
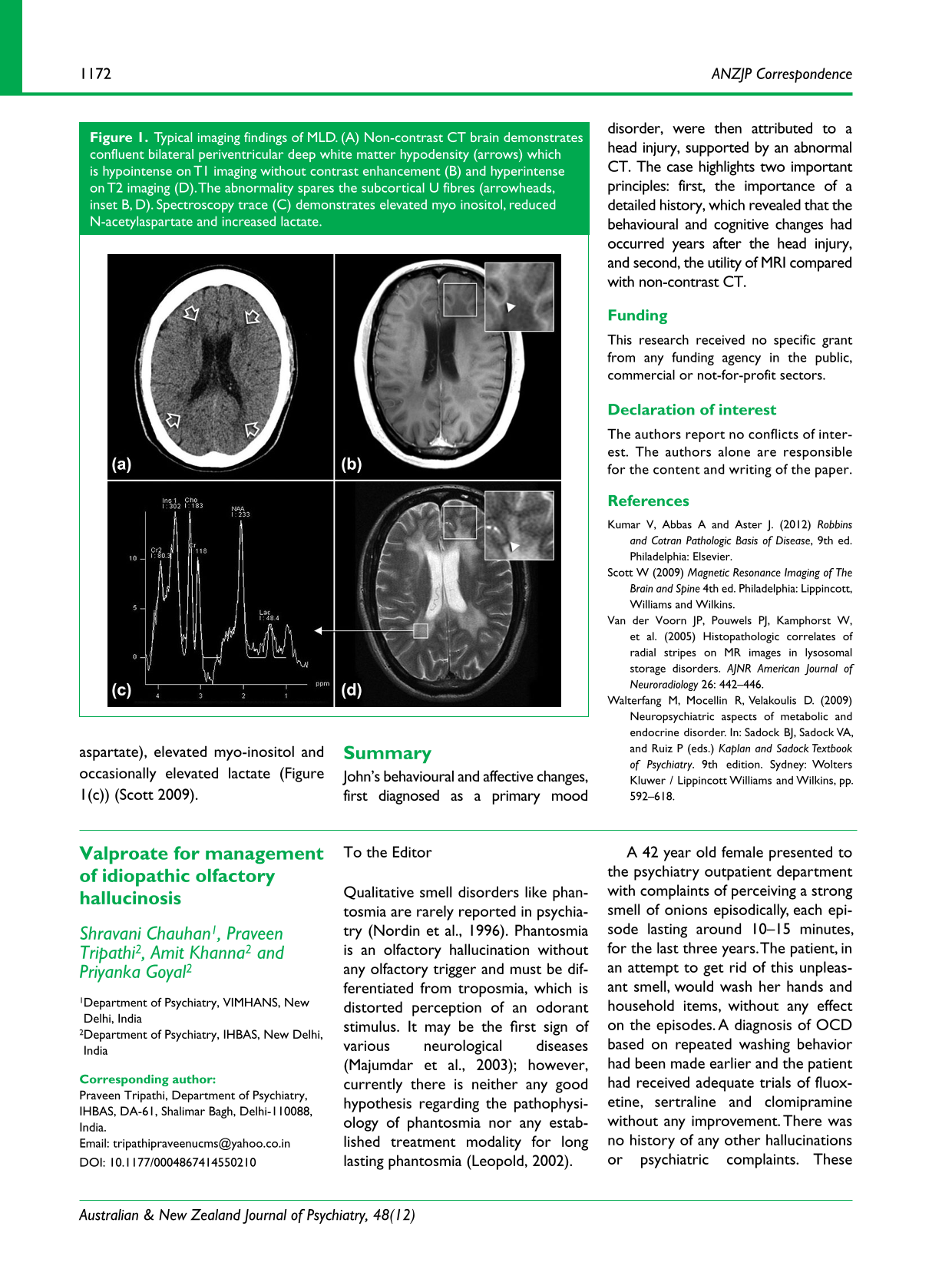
Abstract
To the Editor
Qualitative smell disorders like phantosmia are rarely reported in psychiatry (Nordin et al., 1996). Phantosmia is an olfactory hallucination without any olfactory trigger and must be differentiated from troposmia, which is distorted perception of an odorant stimulus. It may be the first sign of various neurological diseases (Majumdar et al., 2003); however, currently there is neither any good hypothesis regarding the pathophysiology of phantosmia nor any established treatment modality for long lasting phantosmia (Leopold, 2002).
A 42 year old female presented to the psychiatry outpatient department with complaints of perceiving a strong smell of onions episodically, each episode lasting around 10–15 minutes, for the last three years. The patient, in an attempt to get rid of this unpleasant smell, would wash her hands and household items, without any effect on the episodes. A diagnosis of OCD based on repeated washing behavior had been made earlier and the patient had received adequate trials of fluoxetine, sertraline and clomipramine without any improvement. There was no history of any other hallucinations or psychiatric complaints. These episodes were not associated with unresponsiveness or automatisms. There was no significant past or family history and she was not on any medications.
The patient was provisionally diagnosed with idiopathic olfactory hallucinosis and, after ruling out depression and psychosis, her symptoms were thought to be either migrainous or epileptiform. Electroencephalography and magnetic resonance imaging were found to be normal. Results of hematological and serum biochemical analyses were normal.
The patient was given a trial of valproate at a dosage of 800 mg/day. She showed significant improvement with marked decrease in both the number and duration of episodes. Valproate was continued and the patient showed sustained improvement in the hallucinations.
Cases of the above-mentioned olfactory hallucinosis are rarely seen in psychiatry clinics and the pathophysiology of olfactory hallucinations is far from clear. Some have suggested the activation of reverberating neuronal circuits such as in memory networks. The various possible mechanisms could be aberrant firing of action potentials at the periphery, loss of inhibitory fibers, abnormalities of the odor-binding proteins, disturbed central cortical processing or misinterpretation of other sensory signals (Majumdar et al., 2003). Several medications, including sedatives, anti-depressants and anti-epileptic drugs, have been suggested to treat olfactory distortions (Majumdar et al., 2003). In our case, absence of any imaging or electroencephalographic abnormalities and resolution of symptoms with anti-epileptic medications prompted us to consider that reverberating circuits and abnormal signal generation may have been responsible for the hallucinations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.