
Abstract

The review by Fergusson and colleagues (2013) of the relationship between abortion (versus delivery of an unintended or unwanted pregnancy) and mental health does not inform policies that authorize abortion on the grounds that continuing the pregnancy would pose a serious threat to women’s mental health. Moreover, it was inappropriate to conduct a meta-analysis of the abortion and mental health literature, particularly given that there were only two to three studies used for each mental health outcome.
Review does not inform policies that authorize abortion on mental health grounds
Fergusson et al. (2013) state that: In these societies [England, Wales, Scotland, and New Zealand] over 90% of all abortions are currently authorized on the grounds that continuation of the pregnancy would pose a serious threat to the woman’s mental health … Given the high frequency with which mental health grounds are used in these jurisdictions to authorize abortion, it becomes important for both clinical and legislative reasons to examine the evidence on the extent to which abortion has therapeutic benefits that mitigate any mental health effects of unwanted pregnancy.
In order to determine whether these policies are grounded in the scientific evidence, studies need to test whether abortion reduces women’s mental health risks.
The question then becomes how to test whether abortion reduces women’s mental health risks to inform these policies. Here I discuss two study designs that test this and argue that the design used by Fergusson and colleagues is inadequate. It is not entirely clear what Fergusson and colleagues’ ideal randomized control trial would be. Nevertheless, given the review they conducted, it seems Fergusson and colleagues argue the ideal experiment would randomize women having unwanted or unintended pregnancies either to have an abortion or not and measure post-pregnancy mental health. However, randomly assigning all women with unwanted or unintended pregnancies would not inform the aforementioned policies because women having unwanted or unintended pregnancies and choosing not to seek abortions are likely very different from women seeking abortions for mental health reasons. For instance, women seeking abortions for mental health reasons may have higher rates of pre-existing mental health problems or be living in socially disadvantaged circumstances compared to women having unintended or unwanted pregnancies and not seeking abortions. Instead, the ideal randomized control trial is to randomize women seeking abortions for mental health reasons to have an abortion or to not have one.
While it is not ethical to randomize either women having unwanted or unintended pregnancies or women seeking abortions, understanding what the ideal experimental design is allows us to see what the best non-experimental study would be to inform these policies. Such a study would not compare women who have abortions with women who have unwanted or unintended pregnancies but do not even seek abortions, as Fergusson and colleagues do in their review. Rather, one appropriate design would compare women who obtain abortions because continuing the pregnancy would hurt their mental health to women who are seeking abortions on similar grounds but are denied one. To my knowledge no such study has been conducted. One study that comes closest to this was conducted by Gilchrist and colleagues, who compared women who abort to women who sought an abortion but were denied one (Gilchrist et al., 1995). This study found that among those with no history of psychiatric illness, the rates of any psychiatric illness, non-psychotic illnesses, and self-injury did not differ between women denied an abortion and women who obtained an abortion. However, rates of psychotic illness were higher in women denied an abortion compared to women who obtained an abortion. Among women with histories of psychiatric problems, those who obtained an abortion did not have higher rates of any subsequent psychiatric illnesses compared to women who sought an abortion but were denied one. Together, these results suggest that for some women, abortion reduces women’s risk of some serious psychological disorders—psychotic disorders—and that abortion does not increase women’s risk of mental health problems.
An alternative study design would be to compare women’s mental health pre- and post-abortion. To find scientific support for policies authorizing abortions for mental health reasons, women’s mental health after an abortion would need to be better than or equal to that before an abortion. Some past studies have done this comparison, and they have found that depressive and anxiety symptoms decreased from pre- to post-abortion (Cozzarelli, 1993; Lowenstein et al., 2006; Major et al., 2000; Slade et al., 1998; Zabin et al., 1989). Moreover, self-esteem has been found to increase from pre- to post-abortion (Major et al., 2000; Zabin et al., 1989). Together, these findings support policies that justify abortions on mental health grounds because women’s mental health improved from pre- to post-abortion.
Both of the study designs discussed here provide a different angle for answering whether policies granting abortions for mental health reasons are supported in scientific evidence. As depicted in Figure 1, using two possible scenarios, women’s mental health symptoms may decrease from pre- to post-abortion (Figure 1a) and still remain above women who sought an abortion but were denied one. Alternatively, women’s mental health symptoms may increase from pre- to post-abortion (Figure 1b), but this increase may occur at a slower rate than among women who delivered a pregnancy because they were denied an abortion. In both scenarios, women’s mental health after an abortion is better than a comparison group. In the first example, women’s mental health after an abortion has improved relative to that before the abortion. In the second, women’s mental health after an abortion is better than women’s mental health after being denied an abortion. The best study design would combine elements from both of these methods, examining women’s mental health before seeking an abortion and after receiving versus being denied an abortion.
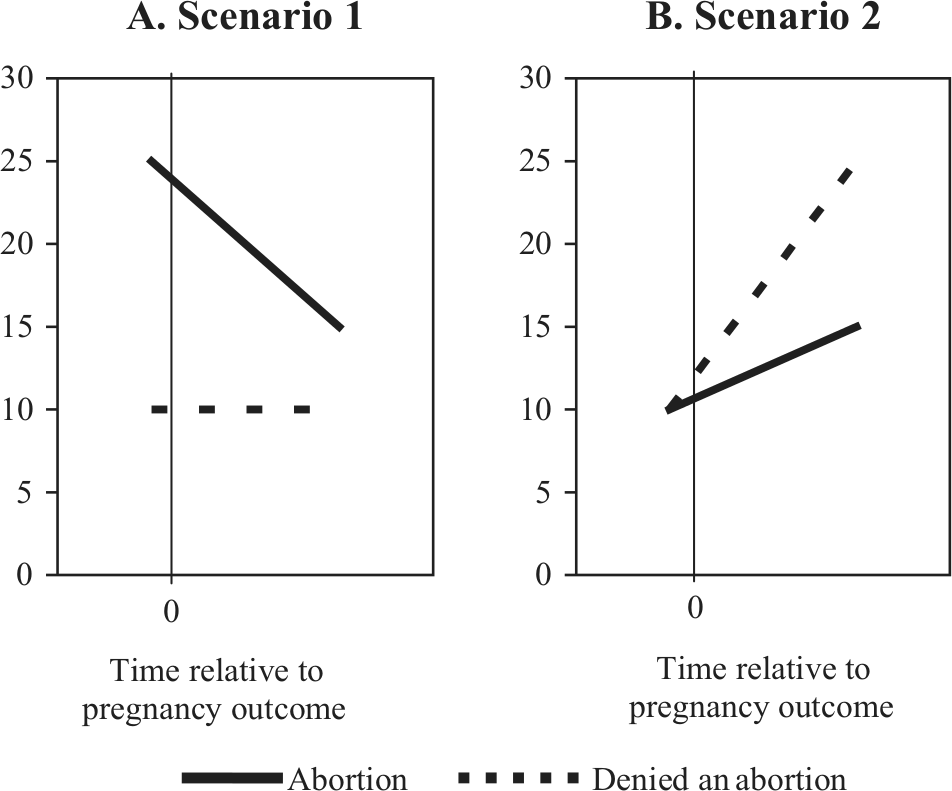
Two examples of how women’s mental health could change from pre- to post-abortion compared with women who were denied an abortion. Notes. 0 is when the pregnancy outcome occurred. Before 0 is before obtaining an abortion or childbirth. Scenario 1 indicates that abortion improves women’s mental health from beforehand to afterwards, even though post-abortion women’s mental health symptoms are still higher than post-being denied an abortion. Scenario 2 illustrates that relative to women denied an abortion, women who obtained an abortion had lower mental health symptoms afterwards, despite women’s mental health symptoms increasing from pre- to post-abortion. Findings from each scenario support policies that grant abortions on the grounds that continuing a pregnancy would threaten women’s mental health.
The literature on abortion and mental health and the appropriateness of conducting a meta-analysis
While the Fergusson et al. review (2013) does not in fact address policies that allow abortions on the grounds that continuing a pregnancy would lead to mental health problems, it conducts a meta-analysis over two to three studies (depending on the outcome examined) that compares the mental health of women who abort to that of women who have unintended or unwanted pregnancies that end in birth. It should be noted that others have argued that the abortion and mental health literature is not in a state to conduct a meta-analysis because of the high variability in study design and quality (Kendall et al., 2012; National Collaborating Centre for Mental Health, Steinberg et al., 2012). One way in which studies vary is their method of controlling for pre-pregnancy mental health. Fourof the eight studies failed to control for prior mental health (Coleman, 2006; Reardon et al., 2002, 2004; Schmiege and Russo, 2005), a strong predictor of subsequent mental health and a factor that likely confounds the relationship between abortion and mental health (Major et al., 2009; Steinberg and Finer, 2011). Therefore, findings from these studies must be interpreted with the caveat that prior mental health was not controlled for in the analyses. The remaining four studies controlled for prior mental health in different ways. Fergusson et al. (2008) controlled for mental health status within the year before women’s age 15 interview and did include not all possible prior mental health problems. If a woman did not have mental health problems within a year of her age 15 interview and had a mental health problem at some other time before her pregnancy, she was not coded as having had a prior mental health problem. Cougle et al. (2004) excluded those with anxiety symptoms before the pregnancy (Cougle et al., 2005). Gilchrist et al. (1995) conducted separate analyses for those with and without previous psychiatric problems. Steinberg and Russo (2008) included a covariate that assessed whether the person had anxiety before the pregnancy. Pooling findings that did not control for mental health and that controlled for mental health in very different ways, as this meta-analysis does, does not follow guidelines for conducting meta-analyses (Blettner et al., 1999; Deeks et al., 2011) and makes findings difficult to interpret.
Another way in which the study designs vary is the definition and measurement of unintended or unwanted pregnancy. Of the eight studies included in this meta-analysis, various measures of pregnancy intention were used. For instance, Fergusson et al. (2008) defined unwanted pregnancies that ended in birth as those in which the women reported that the pregnancy was unwanted retrospectively or that she had been distressed or very distressed upon learning of the pregnancy. In contrast, Steinberg and Russo (2008) defined unintended pregnancies as those in which women reported retrospectively that they were too soon or were unwanted any time. While inaccurate or unreliable measures of unintended or unwanted pregnancy make findings from individual studies difficult to interpret, distinct measures from different studies make pooled findings in a meta-anlaysis difficult to interpret.
Conclusions
In sum, because the review examines whether abortion relative to delivery of an unwanted or unintended pregnancy is related to women’s subsequent mental health, it does not inform policies that grant women abortions because continuing the pregnancy would harm mental health. Women seeking and obtaining abortions for mental health reasons likely differ in various ways from women who do not seek abortions for an unintended or unwanted pregnancy (e.g. with respect to their pre-existing mental health) that influence the outcome of subsequent mental health. The research which compares women’s pre- to post-abortion mental health finds that anxiety and depressive symptoms decrease from pre- to post-abortion, suggesting abortion does improve women’s mental health. More research which assesses women’s mental health before seeking an abortion, at the time of seeking an abortion, and after obtaining or being denied an abortion is needed. Given the current state of the literature, it is inappropriate to conduct a meta-analysis of the abortion and mental health literature.
Footnotes
Acknowledgements
I would like to thank Diane L Steinberg, Jeanne M Tschann, and James Trussell for comments on an earlier draft.
Funding
Support was provided by the NIH/NICHD Building Interdisciplinary Research Careers in Women’s Health (BIRCWH) K12, grant number: K12 HD052163.
Declaration of interest
The author report no conflicts of interest. The author alone is responsible for the content and writing of the paper.