
Abstract

To the Editor
A 31-year-old man, John, presented with a history of depression with episodes of disinhibition. He had lost his job as a professional two years earlier and been provisionally diagnosed with bipolar disorder. There was a history of a head injury aged 17 without loss of consciousness or cognitive sequelae. A recent CT scan (Figure 1(a)) was reported by a radiologist as demonstrating frontal changes ‘consistent with a past head injury’.
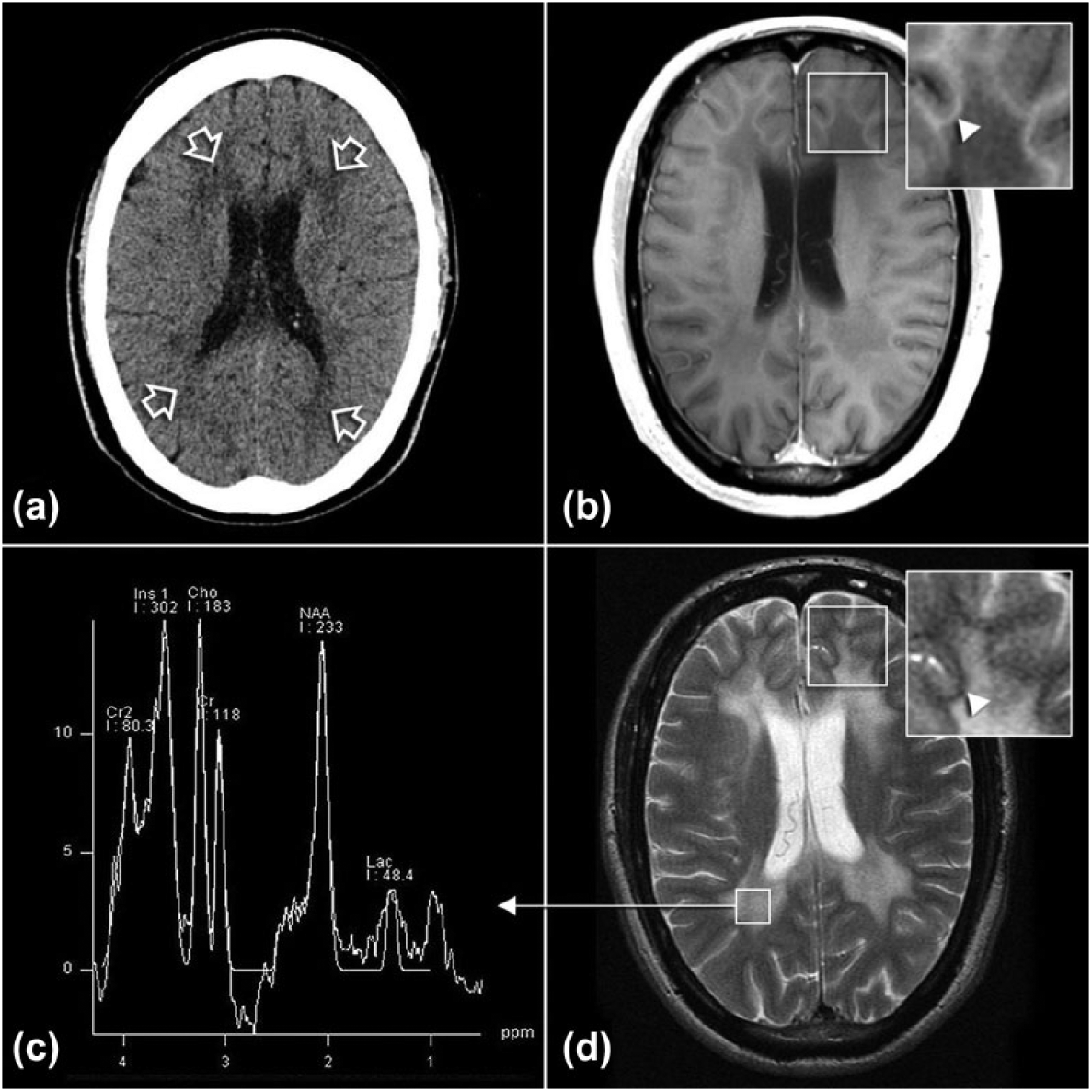
Typical imaging findings of MLD. (A) Non-contrast CT brain demonstrates confluent bilateral periventricular deep white matter hypodensity (arrows) which is hypointense on T1 imaging without contrast enhancement (B) and hyperintense on T2 imaging (D). The abnormality spares the subcortical U fibres (arrowheads, inset B, D). Spectroscopy trace (C) demonstrates elevated myo inositol, reduced N-acetylaspartate and increased lactate.
John was referred for neuropsychiatric assessment of his ‘head injury’ and mood changes. Following the head injury, John had completed high school, a university degree and progressed well through his profession. The history of cognitive decline and behavioural and mood changes had only commenced at around the age of 25. The mental state examination revealed a fit looking, fatuous and disinhibited man. Cognitive assessment revealed memory and executive dysfunction. MRI revealed changes consistent with metachromatic leukodystrophy (Figure 1(b)–(d)). Subsequent testing identified elevated urinary sulphatides. Genetic testing revealed one mutation (c.459+1G>A) with the second yet to be identified.
Metachromatic leukodystrophy (MLD) is the commonest lysosomal storage disorder, with an autosomal recessive pattern of inheritance. A deficiency of the lysosomal enzyme arylsulfatase-A (cerebroside sulfatase) results in accumulation of sulfatides, myelin breakdown and widespread dysmyelination (Kumar et al., 2012). Infantile forms involve gait and movement problems, and mental deterioration. In adult MLD, psychotic symptoms often precede progressive executive deficits, dementia, seizures, chorea or dystonia (Walterfang et al., 2009).
Imaging findings
Classic MRI findings include symmetric areas of high T2 signal within the periventricular and cerebellar white matter (Figure 1) that become confluent with disease progression. A frontal predominance is seen in late onset MLD (juvenile and adult forms), with signal abnormality progressing anterior to posterior (Scott, 2009).
A ‘tigroid’ or ‘leopard skin’ appearance with radially oriented stripes of low signal intensity (normal white matter) within the diffuse symmetric T2 hyperintense white matter abnormality (areas of dysmyelination) has also been described (Van der Voorn, 2005).
MR spectroscopy usually demonstrates decreased NAA (n-acetyl aspartate), elevated myo-inositol and occasionally elevated lactate (Figure 1(c)) (Scott 2009).
Summary
John’s behavioural and affective changes, first diagnosed as a primary mood disorder, were then attributed to a head injury, supported by an abnormal CT. The case highlights two important principles: first, the importance of a detailed history, which revealed that the behavioural and cognitive changes had occurred years after the head injury, and second, the utility of MRI compared with non-contrast CT.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.