
Abstract

The diagnosis of schizoaffective disorder survives in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) (American Psychiatric Association, 2013), despite persuasive exhortations for its removal (Maier, 2006; Malhi et al., 2008). However, its classification has been modified and the DSM-5 authors assert that they have implemented changes to improve both the reliability and the stability of this diagnosis. This prompts a number of questions, including: Is this the correct approach? And will it improve clinical practice?
The creation of schizoaffective disorder
It is perhaps useful to go back and take a brief look over the history of this problematic diagnosis. Kasanin first coined the term ‘schizoaffective disorder’ in 1933, framing it essentially as a reactive psychosis (Kasanin, 1933; Stromgren, 1974), where there is a clear contextual stressor and ultimately a better outcome than is usually associated with a diagnosis of schizophrenia. In the DSM, the purpose of creating a diagnosis of schizoaffective disorder was simply pragmatic: it enabled clinicians to assign a diagnosis to clinical cases that were otherwise difficult to define accurately using diagnoses within affective disorders and schizophrenia. This situation was partly a consequence of the prevailing zeitgeist in which the Kraepelinian dichotomy (Kraepelin, 1919) was the dominant driver. Kraepelin separated schizophrenia and affective disorders on the basis of psychopathology and clinical trajectory. Specifically, he defined dementia praecox (schizophrenia) as a disease of the brain and distinguished this from manic-depressive insanity (psychotic mood disorders) partly on the basis of inter-episode recovery. The latter, along with a better outcome, was thought to be more probable in psychoses associated with mania or depression; by contrast, in schizophrenia, in addition to cognitive deterioration and diminished emotional expression, individuals were generally destined to fare worse.
This model was widely adopted and, clinically, there is no doubt that some psychotic presentations have clear-cut symptoms of schizophrenia and others have clearly defined symptoms of an affective disorder. However, equally, and indeed perhaps in the majority of cases, there are presentations characterised by overlapping symptoms, which are either contiguous or coterminous. Such temporal continuity and/or simultaneity cannot be accommodated in the dichotomous model (Craddock and Owen, 2010).
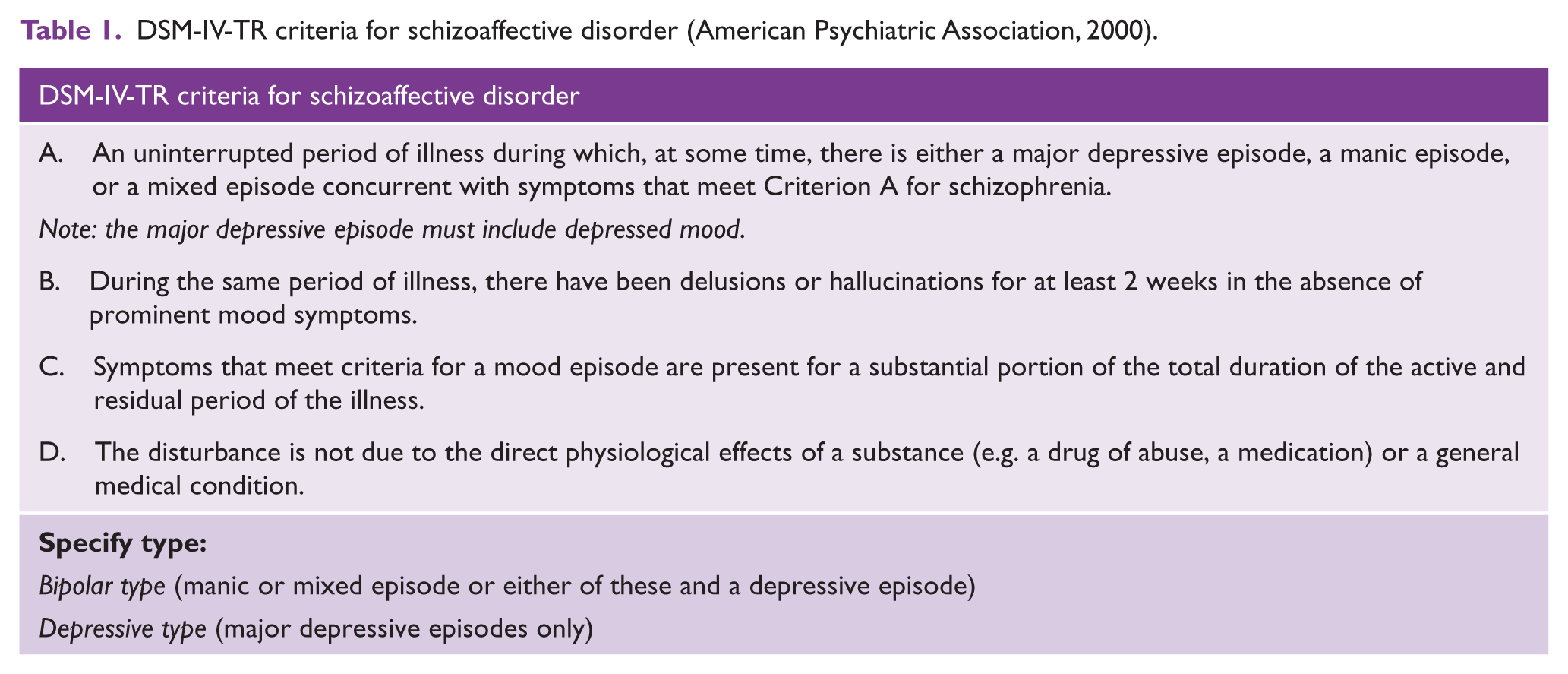
The diagnosis of schizoaffective disorder was introduced in DSM-III (American Psychiatric Association, 1980) and, remarkably, at the time it was the only diagnosis in the manual that lacked specific operational criteria (Tandon, 2012). Indeed, it was not until 1987, with the development of DSM-III-R (American Psychiatric Association, 1987), that diagnostic criteria for schizoaffective disorder were explicitly operationalised. The latter involved the introduction of four criteria (Table 1), which have remained relatively unchanged for over a quarter of a century, until now.
DSM-IV-TR criteria for schizoaffective disorder (American Psychiatric Association, 2000).
Early editions of the DSM used the term ‘schizo-affective type’ to describe a form of ‘schizophrenic reaction’, which could be further partitioned into excited and depressed subtypes. Together these terms were used to describe varying admixtures of symptoms that stemmed from those of schizophrenia and affective disorders. Usually the symptoms of schizophrenia were assigned greater importance because of a fundamental assumption that all these manifestations eventually tend towards schizophrenia. However, the terms could also be applied to affective states in which schizophrenia-like symptoms occurred.
Another reason for the creation of the ‘category’ of schizoaffective disorder was to better understand the nature of psychoses. The belief was that this would be achieved by better definition, which in turn would lead to identification of its determinants and the development of better and more specific treatments. However, since its introduction, schizoaffective disorder has proven to be a problematic diagnosis and one that has provided little insight into the pathophysiology of psychotic disorders. Instead, it has most likely generated confusion with respect to epidemiological and clinical data. Both from aetiological and pathological perspectives, the crux of the issue (which schizoaffective disorder highlights) is whether it reflects an interaction between affective disorders and schizophrenia that arises by virtue of overlap between disorders, or whether it represents a separate entity unto itself.
Clinically, cohorts with schizoaffective disorder exist on a continuum in between the affective psychoses and schizophrenia. Recent research convincingly points to the commonalities between psychotic affective disorders such as bipolar disorder and schizophrenia (Cardno et al., 2002). This supports the notion that functional psychoses exist along a spectrum, and that the myriad clinical manifestations are best captured dimensionally so as to better understand the underpinning neurobiology. In other words, there are no true categories per se and diagnoses are more a matter of degree than absolutes. Where does this leave us with schizoaffective disorder?
From made up to make up?
As briefly outlined above, research supporting a diagnostic category of schizoaffective disorder is weak at best. Clinically, the reliability (Faraone et al., 1996) and consistency (Nurnberger et al., 1994) of the diagnosis has been shown to be extremely poor. In clinical populations, just over a third of patients diagnosed with schizoaffective disorder maintain the diagnosis over a period of 6 months to 2 years (Schwartz et al., 2000). Part of the reason for this is that in real-world practice the criteria used to first assign the diagnosis of schizoaffective disorder are loosely interpreted and variably applied, resulting in a lack of consistency (Vollmer-Larsen, 2006).
Why then has DSM-5 persisted with the diagnosis of schizoaffective disorder? An alternative proposal that was apparently considered but deemed to be unviable because of insufficient data (Malaspina et al., 2013) was to replace schizoaffective disorder with the inclusion of specifiers based on dimensions of mood symptoms, which could be used in conjunction with diagnoses of schizophrenia and/or schizophreniform disorders. Admittedly this option is not without its own limitations (e.g. it is not clear whether this can be achieved with a high degree of reliability) and it has the potential to generate new problems (e.g. new combinations of specifiers may create further subtypes and increase heterogeneity further). However, retaining the diagnosis without much improvement is equally puzzling. Perhaps it is yet another example of the conservative approach adopted by DSM-5 (Malhi, 2013).
The new criteria for schizoaffective disorder in DSM-5 are listed in Table 2; in essence, they require the overlap of mood symptoms with psychotic symptoms to be conspicuous and stipulate that this should occur for a greater proportion of time. Specifying the criteria more clearly in this manner is likely to enhance the reliability of the diagnosis, but possibly only in research settings. Its impact on clinical practice remains doubtful, given that currently the label schizoaffective disorder often reflects diagnostic uncertainty and is sometimes exploited to either defer a diagnosis of schizophrenia or to facilitate access to neuroleptic treatment options.
DSM-5 diagnostic criteria for schizoaffective disorder (American Psychiatric Association, 2013).

If schizoaffective is not so effective?
Returning to the questions posed at the outset, it has been argued (Malhi et al., 2008) that the concept of schizoaffective disorder has been given sufficient opportunity to establish a foundation and that simply refining the diagnostic criteria is unlikely to advance our understanding. This is because clinical phenomenology is too far removed and perhaps too loosely coupled with underlying neurobiological processes to meaningfully inform the putative nature of psychiatric diseases, especially if used in isolation. Bridging this divide between molecular understanding and clinical symptomatology remains a significant challenge, which is compounded by the absence of a definitive diagnosis. In this regard, the DSM endeavour has moved, although, almost imperceptibly, in the correct direction, but the change is likely to be ineffectual. Instead, the broad and inconsistent use of the ‘category’ of schizoaffective disorder is likely to continue to generate confusing and possibly misleading data.
Now that DSM-5 is a reality, the only hope of a significant change in thinking, and thereby practice, is if the International Classification of Diseases, 11th Revision (ICD-11) actively decides not to follow suit and, instead, dispenses with schizoaffective disorder altogether, or at least restricts its use to research only. Arguably, the use of loosely defined DSM criteria for schizoaffective disorder for over three decades has been of no discernible benefit to patients, nor indeed have doctors gained valuable insights. Perhaps only pharmaceutical companies have profited from the clinical ambiguity the diagnosis of schizoaffective disorder has conferred.
Simply tweaking the criteria, as has been done in DSM-5, is unlikely to dramatically advance our understanding, but if ICD-11 took a bold stance and, instead of vague clinical criteria, provided specific research guidance to carefully investigate the overlap of affective and psychotic symptom presentations, then at least future research would be more targeted. For example, to identify the complex pathophysiology, which likely underpins the variegated clinical manifestations of psychoses with and without mood symptoms, using neurobiological probes, requires tightly defined pristine clinical groupings. And only by examining operationalized phenotypes, and doing so concurrently, so that comparative data can be derived, are we likely to glimpse the mechanisms and processes that drive clinical phenomenology. Ultimately, as a clear neurobiology of the affective psychoses and schizophrenia emerges, the ‘make up’ of schizoaffective disorder will fade and the extent to which it has been a ‘made up’ diagnosis will become apparent.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper.