
Abstract
Aim:
To retrospectively examine the outcomes of forensic patients found not guilty by reason of mental illness (NGMI) in New South Wales (NSW) and subsequently released into the community, as measured by reoffending, conditional release revocation and psychiatric hospital readmission.
Method:
Data were collected from the NSW Mental Health Review Tribunal (MHRT) files for all patients who received an NGMI verdict between January 1990 and December 2010, and who were released into the community during this period. The outcome measures of conditional release revocation and psychiatric hospital readmission were extracted from these files. Information about subsequent criminal charges, convictions and penalties were obtained from the Bureau of Crime Statistics and Research’s reoffending database.
Results:
During the 21-year period studied, 364 offenders received an NGMI verdict and were placed under the supervision of the MHRT. Of these, 197 were released into the community, including 85 who were granted unconditional release. Over a follow-up period averaging 8.4 years, 18% of conditionally released patients reoffended, 11.8% were convicted of a further offence, 8.7% were charged with a violent offence, 3.1% were convicted of a violent offence and 3.7% were sentenced to a term of imprisonment. Five (3.1%) conditionally released forensic patients received a further NGMI verdict. One-quarter of the conditionally released patients had their conditional release revoked and half were readmitted to hospital. Of the forensic patients granted unconditional release, 12.5% were charged with an offence, 9.4% received convictions for an offence, 6.3% were charged with a violent offence and 4.7% were convicted of a violent offence, in a mean follow-up period of 7.6 years. None committed a further serious offence resulting in a term of imprisonment, nor a second NGMI verdict.
Conclusions:
The results of this study suggest that the treatment and rehabilitation of forensic patients in NSW, together with the decision-making procedures of the MHRT, is effective in protecting the community from further offending by forensic patients.
Keywords
Introduction
Many jurisdictions have provisions for the supervision and treatment of mentally ill offenders given a verdict of not guilty by reason of mental illness (NGMI), referred to in this paper as ‘forensic patients’. Information about the progress of forensic patients released into the community, especially about their subsequent violence and offending, is important for informing release decisions, policy development and service delivery. However, there have been surprisingly few published studies about the outcome of people found NGMI (Boyd-Caine and Chappell, 2006; Latimer, 2006).
Research into the outcome of released forensic patients has mainly considered rates of reoffending, although other measures are also important, including adherence to conditions of release, readmission to hospital and overall social function (Tellefsen et al., 1992). There is no generally agreed estimate for the rate of reoffending among people released to the community after an NGMI verdict. This might be due to the differences between jurisdictions in the way that NGMI findings are reached, variation in services provided to patients both during detention and after release, and differences in the way decisions to release forensic patients are made. Moreover, different outcomes in similar jurisdictions may reflect changes in treatment and release policies over time. Several early follow-up studies were conducted prior to the introduction of modern rehabilitation services (such as medium-secure units and community treatment of forensic patients) and developments in anti-psychotic medication (such as the wider use of clozapine), which might have reduced reoffending by forensic patients (Coid et al., 2007).
Although there have been meta-analyses of recidivism among mentally disordered offenders as a whole (Bonta et al., 1998; Fazel and Yu, 2011; Izzo and Ross, 1990), there has been no meta-analysis of the outcome of people found NGMI. Researchers have found it difficult to employ meta-analytic techniques to study this population because of differences in the rates of NGMI verdicts, measures of recidivism, duration of detention, community treatment, criteria for release and follow-up periods (Caffrey, 2005; McGuire, 2000).
The rearrest rate has been considered to be a more sensitive measure of recidivism than conviction because it includes forensic patients who are dealt with under mental health provisions rather than convicted of further offences (Maltz, 1984). Reported rates of rearrest among released forensic patients vary widely, ranging from 5.8% (Wiederanders, 1992) to 63% (Tellefsen et al., 1992). Harris (2000) noted that patients were most vulnerable to rearrest in the first 2 years after release, and found a linear relationship between reoffending and the duration of follow-up.
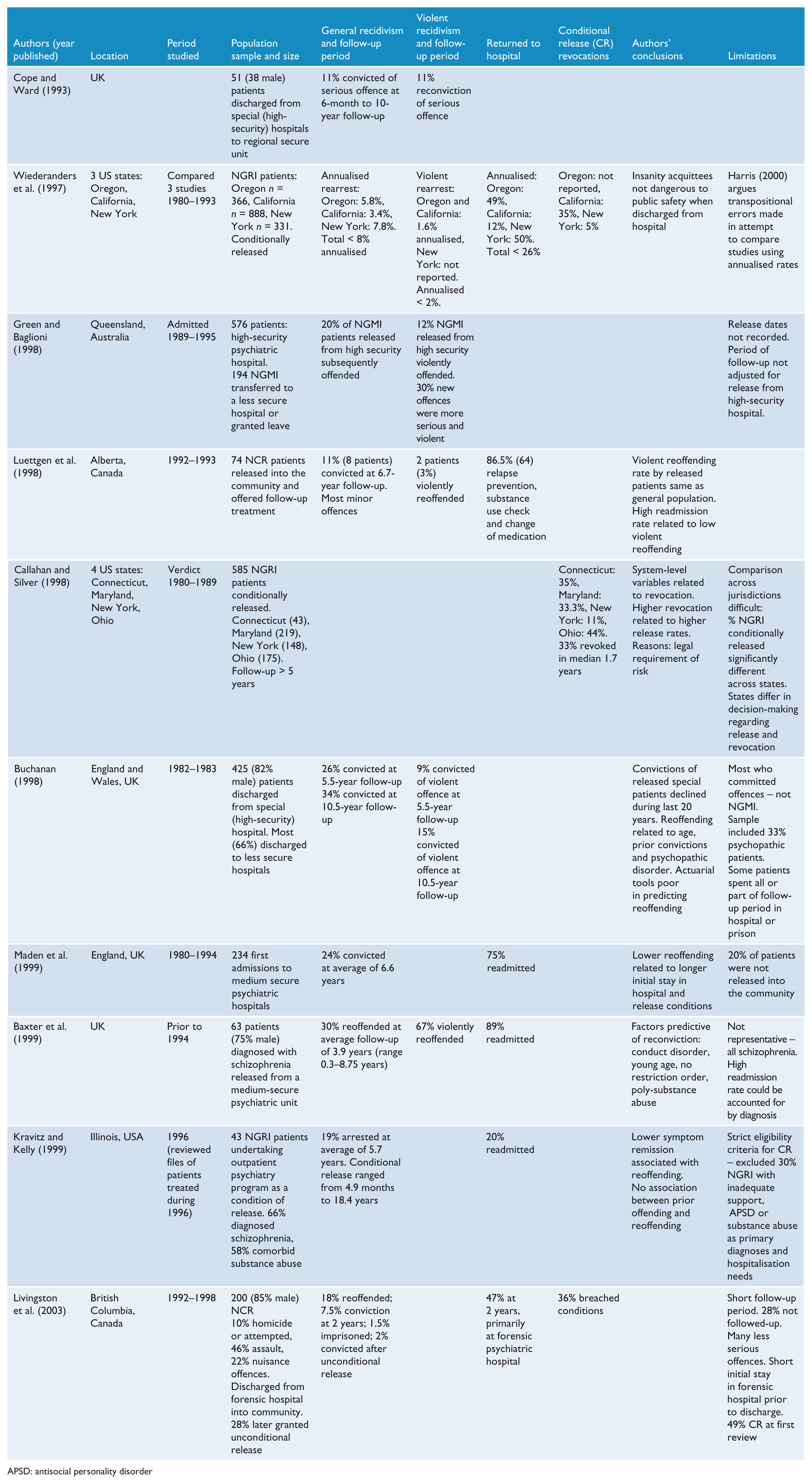
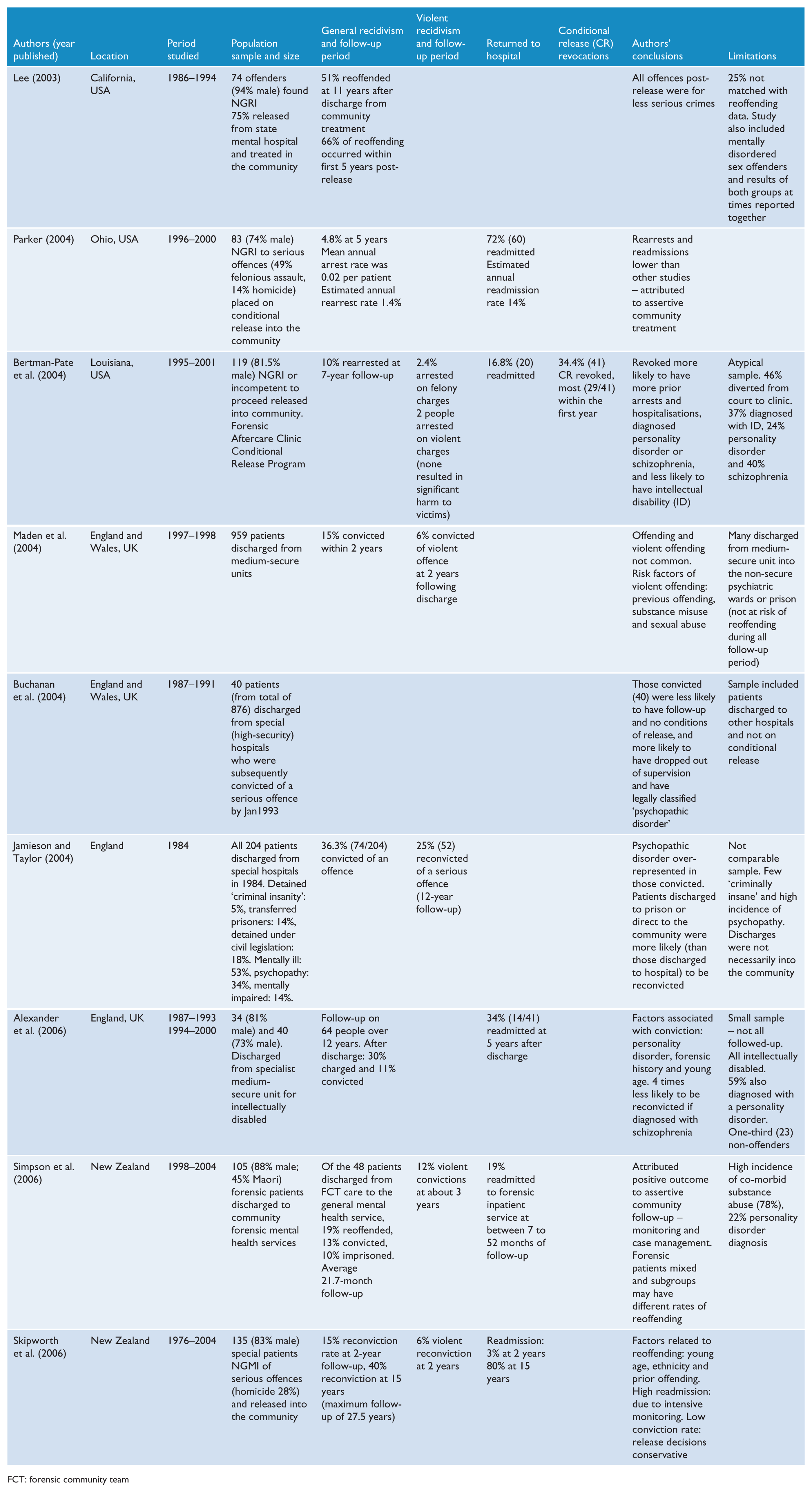
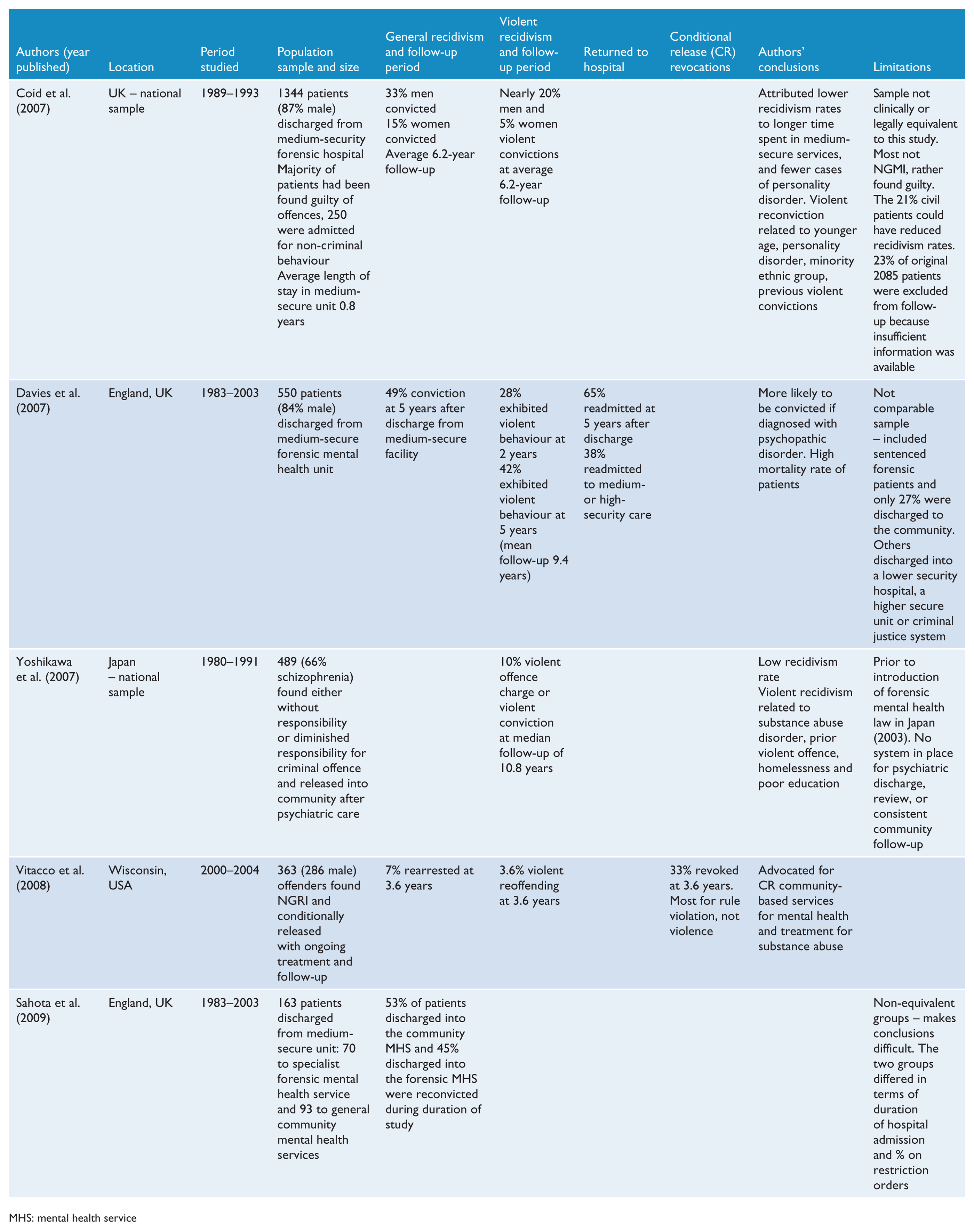
Rates of violent reoffending following release are of the greatest concern to the community, and have ranged from 4% at 3.6 years (Vitacco et al., 2008) to 20% at an average period of 6.5 years after discharge (Rice et al., 1990). Higher rates of violent recidivism are found in samples that included mentally disordered offenders released from high-security hospitals, and range from 6% at 2 years to 20% at 6.2 years (Baxter et al., 1999; Coid et al., 2007; Maden et al., 2004). When conviction rates for violent offences rather than charges are reported, rates are slightly lower and range from 6% at 2 years up to 15% at 10 years (Buchanan, 1998; Skipworth et al., 2006). The results of outcome studies published since 1990 are summarised in Table 1.
Summary of published studies on outcome of released forensic patients since 1990.
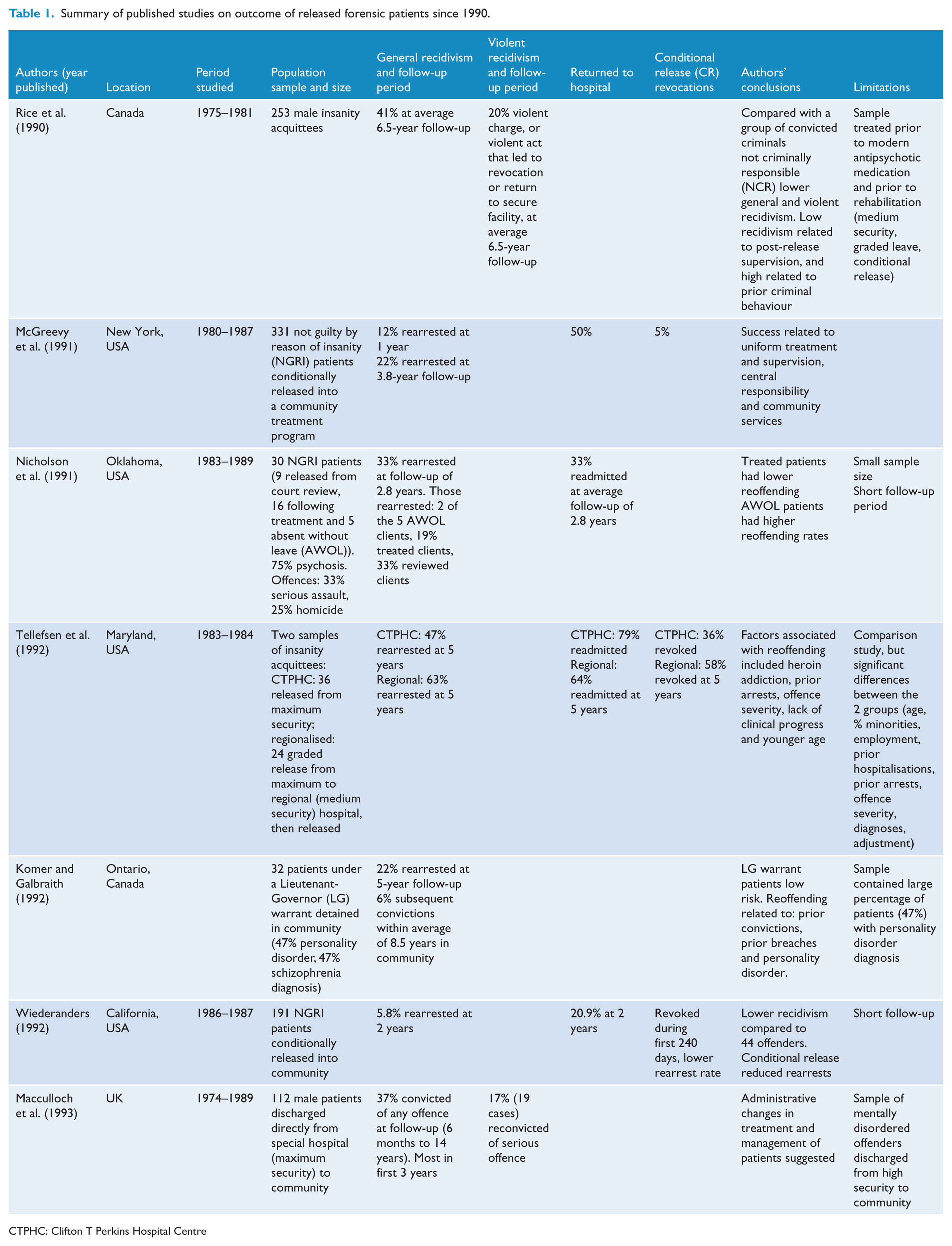
CTPHC: Clifton T Perkins Hospital Centre
APSD: antisocial personality disorder
FCT: forensic community team
MHS: mental health service
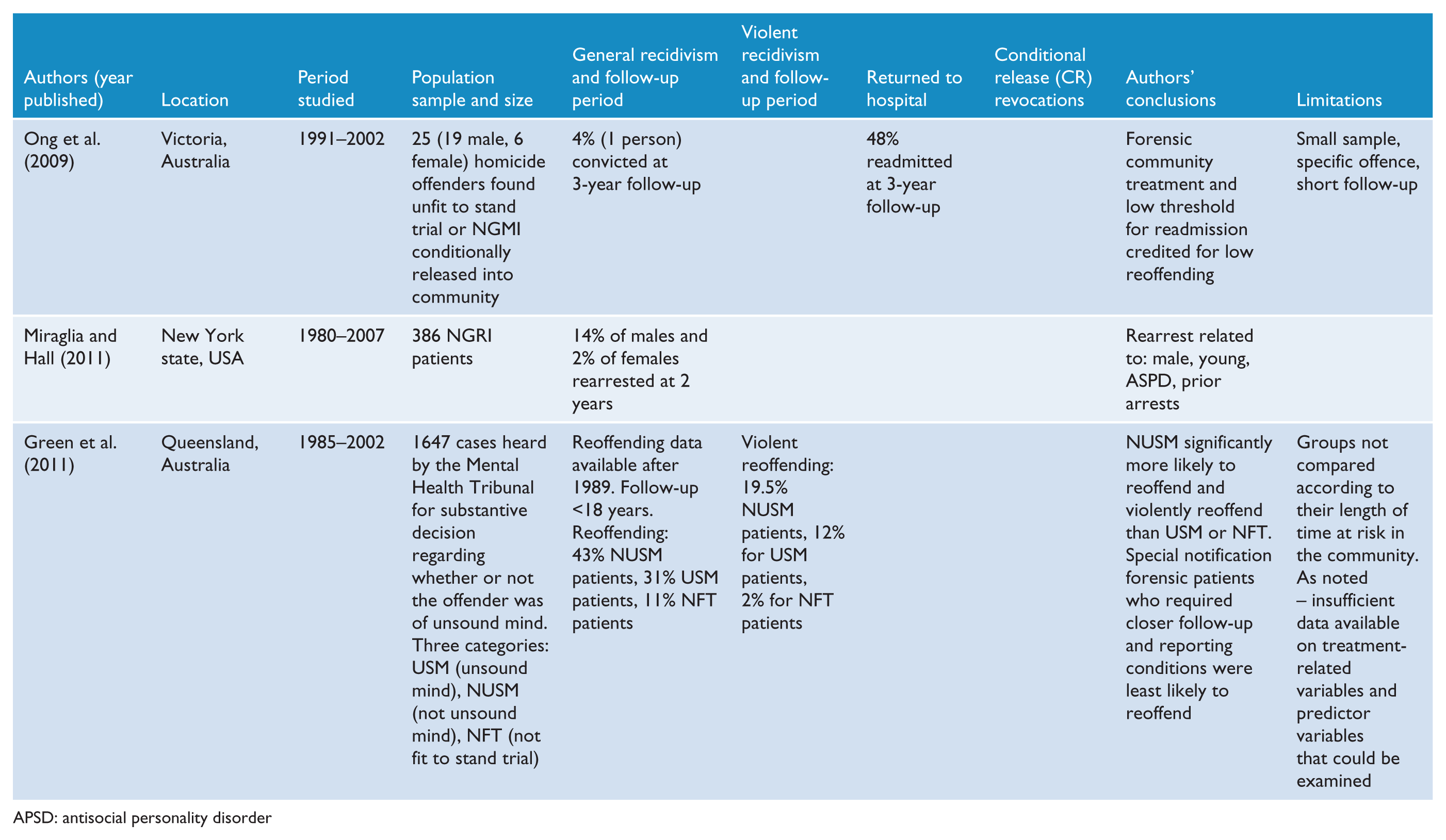
APSD: antisocial personality disorder
Rearrest rates appear to be reduced by assertive aftercare and supervision following conditional release programs (Bertman-Pate et al., 2004; McGreevy et al., 1991; Parker, 2004; Vitacco et al., 2008; Wiederanders, 1992). Conditional release allows for the continuing treatment of forensic patients gradually released into the community, with ongoing monitoring, power to revoke release and the option of returning the patient to secure hospital care (Bloom et al., 1991). The reported rates of revocation of conditional release range from 5% to 36% (Livingston et al., 2003; Wiederanders et al., 1997).
Rearrest rates might also be reduced by psychiatric hospital readmission (Luettgen et al., 1998), although it is difficult to determine the relationship between the two outcomes as so few studies have reported on the rates and circumstances of readmissions of forensic patients following their release into the community. There is wide variation in the reported rates of rehospitalisation of 19% to 47% within 3 years of release (Livingston et al., 2003; Simpson et al., 2006), which increases in studies with longer periods of follow-up. For example, 80% of forensic patients in New Zealand were readmitted within 15 years after release (Skipworth et al., 2006). It is likely that there is some confusion between hospital readmission and conditional release revocation rates, as in some jurisdictions admission to hospital can take place without revoking conditional release.
The aim of this study was to determine the outcome of offenders found NGMI and placed under the supervision of the Mental Health Review Tribunal (MHRT), who progressed through the forensic hospital system in New South Wales (NSW) and were released into the community. The outcome measures included criminal charges and convictions for all offences and for violent offences, the penalties imposed on conviction, revocation of conditional release and rehospitalisation, for forensic patients granted both conditional and unconditional release.
Method
Sample
A list of all people found NGMI between 1 January 1990 and 31 December 2010 was drawn from the MHRT’s client management system. The Mental Health (Forensic Provisions) Act 1990 (NSW) established the role of the MHRT in the supervision of those found NGMI of indictable offences in the District and Supreme Courts of NSW, according to the common law standards known as the McNaughton rules (R v McNaghten (1843)) and the Porter Test (R v Porter (1933)). Patients were included in this study if they were released, either conditionally or unconditionally, prior to 31 December 2010. Forensic patients who were sentenced prisoners transferred from correctional facilities, and offenders who received a ‘limiting term’ after a finding that they were permanently unfit to stand trial were excluded from this study.
Data collection
Information regarding each patient was extracted from the comprehensive MHRT files, which included legal documents (such as police facts, judgements, and orders for detention and release) and reports by mental health professionals (including assessments and reports on the progress of treatment). There was an outcome summary for each 6-monthly review conducted by the MHRT, which contained a synopsis of the case, summary of the patients’ progress, statement of current leave entitlements, and reasons for recommendations for leave, release or revocation of leave. Owing to the archival nature of this research, sections from the files of seven forensic patients could not be located. However, there were sufficient data to include these cases in the analyses.
The following data were extracted:
demographic information: name, aliases, date of birth, sex, marital status, birth place, cultural background, years of education, occupation, living arrangements, employment;
clinical information: psychiatric diagnoses, age at diagnosis, substance use, prior treatment and prior psychiatric admissions, history of head injury;
criminal history: age of first offence, prior convictions, previous convictions for violent offences, previous imprisonment;
offence details: date of offence, most serious offence, relationship to victim, number of victims, use of weapons;
progress through the forensic mental health system: dates of offences, date of apprehension, date of verdict, fitness for trial, dates of transfer between facilities, leave privileges granted, date of conditional release, date of unconditional release, number and reasons for breaches, dates of revocations of conditional release, readmission to psychiatric facilities, location at census date.
Reoffending data
The database of released forensic patients was matched with the NSW Bureau of Crime Statistics and Research (BOCSAR) reoffending database (ROD) and included criminal charges, dates of offences, hearing outcomes and penalties up to 31 July 2011. Offences were recorded according to the Australian and New Zealand Standard Offence Classification (ABS, 2011).
The matching process
The database of released forensic patients was linked with BOCSAR’s reoffending database, which was established in 1994. Reoffending was defined as a recorded charge resulting in a court appearance for any offence after release into the community. The matching process was performed using the patient’s name (and any known aliases) and date of birth (Hua and Fitzgerald, 2006). In cases where matches could not be found, additional available information was used (including identification numbers from prison files, police files and court files). No matches were found for 13.7% of cases (27/197). For patients with a verdict after the establishment of ROD in 1994, matches were found for 94.8% (164/173); whereas successful matching occurred in 25% (6/24) of cases prior to 1994. Owing to problems with records in the early years, it was decided to exclude cases with an NGMI verdict prior to 1994 from the analysis of reoffending.
Census
The MHRT’s client management system was used to establish the location of each conditionally released patient on 31 July 2011.
Statistical analysis
Statistics were performed using SPSS version 21. Survival analyses used the Kaplan–Meier estimator and calculated the percentage of released patients (adjusted for cases lost due to reaching the date of census, or death) residing in the community over time, from their date of release until the particular event studied. The events studied included the date of conditional release revocation, date of first offence following release, and date of first violent offence after conditional release.
Chi-squared tests were used to analyse the significance of variable hypotheses to predict outcomes such as rehospitalisation, revocation of conditional release and reoffending following release. Fisher’s exact tests were employed for comparisons when any one cell had an expected value of less than 5. Binary logistic regressions were used to test the independent predictive ability of significant variables. The results of these analyses are contained in the Supplemental Data.
Ethical review
Approval to conduct the study was granted by the Human Research Ethics Advisory Panel (Psychology) of the University of New South Wales. The Mental Health Tribunal case files were accessed with permission in accordance with the Health Records and Information Privacy Act 2002 (NSW), and linkage to the reoffending database was approved consistent with the NSW BOCSAR’s code of practice under the Privacy and Personal Information Protection Act 1998 (NSW).
Results
Overview
Between the beginning of 1990 and the end of 2010, 364 people received a verdict of NGMI in the NSW higher courts and became forensic patients under the supervision of the MHRT. By 31 December 2010, 197 of these forensic patients had been released into the community. In all, 54% of those found NGMI after the establishment of the MHRT in 1990 had been released to community care. A total of 186 forensic patients were granted conditional release during the period of study and 74 of these patients progressed from conditional release to unconditional release status. A further nine patients were granted unconditional release without a prior period of conditional release, and the pathway (prior to unconditional release) of another two could not be established, making a total 85 forensic patients who had been granted unconditional release by 31 December 2010. A further 112 forensic patients were granted conditional release, but not unconditional release, during the period of study (Figure 1).
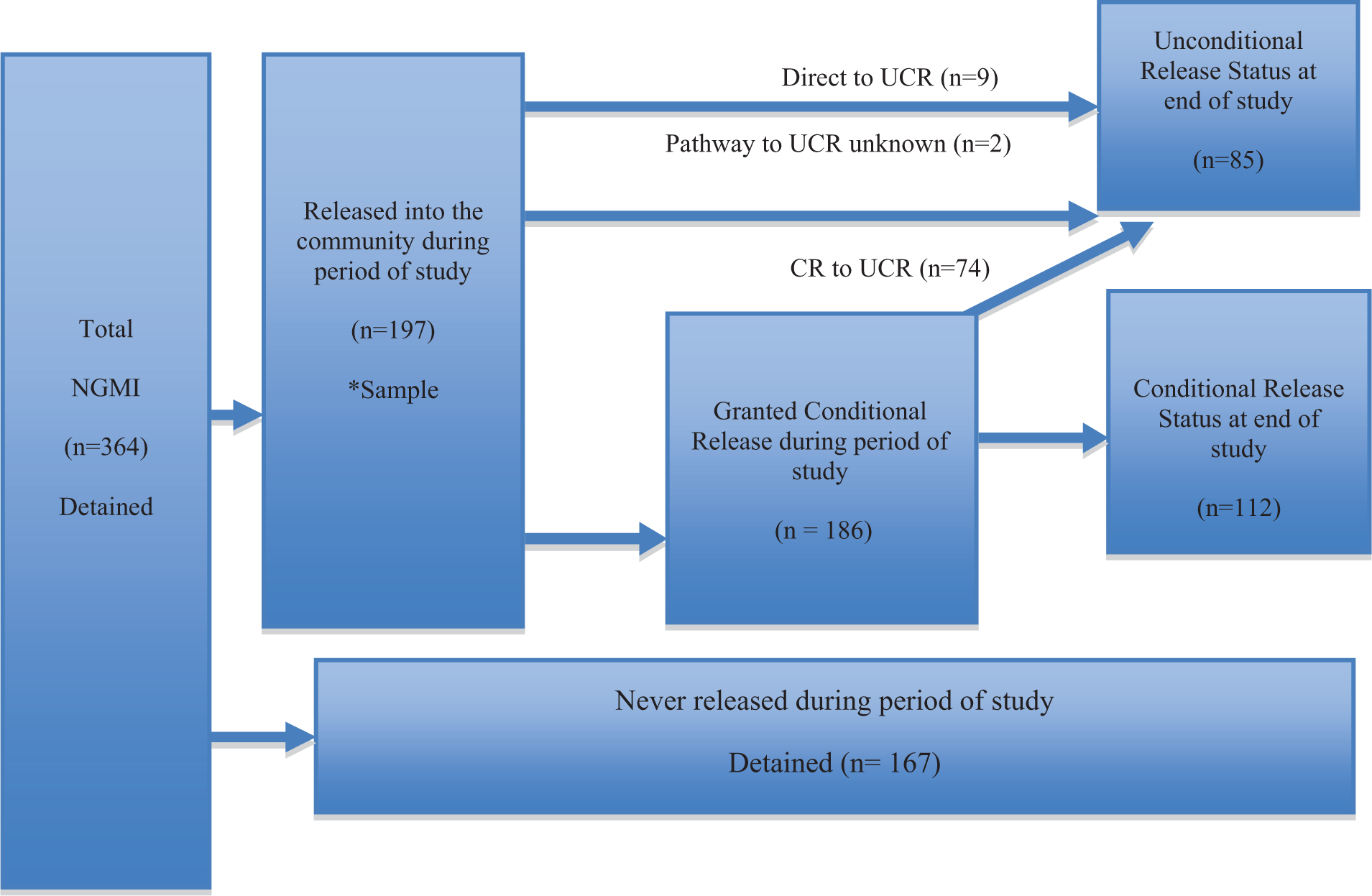
Overview of forensic patients in NSW (January 1990 to December 2010).
Demographic features
Of the 197 released patients, 168 (85.3%) were male, and the average age at the time of the NGMI verdict was 36 years (range 16–82). Twenty-six (13.2%) patients subsequently found NGMI at special hearings had been found to be permanently unfit to stand trial, of whom 18 were diagnosed with a treatment-resistant form of mental illness, four with dementia (three comorbid), one with permanent organic brain injury and two with a comorbid intellectual disability. A schizophrenia-related psychotic illness was the primary diagnosis in 165 (83.8%) cases and 19 (9.6%) were diagnosed with mood disorder. A comorbid substance abuse disorder was diagnosed in 102 (51.8%) cases, 14 (7.1%) had borderline or mild intellectual disability and 16 patients (8.1%) were found to have symptoms consistent with the diagnosis of antisocial personality disorder. Prior contact with mental health services was reported in 146 (74.1%) cases and 123 (62.4%) had had at least one previous admission to a psychiatric hospital. The main offences were homicide (57, 28.9%), attempted murder (37, 18.8%), wounding or grievous bodily harm (34, 17.3%), armed robbery (18, 9.1%), arson (18, 9.1%) and assault (12, 6.1%). With regards to prior criminal history, 108 (54.8%) had no previous convictions, whereas 18 (9.1%) had a previous conviction for a serious violent offence and 29 (14.7%) had served a term of imprisonment prior to the index offence (Table 2).
Demographic features of released forensic patients (n = 197).
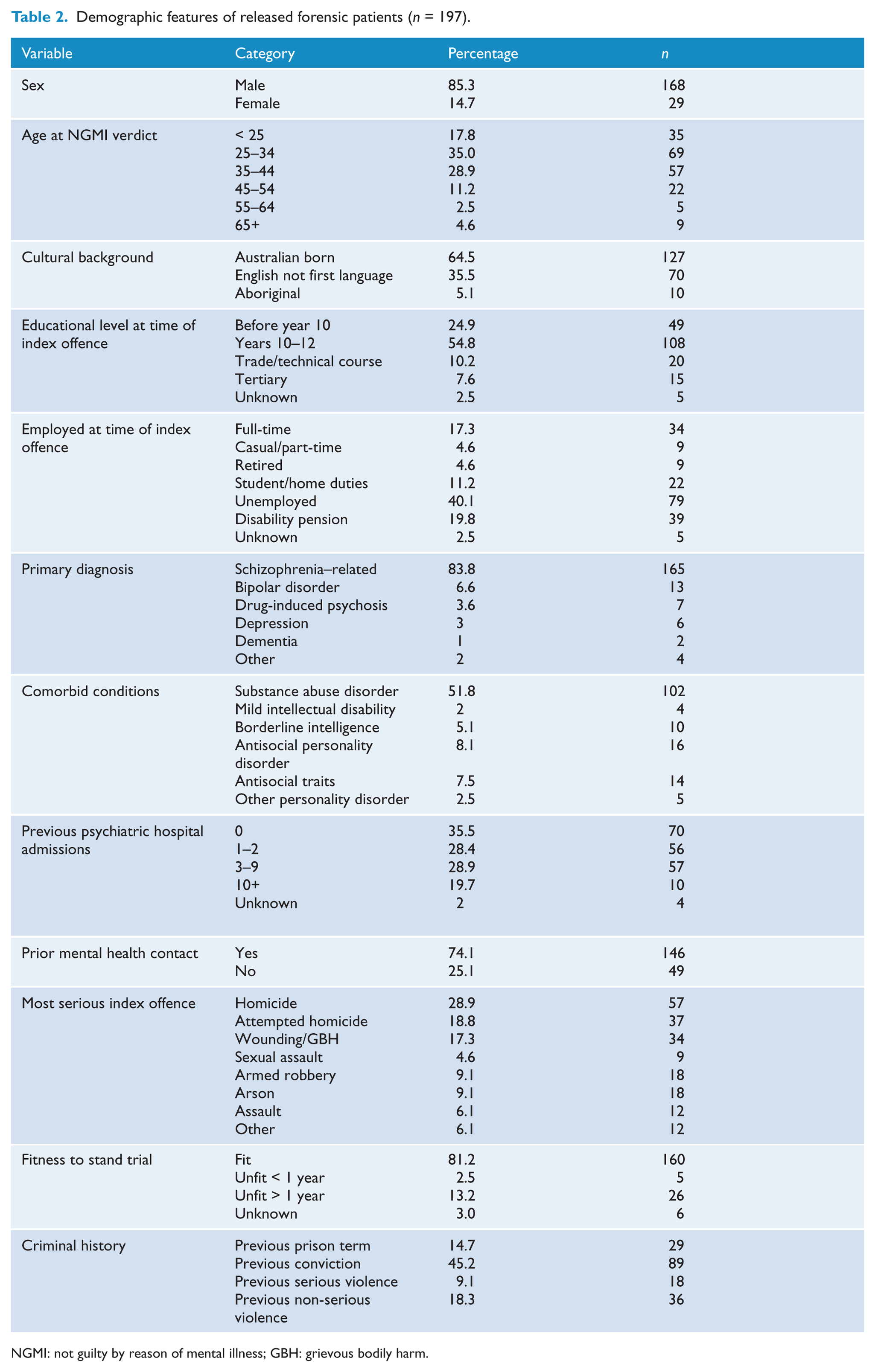
NGMI: not guilty by reason of mental illness; GBH: grievous bodily harm.
Readmission to hospital
The MHRT files did not include sufficient information to establish whether there had been a further hospital admission in 28 of the 186 patients granted a period of conditional release. Moreover, the treatment reports provided to the MHRT did not consistently include the actual dates of hospital admission or discharge, nor the duration of hospital stays. Hence, there was insufficient data in the case files to reliably calculate survival curves for the period from release to rehospitalisation.
Following their conditional release into the community, 76 of the remaining 158 patients (48.1%) were readmitted to a psychiatric facility, 32 (20.3%) once, 27 (17.1%) twice, seven (4.4%) three times and 10 (6.3%) on four or more occasions. Although most admissions were to treat relapses of mental illness or to adjust medication, there were some admissions that were initiated by the treating teams or the patients themselves in order to prevent relapse. Further analyses were conducted to determine variables associated with forensic patients’ readmission to hospital (see Supplemental Tables 1 and 2).
Information about hospital admissions after unconditional release was not available because these individuals were no longer under the supervision of the MHRT and the absence of a state-wide system for recording psychiatric hospital readmissions prohibited linkage of useful data.
Revocation of conditional release
One case, from the total of 186 patients who were granted conditional release, was excluded from the analysis due to missing data (including date of the order). About a quarter (48/185) of forensic patients had their conditional release revoked: 33 (17.8%) on one occasion, 11 (5.9%) twice, three (1.6%) three times, and one patient had his conditional release revoked on four occasions during the period of this study.
A survival analysis was conducted on the 185 patients who were granted conditional release to determine how long they remained in the community until the revocation of their conditional release, death or the census date (Figure 2). After 6 months about 92% of the sample remained in the community, after 12 months 87%, at 2 years 83% and at 5 years 74% were still in the community. The proportion still in the community after 5 years appeared to stabilise at about 70% of all released patients. Only 10.8% (8/74) of the patients who had been granted unconditional release had their conditional release revoked prior to being granted unconditional release: six patients (8.1%) once and two patients (2.7%) twice.
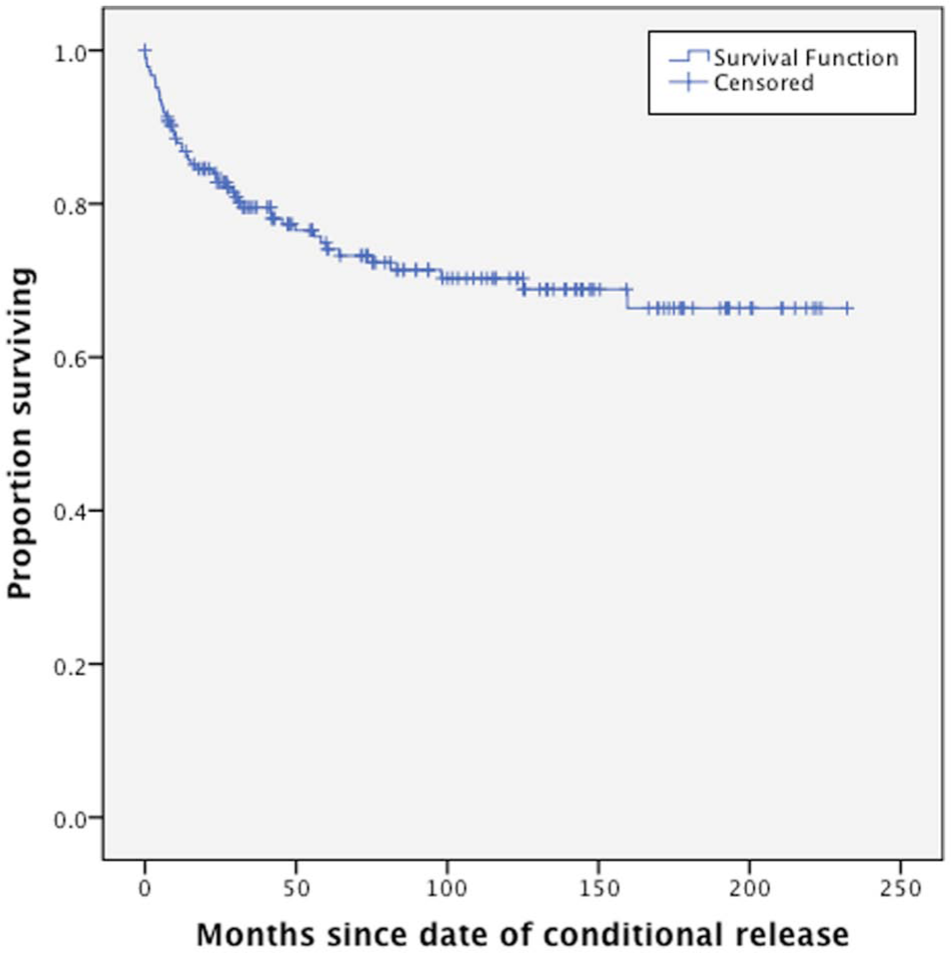
The proportion of forensic patients surviving over time (months) in the community following their conditional release.
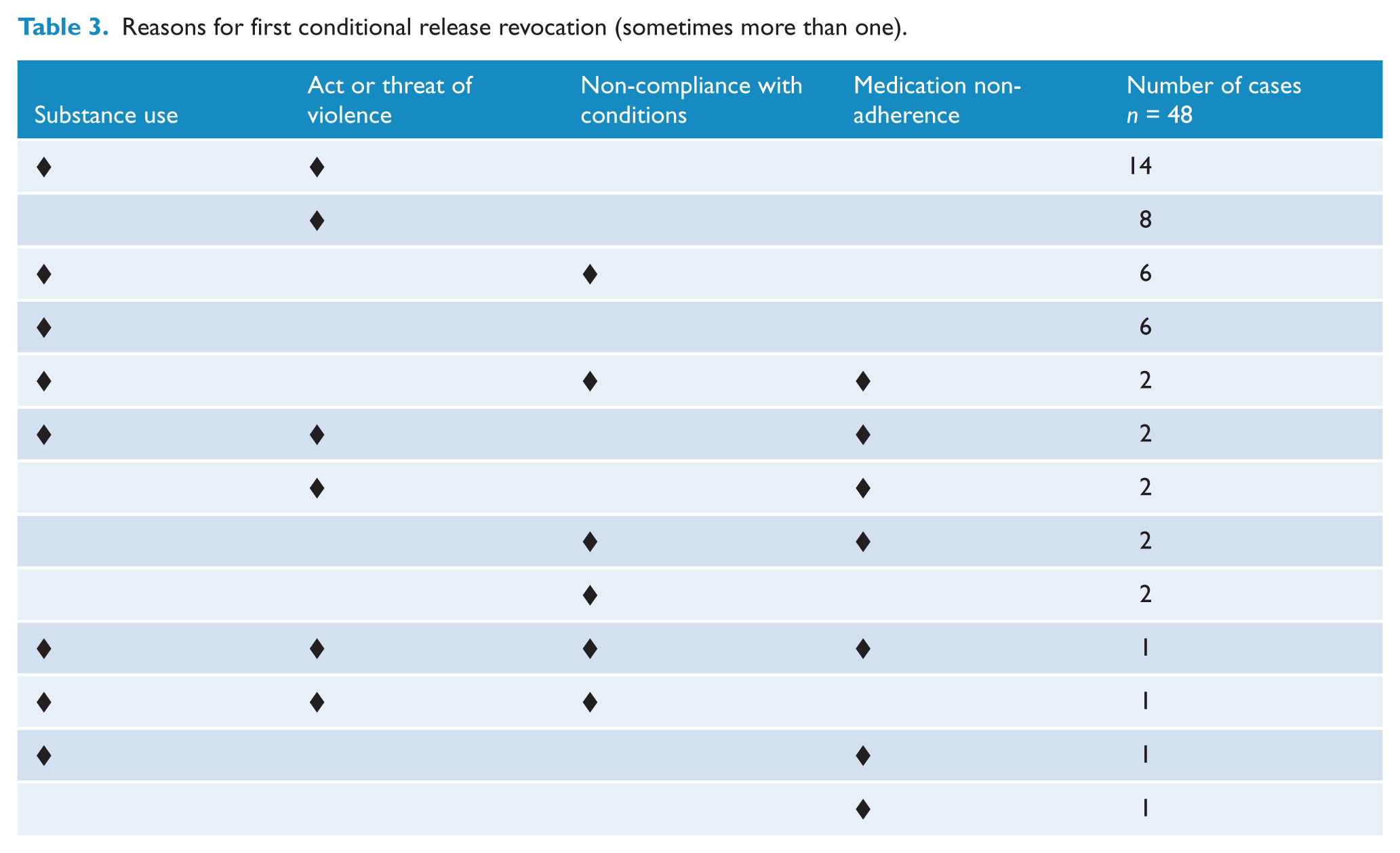
Conditional release was often revoked for breaching more than one of a list of conditions (Table 3). The most common reason for revocation was substance misuse (68.8%, 33/48), followed by an act or threat of violence (58.3%, 28/48). About 23% (11/48) of cases involved non-adherence to medication and 29.1% (14/48) non-compliance with other conditions of release, including 16.7% (8/48) who were deemed to be absent from their approved accommodation without leave. Conditional release was revoked for breaching conditions of release rather than relapses of mental illness, which were usually dealt with by admission to hospital without the revocation of conditional release.
Reasons for first conditional release revocation (sometimes more than one).
Further analyses were performed to determine which factors were associated with conditional release revocation and are reported in the Supplemental Data (see Supplemental Tables 3 and 4).
Reoffending after conditional release
Of the 186 patients ever granted conditional release, 22 received a NGMI verdict before 1994, one had an unknown conditional release date, and two were repatriated to another jurisdiction. Thus, 25 cases were excluded from the analysis of reoffending, with 161 remaining cases.
During their period of conditional release, 18% (29/161) of forensic patients, with verdicts during or after 1994, were charged with a further criminal offence, and 11.8% (19) were convicted of an offence. The average time at liberty was 101 months (median=99 months, range 7–229 months). The median time between the date of conditional release and date of first offence was 48.1 months and mean was 45.2 months (range 1.6–155.7 months).
A survival analysis was conducted of months from conditional release until the recorded date of first criminal charge, census date or death (Figure 3). After 6 months about 97% of forensic patients had not been charged with any offence, and the proportion was 94% at 12 months, 91% at 2 years and 84% at 5 years.
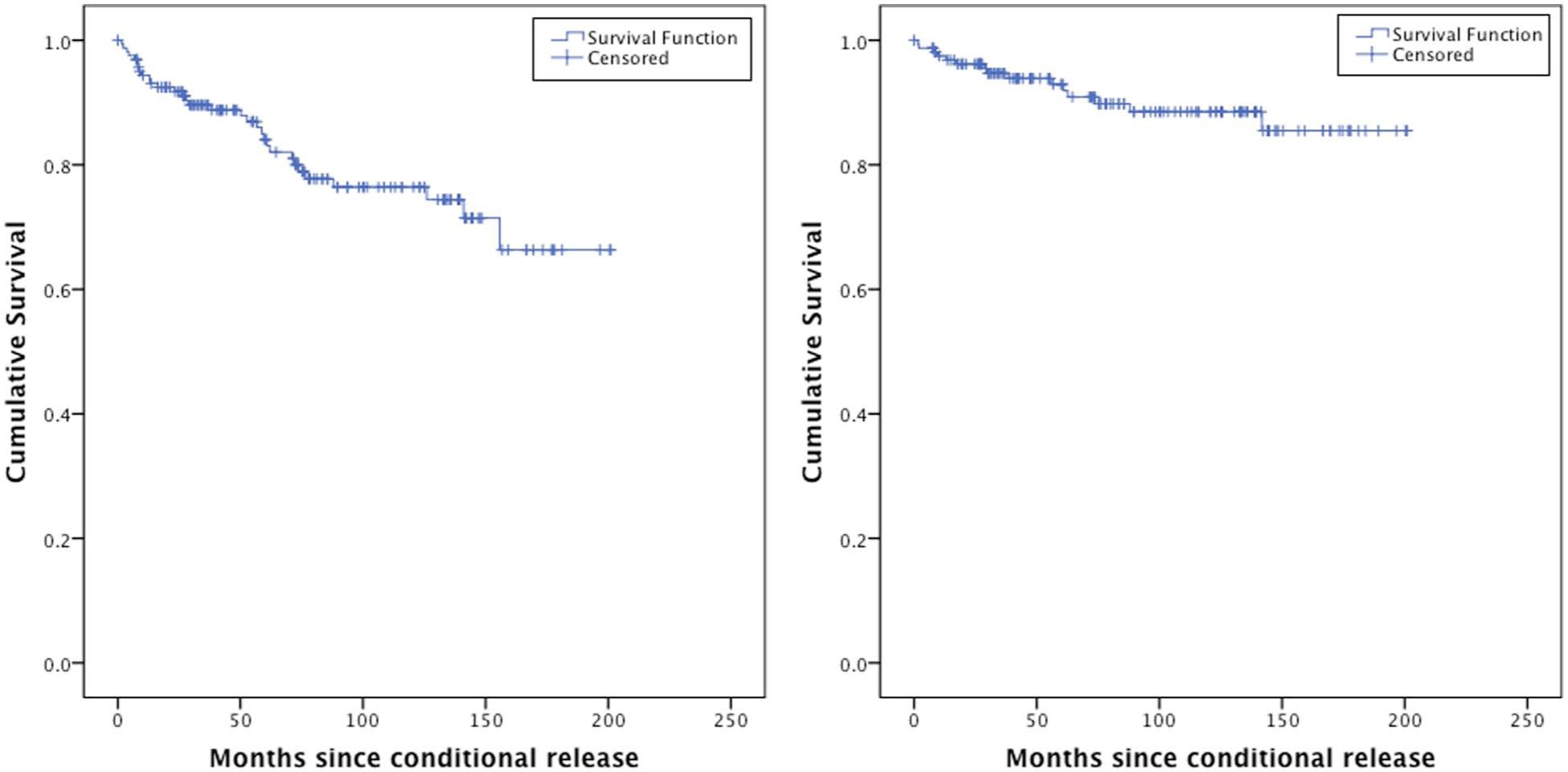
Time to first charge (left panel) or time to first charge for a violent offence (right panel) following conditional release after 1994.
Eleven patients were charged with one offence and three were charged for four or more offences. The majority of ‘most serious offences recorded’ were non-violent traffic offences. Further analyses were conducted to test factors hypothesised to predict reoffending after conditional release and the results are reported in the Supplemental Data (see Supplemental Tables 5 and 6).
Violent reoffending during conditional release
Fourteen of 161 conditionally released patients (8.7%) were charged with a violent offence, and five (3.1%) were convicted. The offences included homicide (1), attempted homicide (1), assault (10) and sexual assault (2). One patient had their violent charge withdrawn, 12 patients had their conditional release revoked as a result of their offending and four received a second NGMI verdict. Of those convicted of violent offences, five received a prison term, one received a suspended sentence and one was placed on a good behaviour bond.
The median time between the date of conditional release and date of recorded violent offence was 30 months and the mean was 42 months (range 2–142 months, SD=39).
In the survival analysis, 1% of forensic patients had recorded a violent offence at 6 months, 3% at 12 months, 4% at 2 years and 7% at 5 years after their conditional release (Figure 3).
Further analyses were conducted to determine factors that could predict violent reoffending during the period of conditional release (see Supplemental Table 7).
Reoffending after unconditional release
Of the 85 patients granted unconditional release, 16 received NGMI verdicts prior to 1994, so were excluded from the analysis of reoffending. A further five patients were excluded because they had been repatriated to another jurisdiction. The average length of follow-up was 91 months (range 7–194 months). The median time between the date of unconditional release and first recorded offence after discharge was 55 months and the mean was 70 months (range 3–175 months).
Eight of the 64 former forensic patients (12.5%) were charged with further offences: two recorded more than five offences and the other six recorded less than three offences. Three people were charged with minor offences (disturbing public order and traffic offences), one for a drug-related offence and four (6.3%) with violent offences, the most serious being assault. Six people (9.4%) received convictions: three (4.7%) for assault and the others for traffic and minor non-violent offences. None of those convictions resulted in a prison sentence and none of the unconditionally released patients received a further NGMI verdict (Table 4). The penalties included community service orders (one case), good behaviour bonds (two cases) and fines (three cases), and two convictions with no penalty.
Summary of reoffending by released forensic patients a .
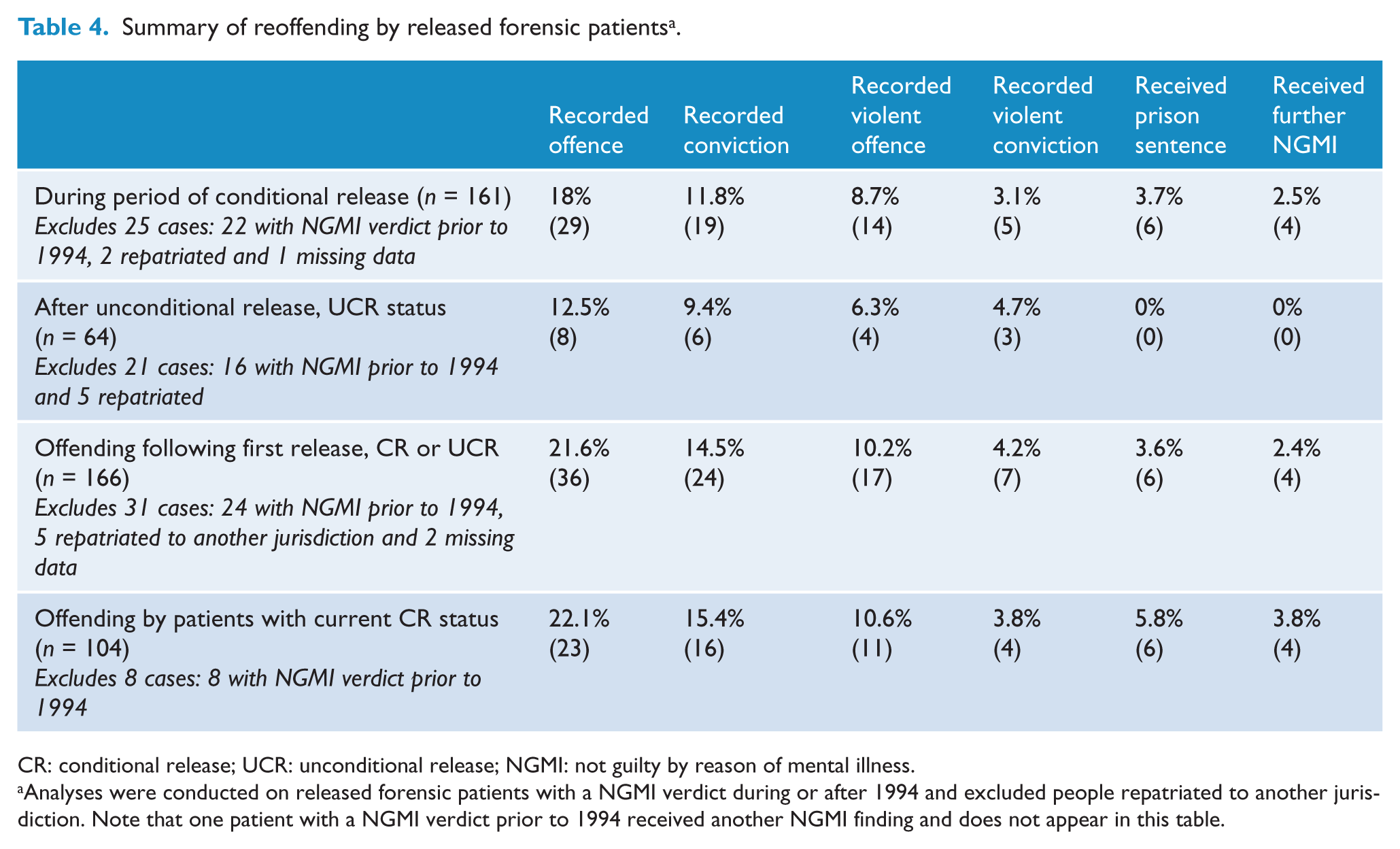
CR: conditional release; UCR: unconditional release; NGMI: not guilty by reason of mental illness.
Analyses were conducted on released forensic patients with a NGMI verdict during or after 1994 and excluded people repatriated to another jurisdiction. Note that one patient with a NGMI verdict prior to 1994 received another NGMI finding and does not appear in this table.
Fisher’s exact tests were used to analyse factors hypothesised to predict reoffending and violent reoffending after conditional release and the results appear in Supplemental Table 8.
Location of conditionally released patients at Census
On the census date (31 July 2011), 65.2% (73/112) of the patients with a conditional release status were living in the community, including five in a supervised home, three in an aged care facility and one living independently in another state. Twenty-six percent (29/112) were in psychiatric hospital wards and 3% (3/112) were detained in a correctional centre. Five patients had died and two patients were absent without leave.
Discussion
Overview
An NGMI verdict was reached in less than 1% of matters dealt with in the higher courts in NSW from 1990 to 2010, despite a lower threshold for NGMI verdicts in NSW compared to other jurisdictions (Nielssen et al., 2011). An NGMI verdict allows for indefinite detention in a secure hospital; however, in the 21 years since the formation of the MHRT, 197 (54%) NGMI forensic patients have been released into the community, including 85 (23.4%) who were released unconditionally. The main findings of this study are that although almost half of forensic patients were readmitted to hospital after conditional release, about one-quarter had their conditional release revoked, and the reoffending rate by released forensic patients is reassuringly low.
Hospital readmissions
In a period of follow-up that was on average more than 8 years, almost 50% of conditionally released patients were readmitted to hospital at some stage. It is difficult to compare this result with studies from other jurisdictions with different forms of treatment and supervision after release, variable thresholds for hospital admission and different follow-up periods. However, this rate would appear lower than the few studies reported elsewhere (Table 1). In this study, patients were significantly more likely to be rehospitalised if they had residual symptoms at the time of conditional release and/or had a history of substance abuse. These findings are not surprising given the chronic nature of mental illness in this sample and also the negative impact of substance abuse on mental illness.
Rehospitalisation is not necessarily an indication of treatment failure, as most forensic patients have chronic mental illness and further episodes of illness requiring hospital treatment would be expected. Furthermore, readmission rates are directly affected by how closely the mental state of released forensic patients is monitored in the community together with a lower threshold for hospital readmission. Although lower rehospitalisation rates are seen as a positive outcome measure, for forensic patients admission to hospital is preferable to arrest (Kravitz and Kelly, 1999).
Some authors have suggested including rehospitalisation in recidivism data, on the basis that many forensic patients are readmitted for breaches of conditions of release that might constitute a criminal offence (Kravitz and Kelly, 1999). However, in this sample, most hospital readmissions were to prevent or treat relapses and were not directly related to violence or criminal behaviour. It has been argued that close supervision after release and low threshold for hospital readmission can reduce reoffending (Rolfe, 2001) and the low rate of reoffending observed in this sample could in part be due to close monitoring of mental state and early rehospitalisation.
Revocation of conditional release
A quarter of forensic patients had their conditional release revoked, which is less than rates reported in other studies (Table 1). Half of all revocations occurred within the first 12 months after conditional release, and most occurred within the first 2 years after release; there were relatively few revocations after 5 years of conditional release. This suggests that problems usually emerge within the first 2 years of conditional release and that in most instances 5 years would be a reasonable period of supervision before considering unconditional release.
The most common reasons for revoking conditional release were breaches of conditions by substance use and acts or threats of violence. In several cases, the revocation was in response to the return of patterns of behaviour that were considered to be similar to those leading to the original offence, and the decision to revoke conditional release was made as a preventative measure. The early revocation of conditional release for forensic patients who do not comply with their release conditions is also likely to have contributed to the relatively low rate of offending in this sample.
This study found that forensic patients were less likely to have their conditional release revoked if they were over 35 years old and/or employed at the time of conditional release. Additional, but not independent, risk factors associated with revocation included being Aboriginal, having a history of substance or poly-substance abuse, and the presence of criminogenic factors (such as early age of first offence, antisocial traits, prior conviction and previous incarceration). These are similar to risk factors associated with reoffending in this and other studies (Baxter et al., 1999; Buchanan, 1998; Rice et al., 1990; Tellefsen et al., 1992). Patients who spent time in a medium-security hospital were less likely to have their conditional release revoked, which suggests that gradual progression through the forensic mental health system may better prepare patients for conditional release.
Reoffending
There was a reassuringly low incidence of criminal charges (18%), convictions (11.8%), convictions for violent offences (3.1%) and imprisonment (3.7%) among conditionally released forensic patients in NSW, over an average period of follow-up of more than 8 years. However, there were five instances of serious violence by patients who had been granted conditional release, including one homicide. The reoffending rate of NSW forensic patients is considerably lower than those reported by similar services overseas (Jamieson and Taylor, 2004; Livingston et al., 2003; Rice et al., 1990; Skipworth et al., 2006). The overall reoffending rate and the violent reoffending rate in this study are similar to the rates reported by Luettgen et al. (1998). Luettgen and associates attributed the low rate in their study to preventative hospitalisations, with 86.5% of their sample readmitted to hospital compared to 50% in this study. A violent conviction rate of 6% at 2 years was reported by Skipworth et al. (2006), which they attributed to cautious decisions regarding release. The present finding, of less than 5% violent reconviction at an average of more than 8 years, would suggest that the MHRT operates conservatively in its recommendations to release forensic patients into the community.
Limitations
This research has limitations common to retrospective research. Forensic patients are a small, complex and heterogeneous group and do not follow an orderly, predictable pathway from verdict to release into the community. Furthermore, cases were examined over a 21-year period and thus were subject to changes in the law, MHRT procedures and facilities for treatment of forensic patients. The use of archival case files meant that some data were reported inconsistently or were missing. The study was further hindered by the absence of centralised and integrated information systems to track the movement of patients between hospitals, community or corrective services. For instance, NSW hospital admission data have only become available since 2000, which meant that survival time in the community prior to rehospitalisation could not be measured. Reoffending data were available from BOCSAR only after 1994 and there appeared to be some inconsistencies of recording in the early years, and the data are limited to offences in NSW.
Another limitation of this study is that it did not compare forensic patients to a control group; for example, convicted offenders with similar psychiatric disorders. Although as many as 7% of prisoners in NSW have schizophrenia (Nielssen and Misrachi, 2005) and about 10% of violent offenders have a diagnosed psychotic illness (Yee et al., 2011), there is currently no available data on their rates of recidivism. The reported rates of recidivism and breaches of parole conditions for NSW prisoners suggest the outcome for NGMI forensic patients is considerably better, as 60% of adults convicted of an offence in NSW in 1994 were convicted of a further offence within 15 years, 66% of people released on parole in NSW were charged with a further offence within 3 years, and 40% of prisoners across Australia were reimprisoned within 10 years of release (ABS, 2010; Holmes, 2011; Jones et al., 2006). A comparison with the recidivism rates of non-mentally ill offenders was not possible because the available data on reconviction in NSW does not include more severe offences (such as homicide and attempted homicide) that were more typical of offences committed by the forensic patients (Holmes, 2011). Moreover, although the literature reports that recidivism rates for insanity acquittees are comparable to recidivism rates in convicted prisoners (Caffrey, 2005), the current study suggests lower levels for forensic patients. Reasons for this lower rate of recidivism among released forensic patients in this study, compared to prison cohorts, might include their lower rates of substance dependence, antisocial personality traits, family dysfunction and past criminal conviction (Butler et al., 2006).
The low rate of reoffending might also be due to the success of treatment and rehabilitation provided by the forensic mental health system, which includes a high level of supervision and support after release into the community. Given the direct relationship between the acute symptoms of mental illness and the index offence for this sample, it is probable that continuous treatment reduced the likelihood of released patients committing further serious offences. The effect of the course of illness on the propensity to commit further offences could also be relevant, as a large proportion of the forensic patients committed their offences prior to initial treatment (Nielssen et al., 2011), and the negative symptoms of more chronic forms of illness may be protective against further violence (Torrey et al., 2008). The observation that forensic patients achieve better outcomes than mentally disordered prisoners has important implications for the way treatment and continuing supervision is provided to mentally disordered prisoners after release.
Factors that predict reoffending
The current study offers tentative support that the success of the forensic mental health system is due to a model that represents gradual progression through the forensic system to treatment in community settings. For example, patients who spent time in medium-security hospitals and were granted unsupervised day and unsupervised overnight leave privileges were less likely to reoffend than those who followed different pathways.
Potential risk factors of recidivism were analysed for this population. As with earlier studies, factors such as being indigenous, less than 25 years old at the time of their first offence, having a diagnosed substance abuse disorder, having a diagnosis consistent with antisocial personality disorder, prior imprisonment, previous convictions and being unemployed at the time of conditional release were all significantly related to reoffending post-release (Baxter et al., 1999; Buchanan, 1998; Coid et al., 2007; Skipworth et al., 2006). Although models that included these factors in analyses could predict reoffending with over 85% success, they were of limited value in predicting which specific patients were likely to reoffend. Furthermore, the low rate of convictions after unconditional release precluded any meaningful analysis of factors associated with recidivism.
Decision-making process
Over the last 20 years, actuarial tools (such as the HCR-20) have been increasingly used to estimate the probability of further violence (Buchanan, 2008), although there is some controversy about the value of incorporating actuarial risk assessment results into the process of deciding on the release of individual patients (Hilton and Simmons, 2001; Large et al., 2011; Manguno-Mire, 2007). Although risk assessment reports were available from the files of about half of the patients in this sample, it could not be determined how these were used by the MHRT to influence their decisions to release. Future research could examine the process by which the MHRT reaches its decisions and whether information from risk assessments is helpful in further reducing the rates of reoffending and the more rational use of forensic service resources.
Another important finding is the lower rates of reoffending, including for less severe offences, recorded for unconditionally released forensic patients compared to rates after conditional release. This indicates that the conditional release process might be contributing to reducing reoffending rates. Furthermore, it suggests that the MHRT was successful in identifying patients who were likely to do well and to make appropriate recommendations regarding unconditional release. This finding supports the legislative change that came into effect in 2009 granting the MHRT the power to make unconditional release orders (Mental Health Act, 2007).
Conclusions
This study found that reoffending by forensic patients released into the community in NSW is low and that none of the patients who were granted unconditional release in the last 20 years went on to commit a further serious offence. A large proportion were readmitted to hospital and a significant proportion had their conditional release revoked at least once, which suggests that early intervention in the event of relapse of mental illness and non-compliance with conditions of release prevented reoffending. The results of this study provide a strong endorsement of the treatment and rehabilitation of forensic patients in NSW, and the decision-making process of the MHRT.
Footnotes
Acknowledgements
The authors would like to thank Sarah Hanson and John Feneley of the NSW Mental Health Tribunal, and the NSW Bureau of Crime Statistics and Research for their assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.