
Abstract

Psychiatric services have been transformed over recent decades (Carr and Waghorn, 2013) and the rate of change shows no sign of diminishing. Taking up this issue, Jorm and Malhi (2013) began a discussion of the evidence base for mental health services reform in Australia. Their Editorial was accompanied by three invited Viewpoints with expert opinions on the relevant mental health services research (Carr and Waghorn, 2013; Castle, 2013; Whiteford et al., 2013). The Editors invited readers to comment on the Viewpoints ‘so that we can have an ongoing discussion that may eventually converge on a consensus’. This discussion of evidence-based reform represents a further development of the Journal as a forum for policy debate in Australia and New Zealand.
Taken together, the Editorial and Viewpoints outlined the key aspects of health advocacy and lobbying governments on behalf of these reforms. The phases included reaching a consensus on the research evidence through the Journal (Jorm and Malhi, 2013); the College and other peak medical groups such as the Australian Medical Association (AMA) acting as spokespersons for mental health reform (Castle, 2013); and engaging with the political, media and administrative processes required for reform (Whiteford et al., 2013).
Since this time, the health debate has changed radically with the 2014 Australian Budget. The Federal Health Minister has expressed concerns that health spending is unsustainable following an increase from 19.8% to 25.6% of Australian total tax revenues in the last decade (Richardson, 2014). The Federal Government resolved to make savings on future health spending. Significant budget cuts were proposed, which will have an impact on the delivery of front-line mental health services. This budgetary restraint makes it more likely that the next wave of mental health ‘reform’ may lead to reductions in bed numbers, community services and Medicare funding.
Australia’s mental health system starts from a relatively vulnerable position entering this new period of austerity. Our proportion of the health budget is relatively low compared to comparable western countries such as the United Kingdom. While Australia and the UK spend similar proportions (9.5% vs 9.4%) of their gross domestic product on health, Australia invests considerably less (7.6% vs 10.8%) of the total health budget on mental health (Richardson, 2014; World Health Organization, 2011).
The Federal Budget cuts proved to be highly contentious. The cuts were partly designed to reduce funding for State-based health services and the South Australian Labor Government Health Minister encouraged public servants, including psychiatrists, to join a ‘Day of Action’ to protest against the Federal Coalition Government Budget (Crouch, 2014). This call presented a dilemma for psychiatrists who might be understandably reticent about political involvement while in their professional roles. But it did raise the question: How actively should we advocate and lobby governments over funding for mental health services? What principles and practices should guide our health advocacy and lobbying?
Health lobbying can be highly effective. In the United States, for example, professional lobbyists have been instrumental in the US spending greater amounts on health than comparable countries but arguably with poorer and less equitable outcomes. Currently, the US spends a massive 17.7% of their gross domestic product on health (Richardson, 2014). During the Congressional debates about the Obama administration’s health care reforms, the health sector spent enormous amounts on lobbying in Washington (Steinbrook, 2009). There are, however, substantial differences between the politics, legislation and funding of health in Australia and the US.
In Australia, health advocacy and lobbying are generally much less intensive. This is recognised as a potential problem and greater efforts could be required to ensure adequate government funding for front-line mental health services (Castle, 2013). Ideally, health advocacy would be built upon strong partnerships between peak professional groups such as the College and the AMA (Castle, 2013). In political terms, the AMA clearly has the national profile and the capacity to lead debates around health funding, as seen in the media after the 2014 Federal Budget.
Public advocacy and lobbying are inherently political activities even when rigorously evidence-based and non-partisan. Reform tends to progress in rapid and non-linear ways. For instance, Whiteford and colleagues (2013) highlighted the unpredictable role of the media in political decision-making. Personal relationships can play a major role. A politician may be more open to health lobbying when he or she has direct experience with a condition and understands the impact. It is probably fair to say that these considerations have influenced some crucial decisions in regard to funding for the treatment of mental illness in Australia, and on balance it has been welcome.
The College has adopted the professional framework of the Royal College of Physicians and Surgeons of Canada (CanMEDS) to better define psychiatrists’ public roles in health advocacy. Within the CanMEDS health advocate role, psychiatrists are expected to ‘use their expertise to advocate on behalf of individual patients, their families and carers, as well as more broadly, on the epidemiological level’ (Royal Australian and New Zealand College of Psychiatry, 2012). This is consistent with medical opinion suggesting that doctors have both an obligation and the expertise to promote the health of the wider community (Gruen, 2008).
While health advocacy is recognised as part of our brief, doctors’ public roles have not been fully delineated (Gruen, 2008) and there are potential conflicts with the other CanMEDS roles for the medical expert. In the CanMEDS Framework, the health advocate role sits neatly between the scholar and manager roles (Figure 1). Tensions can arise at these interfaces. The manager role includes clinical governance in health care settings where public service rules and governmental attitudes limit acceptable advocacy for employed doctors. In fact, health advocacy may be counterproductive, with effective advocates being excluded from the decision-making process.
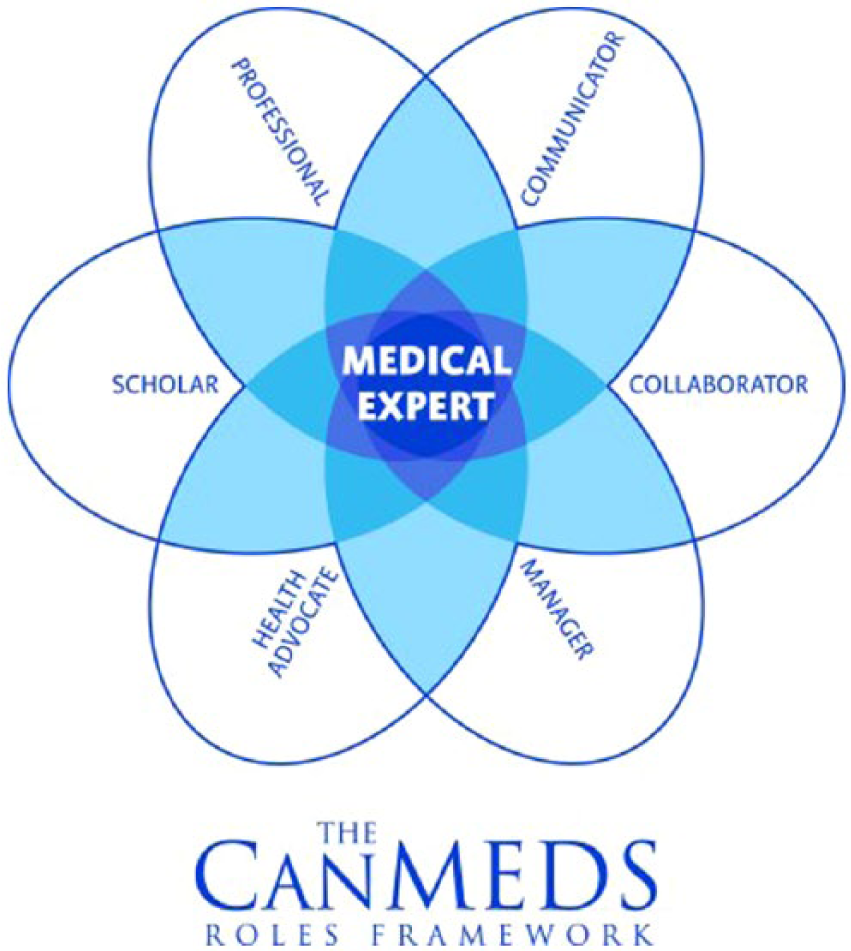
Health Advocate, Manager and Scholar are recognised as key roles of the Medical Expert within the CanMEDS Framework. Copyright © 2009 The Royal College of Physicians and Surgeons of Canada. http://rcpsc.medical.org/canmeds. Reproduced with permission.
In addition, the political roles of health advocacy and lobbying require a different orientation and skill sets compared to the scientific role of the CanMEDS scholar. Scholarship tends to be sceptical and incremental by nature; in contrast, politics is rhetorical, a field where ‘everyone exaggerates everything all of the time’. The issue of exaggeration is important to discuss further because while it appears necessary and expected in the political context, it may require psychiatrists to move beyond the strict and often incomplete evidence base for mental health services reform.
In conclusion, the 2014 Budget defined the current political contest. The budget cuts are likely to impact on the delivery of Australian front-line public and private psychiatric services across the States and local communities. Broadly, the challenge is to continue mental health services reform during difficult times. The Editorial and Viewpoints began an ongoing discussion of the evidence base for reform in the pages of the Journal. This discussion could be extended to the public roles for trainees, psychiatrists and the College at large in progressing the reform agenda in non-partisan and evidence-based ways. This focus of inquiry could better define the potential and the limits of the CanMEDS health advocate role for psychiatry. Most importantly, it could increase the preparedness of the profession to argue for a positive reform agenda during a budgetary contraction.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.