
Abstract

To the Editor
A 68-year-old woman with a 25-year history of schizophrenia presented with a 3-month history of persecutory delusions, amotivation, personality change and forgetfulness. She complained of headaches she believed were caused by her neighbours, whose voices she could hear abusing her. Prior to this, she had been on antipsychotic medication and free of psychotic symptoms for over 10 years. She exhibited impairments in attention, orientation, memory, drawing reproduction, calculation, left–right orientation, and praxis. The patient’s presentation was considered atypical for a relapse of schizophrenia.
Magnetic resonance imaging (MRI) of the brain obtained with contrast (Figure 1) demonstrated a 3 cm mass located anteriorly in the interhemispheric fissure, between the frontal lobes and above the corpus callosum which it distorts (C). The mass demonstrated a low signal centrally on all sequences, in keeping with calcification, and a rim of enhancing tissue around the periphery (B). Extensive vasogenic oedema involving both frontal lobes was seen as a high T2 signal on the axial fluid attenuation inversion recovery (FLAIR) image (A). There was no appreciable diffusion restriction (D) and the remainder of the brain was unremarkable.
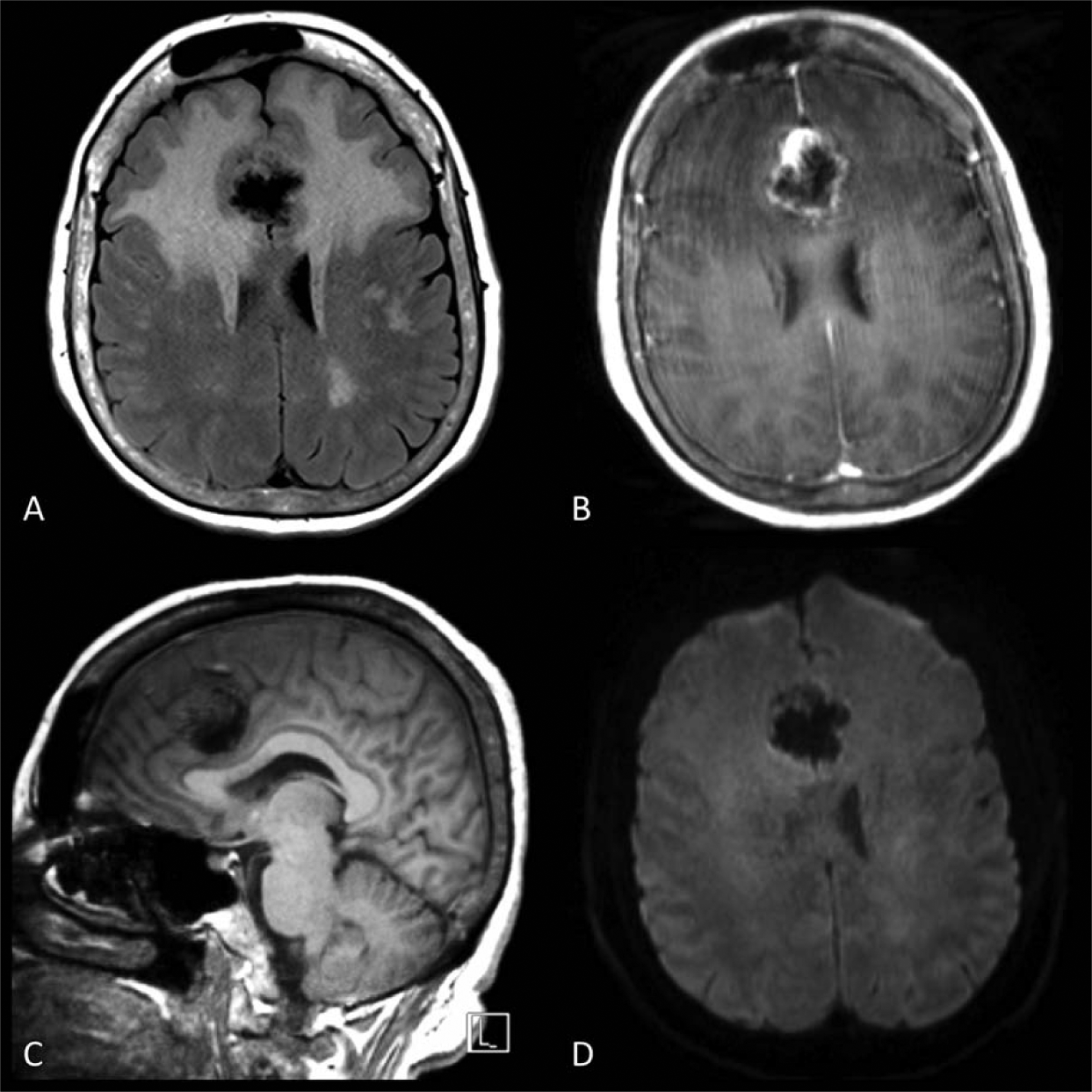
The imaging was consistent with a frontal falx meningioma, and the patient proceeded to complete surgical removal. Her presenting symptoms subsequently resolved and she returned to her premorbid level of function.
Meningiomas are treatable, slow-growing and mostly histologically benign tumours of the central nervous system with a pathologically confirmed prevalence of around 1/1000 (Dolecek, 2012). The clinical manifestations of frontal meningioma are often non-specific and late to present, but in patients with mental illness they may mimic past symptoms and delay diagnosis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.