatric disorders alone do not explain why people chose to end their lives but it is an established fact that in the majority of cases there is an underlying mental disorder and there is evidence this vulnerability interacts with multiple psychological and social factors which leads some individuals to end their lives or try to do so. To neglect this is to do a disservice to the people whose deaths we are trying to prevent.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, and not-for-profit sectors. KH is a National Institute for Health Research Senior Investigator.
Declaration of interest
KH is a member of the National Suicide Prevention Strategy for England Advisory Group.