
Abstract

A 33-year-old Vietnamese man (KN) with a 10-year history of schizoaffective disorder was referred for neuropsychiatric assessment with a recent history of apathy, memory impairment, and becoming lost on public transport. His family related the onset of these symptoms to a heroin overdose 3 months previously, at which time he required emergency treatment for respiratory arrest at another institution. KN’s past medical history included osteomyelitis, heroin addiction and hepatitis C, but his only regular medications were olanzapine 10 mg daily and escitalopram 20 mg daily.
On admission, KN’s basic blood tests and physical examination were essentially normal, but cognitive testing revealed substantial short-term memory deficits with relatively preserved remote and autobiographical memory, attention, visual construction, language, and executive function. KN also demonstrated a striking inability to navigate around the hospital, although this elicited neither his interest nor concern.
During his admission a magnetic resonance imaging (MRI) scan was performed demonstrating subtle atrophy and increased T2 signal of both hippocampi (Figure 1A). The finding was felt to be important in the context of KN’s clinical presentation, and prompted a review of the MRI obtained at the time of his respiratory arrest 3 months earlier. When this scan was received, additional abnormalities were identified: both hippocampal heads were swollen with blurred laminar architecture (Figure 1B); there was high T2 signal throughout the head, body and tail of the hippocampi (Figure 1C); and diffusion was restricted (Figure 1D). The findings were consistent with acute hypoxic-ischaemic encephalopathy.
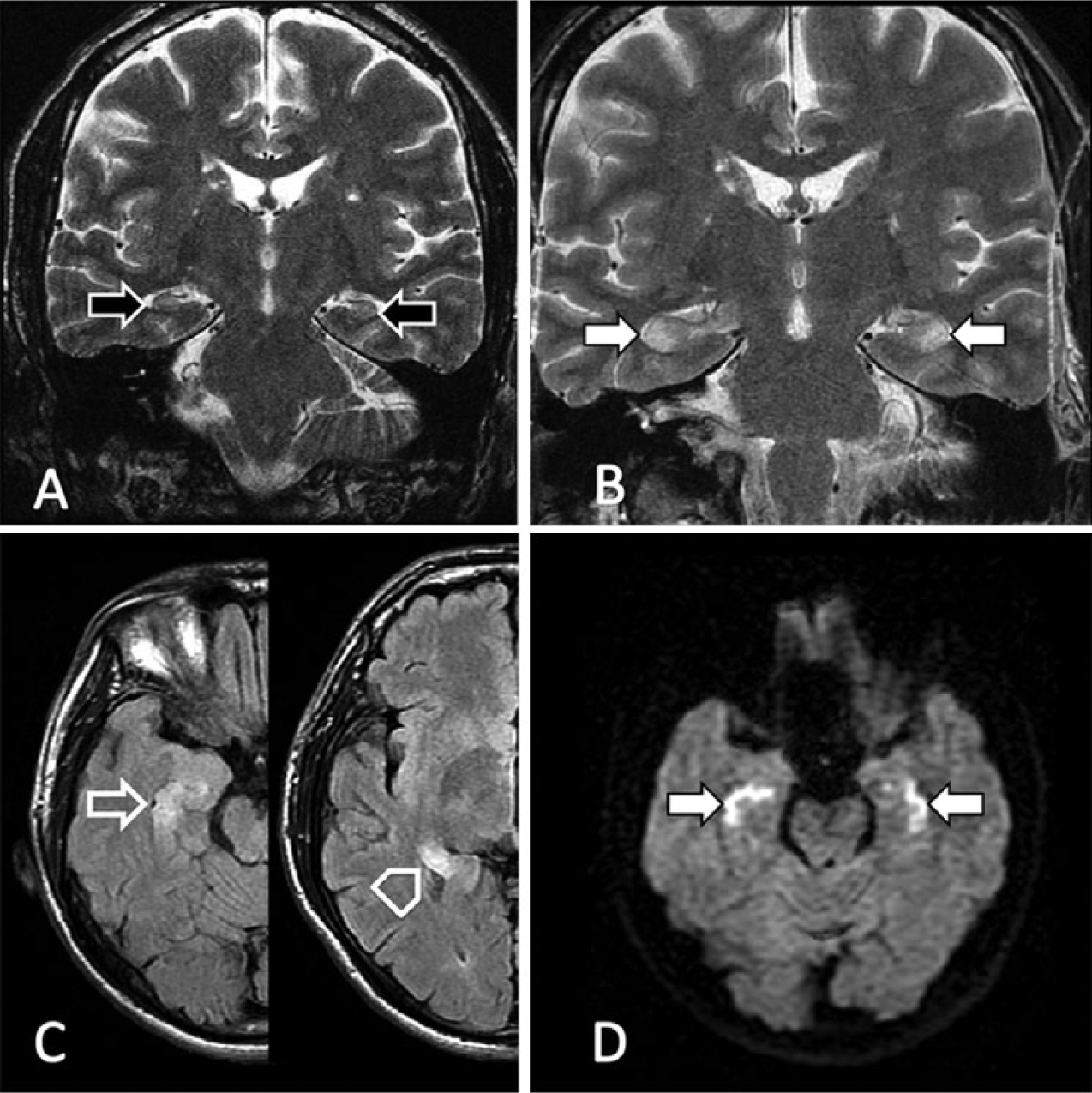
(A) Scan performed on admission demonstrates bilaterally small and high T2 signal hippocampi (black arrows). (B–D) The MRI scan obtained 3 months earlier demonstrates the hippocampi (white arrows) to be symmetrically abnormal. (B) Coronal T2-weighted fast spin echo: high T2 signal involves particularly CA1 and CA2, with mild swelling and blurring of the internal architecture in the affected parts. (C) Axial fluid-attenuated inversion recovery (FLAIR) of the right hippocampal head/body (open arrow) and tail (open arrowhead): high T2 signal extends throughout the hippocampus. (D) Diffusion-weighted imaging (DWI): restricted diffusion (confirmed by apparent diffusion coefficient – not shown) is seen in the areas of high T2 signal, consistent with acute ischaemia.
The pyramidal neurons of the CA1 sub-field of the hippocampus have long been recognised to be particularly vulnerable to hypoxic-ischaemic injury (Smith et al., 1984), with the concept of differential sensitivity of specific neuronal populations originally ascribed to Vogt and Vogt (1937). While unilateral injury of the hippocampus may have negligible clinical consequences, bilateral injury can cause severe anterograde amnesia and focal impairment of spatial and navigational memory (Moser et al., 2008). While each of these symptoms was exemplified by our patient, his diagnosis was initially delayed by their attribution to his premorbid psychiatric conditions.
Besides warning against diagnostic overshadowing, this case demonstrates the important contribution of MRI in elucidating the pathophysiology and facilitating the definitive diagnosis of a complex neuropsychiatric presentation – neither would have occurred in the absence of early imaging, or if a computed tomography (CT) scan had been selected as the preferred modality. The case also highlights the value of retrospectively reviewing all available imaging, as findings crucial to establishing a diagnosis are occasionally overlooked or underappreciated. A close working relationship between psychiatrists and radiologists is essential to this task.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.