
Abstract
Objective:
Childhood mental health difficulties affect one in every seven children in Australia, posing a potential financial burden to society. This paper reports on the early lifetime individual and population non-hospital healthcare costs to the Australian Federal Government for children experiencing mental health difficulties. It also reports on the use and cost of particular categories of service use, including the Medicare Benefits Schedule (MBS) mental health items introduced in 2006.
Method:
Data from the Longitudinal Study of Australian Children (LSAC) were used to calculate total Medicare costs (government subsidised healthcare attendances and prescription medications) from birth to the 8th birthday associated with childhood mental health difficulties measured to 8–9 years of age.
Results:
Costs were higher among children with mental health difficulties than those without difficulties. While individual costs increased with the persistence of difficulties, population-level costs were highest for those with transient mental health difficulties. Although attenuated, these patterns persisted after child, parent and family characteristics were taken into account. Use of the MBS-reimbursed mental health services among children with a mental health difficulty was very low (around 2%).
Conclusions:
Australian healthcare costs for young children with mental health difficulties are substantial and provide further justification for early intervention and prevention. The current provision of Medicare-rebated mental health services does not appear to be reaching young children with mental health difficulties.
Introduction
The total annual cost of adult mental health problems to Australian inpatient and community services was recently estimated to range from AU$34m for substance use disorders to AU$177m for anxiety and affective disorders (Mihalopoulos et al., 2005). The onset of mental health problems is often in childhood (Kessler et al., 2005), with one in seven Australian children aged 4–17 years having a mental health difficulty (Sawyer et al., 2001). Of these youth in need of professional health services, only a quarter access professional help for this problem, usually from a family doctor, school counsellor or paediatrician (Sawyer et al., 2001). Nevertheless, children with mental health difficulties are likely to access more general healthcare services than their peers for a range of reasons, including for: (a) diagnosis and/or treatment of the mental health difficulty itself; (b) underlying health or developmental issues contributing to the mental health difficulty (e.g. autism) (Simonoff et al., 2008); and (c) problems associated with the mental health difficulty (e.g. achievement problems at school related to anxiety, attention or conduct problems in class (Pati et al., 2011)). To date, the costs of children’s mental health difficulties to the Australian healthcare system are unknown.
Children can experience mental health problems at any age (Wichstrom et al., 2012). While mood and substance-use disorders tend to appear later in life, around one-quarter of anxiety (e.g. separation anxiety) and impulse-control problems (e.g. attention-deficit/hyperactivity disorder) have onset before age 7 (Kessler et al., 2005), hence there is a substantial need for early-life mental health services. The presentation of childhood mental health difficulties most commonly involves somatic complaints (e.g. headaches, tiredness), delinquent behaviours (e.g. lying, cheating) or attention problems (e.g. poor concentration) (Sawyer et al., 2001). As with adults, comorbidity of mental health disorders is common (Wichstrom et al., 2012). In this paper, we examine data from the Longitudinal Study of Australian Children (LSAC) and determine the excess costs from birth to age 7 years to the Federal Government’s Medicare scheme of children who have mental health difficulties. This scheme includes health services funded by rebates through the Medicare Benefits Schedule (MBS) and prescription medications funded by rebates through the Pharmaceutical Benefit Scheme (PBS). While the majority of childhood prescription medications are likely to be for non-mental health-related conditions (e.g. antibiotics, asthma medications), some children are prescribed medications for mental health difficulties (Hetrick et al., 2007). In November 2006, items were added to the Medicare scheme specifically for mental health-related services under the Better Access Initiative (Crosbie and Rosenberg, 2007). These included special items for mental health-related treatment by medical practitioners and rebates for non-medical practitioner services for people referred by a GP, paediatrician, or psychiatrist. A secondary aim was therefore to examine the use of these specific mental health-related rebated services.
Three research questions were posed: (1) are the mean Medicare (total, MBS, PBS) costs from birth to 4th birthday higher for children with than without mental health difficulties at age 4–5 years?; (2) are the mean Medicare (total, MBS, PBS) costs from the 4th to the 8th birthday higher for children who have any reported mental health difficulties up to 8–9 years compared to children without difficulties?; and (3) are the mean Medicare (total, MBS, PBS) costs from the 4th to the 8th birthday higher for children with persistent childhood mental health difficulties? We model results to the population level to estimate the Australia-wide Medicare costs associated with childhood mental health difficulties. We also explore whether differential costs between children with versus without mental health difficulties are sustained, even when adjusting for key factors that may covary with child mental health and/or use of health services (child gender, child physical health (Chavira et al., 2008), parent mental health (Beardslee and Wheelock, 1994), socioeconomic position (SEP) (Sawyer et al., 2001, 2006) and geographical remoteness (Productivity Commission, 2005)). Finally, we explore how the uptake and costs of key MBS services (family doctor and specialist visits, and specific mental health service items since 2006) vary according to the presence and persistence of mental health difficulties over time.
Materials and method
Data
Data were from the LSAC, a national longitudinal study of children’s health and development commencing in 2004. Detailed information on study design and sample are available elsewhere (Soloff et al., 2005). To provide a geographical distribution similar to the target Australian infant and child populations, a two-stage clustered sampling design was used, with stratification by state and then by major metropolitan centre versus other. Two cohorts were recruited at wave 1: the ‘B’ cohort, comprising 5107 infants who were aged 3–19 months at wave 1 (64% response rate), 2–3 years at wave 2 (2006, n = 4606, 90% retention from wave 1) and 4–5 years at wave 3 (2008, n = 4386, 86% retention from wave 1); and the ‘K’ cohort of 4983 children aged 4–5 years at wave 1 (59% response rate), 6–7 years at wave 2 (n = 4464, 90% retention from wave 1) and 8–9 years at wave 3 (n = 4331, 87% retention from wave 1) (Sipthorp and Misson, 2009). Healthcare costs incurred from 2002 to 2009 were obtained by linkage with Medicare Australia data. The LSAC’s two-cohort, three-wave study design provides a unique opportunity to examine how costs vary across a wide age range (from birth to the 8th birthday) and with the persistence of mental health disorders over time.
The LSAC study and protocol were approved by the ethics committee for the Australian Institute of Family Studies. Consent for participation in the LSAC and Medicare data linkage was provided by a parent at wave 1.
Sample
Children were included in the sample if their parent gave consent for Medicare data linkage and the linkage was successful (93% of B cohort; 92% of K cohort), if they participated in wave 3 and had sufficient child mental health data. Outliers were defined as children with MBS costs in any year above AU$10,000, or PBS costs in any year above AU$8000, yielding three outliers in the B cohort and one in the K cohort. As mean costs were substantially influenced by outliers, these cases were removed from analysis. The final sample was 3605 children for the B cohort and 4006 for the K cohort.
Measures
Medicare costs of health services and subsidised prescription medications were provided for use of the MBS and PBS, yielding MBS costs, PBS costs and total Medicare costs (MBS and PBS combined). Through the MBS, the Federal Government subsidises non-hospital-based medical practitioner care up to a determined amount, with the remainder paid by the patient. Since November 2006, MBS rebates have also been available for a limited number of mental health-related services per year, covering mental health development plans by a GP, psychological services from psychologists, social workers or occupational therapists, consultant psychiatric services and allied health services (Crosbie and Rosenberg, 2007; Department of Health and Ageing, 2010). The cost of these services is distinguished from that of specialist and family doctor visits for some analyses. Pharmaceutical costs are subsidised by the PBS, in which an approved list of prescription medications and formulas is subsidised by an average of 83%, with the remainder paid by the patient (Commonwealth Department of Health and Aged Care, 2000). For the B cohort, costs were calculated from birth to the 4th birthday; for the K cohort, costs were calculated from the 4th to the 8th birthday. Costs were inflated to 2009 dollars using Australian Bureau of Statistics’ consumer price index figures (www.abs.gov.au).
Childhood mental health difficulties were assessed at age 4–5 years (wave 3) for the B cohort and at ages 4–5, 6–7 and 8–9 years (waves 1–3) for the K cohort using the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997). This screening measure is widely used in cohort studies internationally, has concurrent validity against more comprehensive measures (Goodman and Scott, 1999) and is effective in distinguishing children across the full range of psychopathology (Goodman and Goodman, 2009). Parents responded to 25 items regarding their child’s behaviour over the previous 6 months on a three-point scale ranging from 0 = not true to 2 = certainly true. The current study used the total difficulties score (sum of the emotional, conduct, hyperactivity and peer relationship subscales: range 0–40), with higher scores indicating more mental health difficulties.
A lack of Australian SDQ representative norms or clinical cut-points for the ages covered in this study necessitated comparison to UK normative data (Brown et al., 2009). At age 4–5 years the SDQ UK preschool version was used in the LSAC, which has no clinical level cut-points. At ages 6–7 and 8–9 years (K cohort only), we classified children as having a mental health difficulty if their scores were in the borderline (80–90th centile) or abnormal (≥ 90th centile) SDQ ranges of UK norms. For the 4–5-year-olds in both cohorts, we assigned the same proportion of children to the mental health difficulties category as that assigned at 6–7 years in the K cohort. The resulting cut-points were 0–13 (normal) versus 14+ (borderline/abnormal) for the 4–5-year-olds of both cohorts, and 0–14 (normal) versus 15+ (borderline/abnormal) for the 6–7 and 8–9-year-olds.
Demographic characteristics were collected for child gender, child Indigenous status (Aboriginal or Torres Strait Islander), mothers’ and fathers’ education (completed versus did not complete high school), mothers’ primary language spoken at home (English versus not English) and family type (single versus two-parent household). SEP was derived from standardised scores for three variables: combined annual household income, including pensions and allowances before tax (with natural log transformation); parents’ years of education; and parents’ occupation as determined by the status of main occupation. Geographic remoteness of the child’s residence (accessible versus remote/very remote) was coded at the postcode level using the Accessibility/Remoteness Index of Australia (ARIA), which classifies regions according to the required travelling distance for accessing an urban centre containing basic health, education and retail services (Department of Health and Aged Care, 2001). Parent mental health (of the child’s primary carer) was measured using the Kessler 6 scale of psychological distress, on which a score of 13 or more (out of 24) indicates probable diagnosis of a mental health condition (Kessler et al., 2003). Child physical health difficulty was assessed on a single-item, five-point scale which was then dichotomised ‘In general, how would you say your child’s current health is?’ (‘poor/fair/good’ = 1 to ‘very good/excellent’ = 0).
Analyses
For the B cohort, we compared MBS and PBS costs from birth up to the 4th birthday (0–3 years) among children who did and did not have a mental health difficulty at age 4–5 years. For the K cohort, we compared MBS and PBS costs from the 4th to the 8th birthday (4–7 years) according to the number of time points (waves) at which a child had a mental health difficulty. Children with missing SDQ data were conservatively assumed to have no mental health difficulties for that wave. All data were analysed using Stata 11.2 (for PC; StataCorp LP, College Station, TX, USA). As initial and continued participation in the LSAC were less likely among disadvantaged families (Misson and Sipthorp, 2007; Sipthorp and Misson 2009; Soloff et al., 2006), weights accounting for differential non-response and sample attrition were applied in all analyses (Soloff et al., 2006). The complex sample design features (i.e. clustering and stratification) were taken into account using first-order Taylor linearisation.
Differences in demographic characteristics at wave 3 according to mental health difficulties were tested using chi-squared analyses. The range, mean and median of MBS, PBS and total Medicare costs were calculated via descriptive sample statistics. Unadjusted and adjusted (for child gender, child physical health, parent mental health, SEP and geographic remoteness) mean differences were calculated using general linear model regression analyses. Population cost estimates were calculated by multiplying mean differences by the estimated population size, as reported in Australian 2009 population size statistics (Australian Bureau of Statistics, 2010). Ideally, the bootstrap method would be used to ensure robustness of the standard error calculations for skewed data. This method could not be implemented in conjunction with the survey methods (weighting and first-order Taylor linearisation) in place to account for the complex survey design. However, a comparison of means with and without bootstrapping using the data without the survey design revealed very small differences (AU$1–7 maximum difference in 95% confidence interval bounds for total Medicare mean costs per child). Because of this, and because utilisation of standard linear regression techniques for highly skewed cost data is supported in large public health datasets (Lumley et al., 2002), we present results of the standard regression analyses in this paper.
Results
Differences between groups
Table 1 shows demographic characteristics of each cohort according to the number of waves at which participants had a mental health difficulty (SDQ borderline or clinical ranges). In the B cohort, children with a mental health difficulty at age 4–5 years were more likely than those without a mental health difficulty to be male, Indigenous, to have poor physical health, to have a primary carer with poor mental health, and to be disadvantaged on all socio-demographic measures. For example, they were almost twice as likely to be in the most disadvantaged SEP quartile. For the K cohort, the proportion of children experiencing disadvantage increased in a linear fashion with the number of times the child experienced a mental health difficulty. Increased frequency of mental health difficulties was associated with being male, having poor physical health, being in the most disadvantaged socioeconomic quartile, having parents who did not complete high school, having a primary carer with poor mental health, and being from a single-parent household. While being Indigenous and having a mother whose primary language is not English were also associated with mental health difficulties, these did not show linear increases with frequency of mental health difficulties. In contrast to the B cohort, geographic remoteness was not associated with mental health difficulties in the K cohort.
Sample characteristics a , by number of waves with a mental health difficulty.
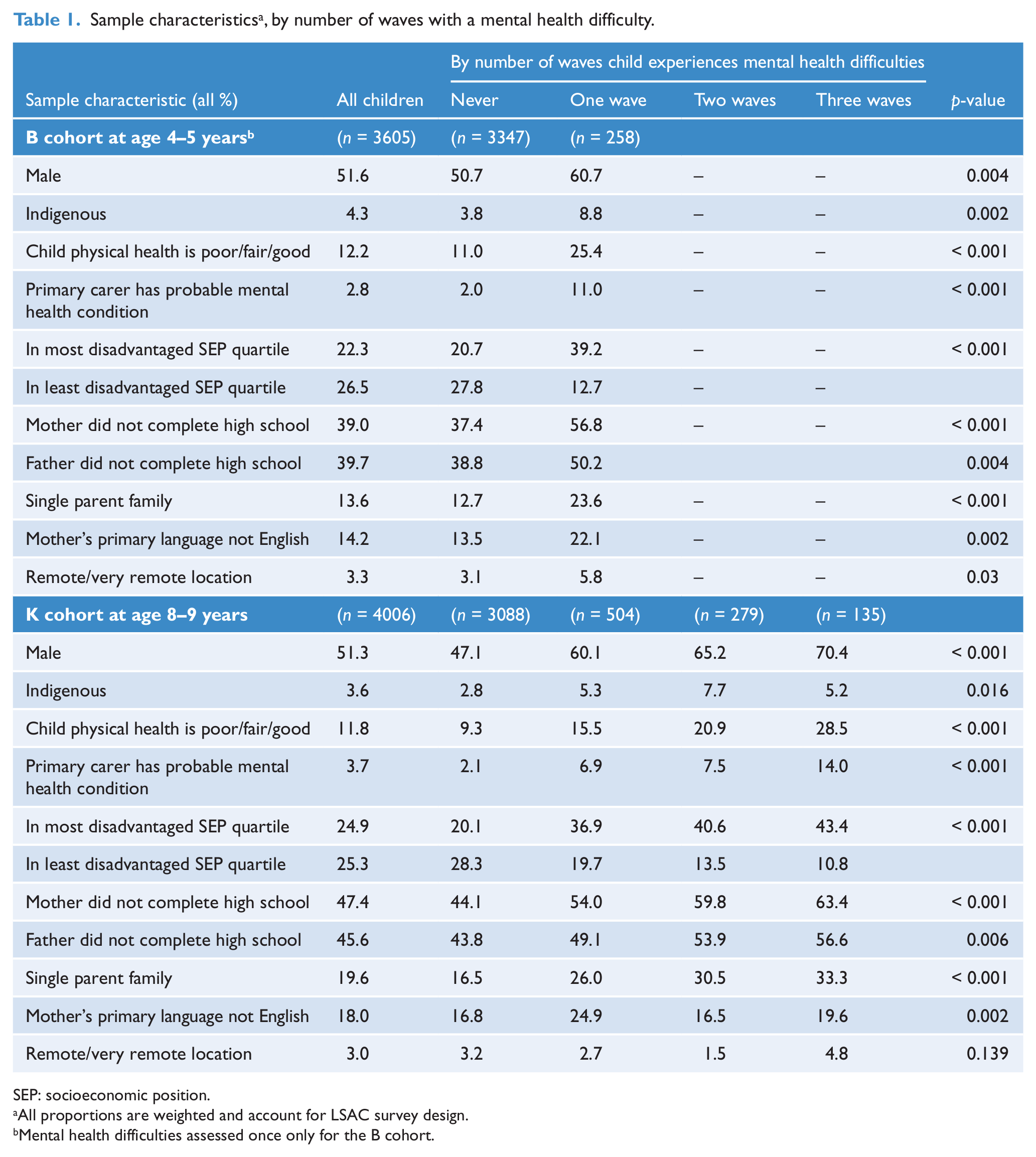
SEP: socioeconomic position.
All proportions are weighted and account for LSAC survey design.
Mental health difficulties assessed once only for the B cohort.
Cost differences between groups
Table 2 shows the range, median and unadjusted and adjusted means of MBS, PBS and total Medicare costs per child over the 4-year period for each cohort. Three general patterns were evident: median costs were consistently lower than mean costs, reflecting a positive skew in cost data; health services use (MBS) contributed more to total Medicare costs than did pharmaceuticals (PBS); and total costs, irrespective of mental health difficulties, were higher from birth to 3 years compared to 4–7 years. Adjusted mean costs tended to be higher than unadjusted means for children without a mental health difficulty and lower for children with a mental health difficulty. Interaction analyses did not provide evidence that the costs associated with mental health difficulties varied by gender (B cohort: presence of mental health difficulty, p = 0.742; K cohort: persistence of mental health difficulties over time, p = 0.620); hence, results are presented for girls and boys combined.
Medicare costs per child a , by presence of / number of waves with a mental health difficulty.
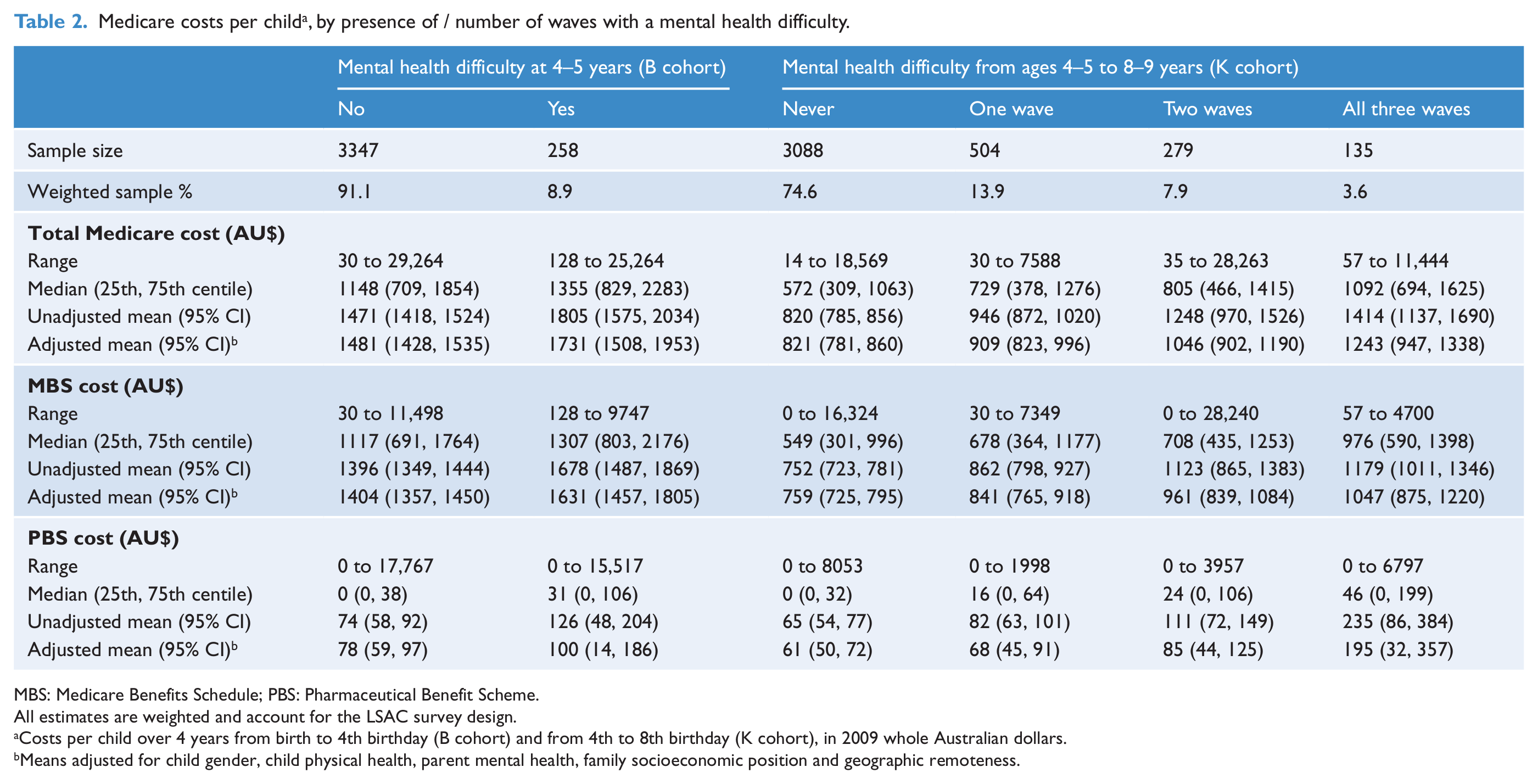
MBS: Medicare Benefits Schedule; PBS: Pharmaceutical Benefit Scheme.
All estimates are weighted and account for the LSAC survey design.
Costs per child over 4 years from birth to 4th birthday (B cohort) and from 4th to 8th birthday (K cohort), in 2009 whole Australian dollars.
Means adjusted for child gender, child physical health, parent mental health, family socioeconomic position and geographic remoteness.
In the B cohort, total Medicare costs from birth up until the 4th birthday were reliably higher for children with than without a mental health difficulty at age 4–5 years; an unadjusted mean difference of AU$334 or 23% (Table 3). This difference reduced to AU$249 (17%) once child, parent and family characteristics were taken into account. In the K cohort, unadjusted costs over ages 4–7 years increased linearly with the frequency of mental health difficulties (p <0.001 for trend). Compared to children who never had a mental health difficulty, costs increased for children with a mental health difficulty at one wave by AU$125 per child (15% increased cost), at two waves by AU$427 (52% increased cost), and at all three waves by AU$593 (72% increased cost). In the adjusted analyses, costs for children with a mental health difficulty at one wave were no longer significantly higher than those for children who never had a mental health difficulty. The excess costs for children with a mental health difficulty at two and three waves remained significant, but were reduced from those in the unadjusted analyses to AU$225 (27%) and AU$422 (51%), respectively.
Four-year Medicare cost differences per child and population estimates of costs a , by frequency of mental health difficulties.
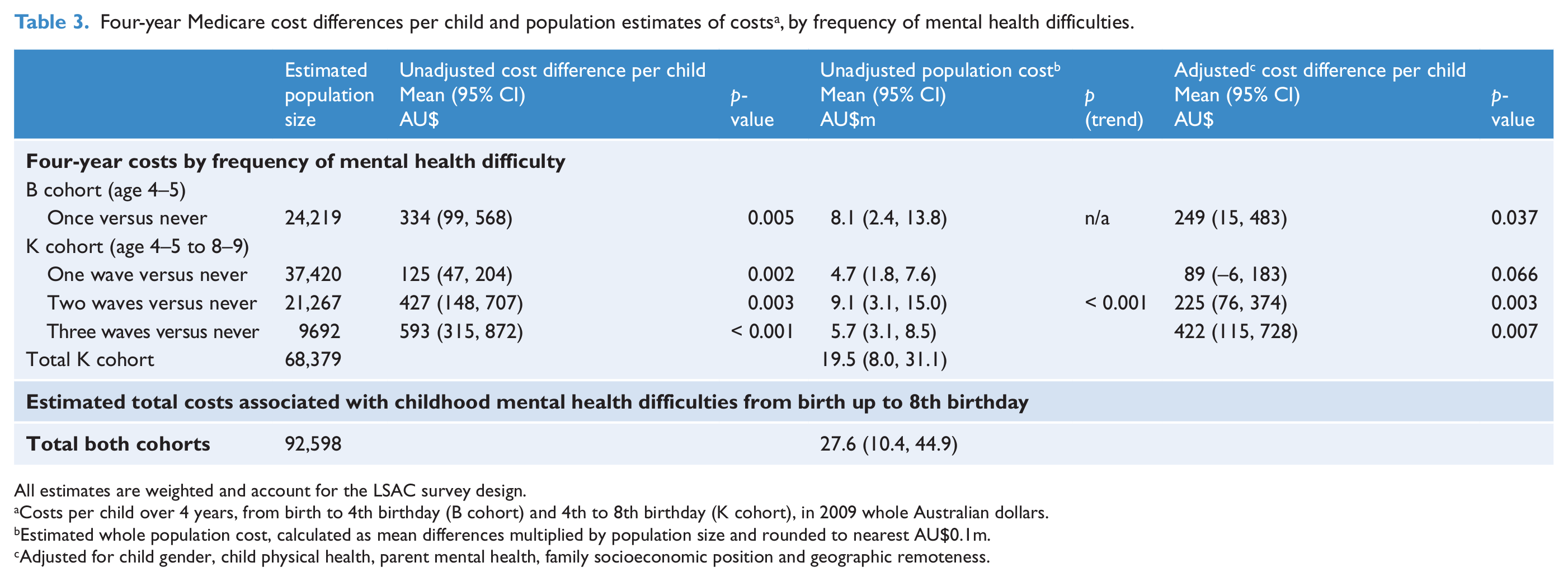
All estimates are weighted and account for the LSAC survey design.
Costs per child over 4 years, from birth to 4th birthday (B cohort) and 4th to 8th birthday (K cohort), in 2009 whole Australian dollars.
Estimated whole population cost, calculated as mean differences multiplied by population size and rounded to nearest AU$0.1m.
Adjusted for child gender, child physical health, parent mental health, family socioeconomic position and geographic remoteness.
Table 3 also shows the extrapolation of these findings to the entire Australian Medicare system, taking into account the proportions of children in the relevant comparison groups. The estimated unadjusted additional cost to Medicare for both healthcare utilisation and pharmaceuticals associated with childhood mental health difficulties from birth up to the 8th birthday was AU$27.6m; AU$8.1m in excess costs for children in their first 4 years of life, and nearly $20m in excess costs for children from the 4th to the 8th birthday.
Finally, Table 4 separates MBS costs by health service provider, showing the proportion of children who used, and the cost of, MBS items related to different health services. The overall proportion of children using the Better Access mental health items was very low (around 2% for children with a mental health problem), although the likelihood of their use and cost tended to be higher among children with than without a mental health difficulty in both cohorts. This low use contrasted with the use of specialist and family doctor visits, used by over 34% and 99% of all children, respectively. The use and cost of specialist visits increased with the frequency of mental health problems in the K cohort, but no differences were observed in the B cohort. Almost all children in both cohorts had visited a family doctor in the 4-year period and the cost of these visits increased with the presence/frequency of mental health problems, likely reflecting more frequent attendance by children with poor mental health.
Proportion of children accessing, and 4-year cost a of, MBS services by health service provider and mental health.
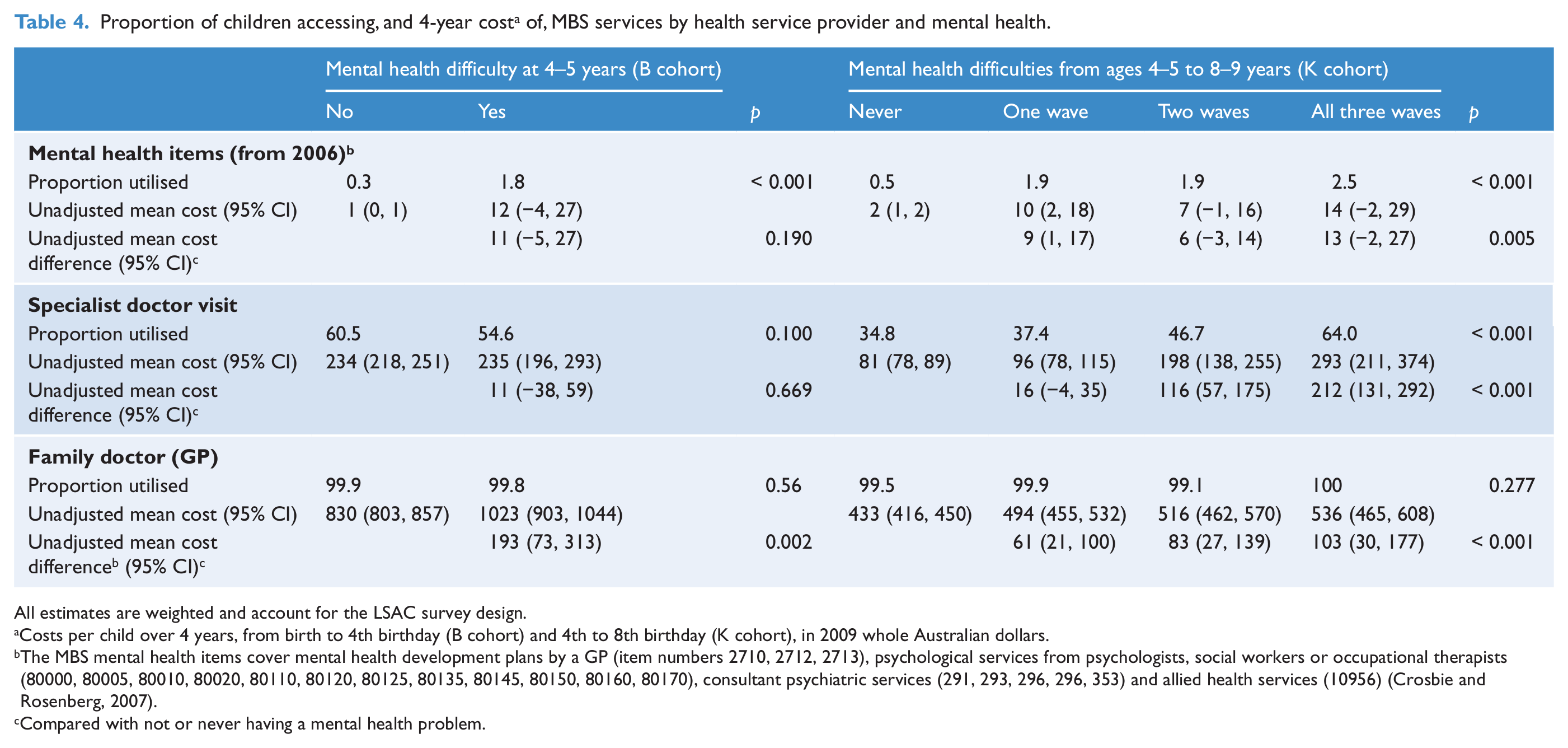
All estimates are weighted and account for the LSAC survey design.
Costs per child over 4 years, from birth to 4th birthday (B cohort) and 4th to 8th birthday (K cohort), in 2009 whole Australian dollars.
The MBS mental health items cover mental health development plans by a GP (item numbers 2710, 2712, 2713), psychological services from psychologists, social workers or occupational therapists (80000, 80005, 80010, 80020, 80110, 80120, 80125, 80135, 80145, 80150, 80160, 80170), consultant psychiatric services (291, 293, 296, 296, 353) and allied health services (10956) (Crosbie and Rosenberg, 2007).
Compared with not or never having a mental health problem.
Discussion
This is the first Australian study to assess the healthcare costs associated with early life mental health difficulties in a nationally representative sample. Our findings highlight the very early age at which mental health-related cost differences arise. Mental health difficulties were associated with higher Medicare costs in the first 4 years of life (unadjusted mean difference AU$334 per child) and from the 4th to the 8th birthday (unadjusted mean difference AU$125 to AU$593 per child), with these patterns remaining after adjusting for child, parent and family characteristics. For the younger cohort, those who had mental health difficulties at age 4–5 years had elevated Medicare costs at both earlier time-points as well as at age 4–5 years (data not shown). In the older cohort, individual costs increased with the persistence of mental health difficulties over the three data collection waves in both the unadjusted and adjusted analyses. We presented costs data for girls and boys combined. Despite the higher prevalence of mental health difficulties among boys, exploratory analyses revealed no gender interactions in predicting costs.
Despite our reliance on UK norms for identifying mental health difficulties, the rates of mental health difficulties identified in this study are broadly consistent with previous Australian estimates. Fourteen percent of K cohort children had a mental health difficulty at one wave, which is almost identical to the prevalence of mental health disorders among 4–17-year-olds reported by Sawyer et al. (2001). As expected, given the longer (6-year) period of data collection, we found a much higher proportion (25%) of K cohort children reporting mental health difficulties at one or more waves. The prevalence of mental health difficulties among 4–5-year-olds in the B cohort (9%) was lower than the prevalence reported by Sawyer for 4–17-year-olds, likely reflecting the younger and more narrow age distribution of our sample.
When scaled to the population level, childhood mental health difficulties were associated with an estimated excess Medicare cost of AU$8.1m over the first 4 years of life and AU$19.5m from the 4th to the 8th birthday (unadjusted). At the population level, additional Medicare costs were highest for the group of children with a mental health difficulty at two waves (representing 7.9% of the population, AU$9.1m unadjusted) rather than those with difficulties at one wave only (13.9%, AU$4.7m) or at all three waves (3.6%, AU$5.7m unadjusted). This reflects the combined effects of higher individual costs with increased persistence, and the relative size of the population sub-groups. Prevalence differences also accounted for higher population costs for mental health difficulties at ages 4–7 compared to 0–3 years. While individual costs were generally higher at the younger ages, the prevalence of mental health problems was substantially smaller in the younger cohort. Again, these patterns persisted once child, parent and family characteristics had been taken into account.
It is somewhat reassuring to note the majority of children in the older cohort had a mental health difficulty at only one wave of data collection. In addition to their lower individual Medicare costs, children with short-term difficulties are less likely to develop adult mental health disorders (Reef et al., 2011) and pose less burden on families and other service providers than those with persistent childhood difficulties. However, it should be noted that we assessed mental health problems until age 8–9 years only, and the mental health difficulties of some children will persist into adolescence.
Consistent with a previous evaluation (Crosbie and Rosenberg, 2007), we found very low uptake of the Better Access mental health items among children, observing around 2% for children with a mental health difficulty in both cohorts. This contrasted strongly with the use of MBS items related to specialists and family doctors, used by over 34% and 99% of children, respectively, and suggests that a key at-risk group may be missing out on the benefits of these MBS entitlements.
It was not possible with the LSAC data to establish whether these increased costs directly reflected children’s access to assessment or treatment for their mental health difficulties per se. Medicare data do not readily identify the diagnostic reasons for service use and the costs estimated here will include services for unrelated conditions as well as those which may have led to or arisen from mental difficulties. Comorbidity is likely to be an important factor in the elevated healthcare costs (Waters et al., 2008). For example, children with chronic health conditions (Combs-Orme et al., 2002) and those with learning difficulties (Frazier et al., 2007) are at increased risk for mental health difficulties and it may be these conditions or their combination that drive the use of Medicare services. More research is required to determine the extent to which excess Medicare costs are actually appropriate and necessary costs, and which costs may be preventable through earlier or different treatment.
While substantial, the healthcare costs estimated here are likely to be only a fraction of the real cost burden to Australia of early life mental health difficulties. Medicare data do not include the cost of the large number of mental health treatment and prevention services provided by non-government organisations, school counsellors or state-based Child and Adolescent Mental Health Services (CAMHS). Nor do they include other government costs such as the cost of hospital admissions, emergency department presentations or preventative measures such as the Positive Parenting Program recently implemented by the government of New South Wales (www.families.nsw.gov.au). We also could not estimate broader societal costs including family out-of-pocket expenses, parent time and loss of productivity, and indirect supports provided through the education and welfare systems. Three small studies conducted in the UK involving children aged 10 years or younger (sample sizes of 10 to 142) showed that those with clinical disorders and/or receiving care through mental health services, incurred average annual costs in the order of £6000 to £24,000 per child (Knapp et al., 1999; Romeo et al., 2006; Scott et al., 2001). Across the studies, the greatest costs were borne by families, followed by justice, education and welfare services, with health costs being comparatively small.
The current research provides an important starting point for understanding the cost burden of very early mental health difficulties in Australia. Future research is needed to determine how the costs of these problems are distributed across sectors and families, how the amounts and balance of costs vary as children progress through middle childhood and into adolescence, and the extent to which early intervention and treatment deflect, redirect or reduce societal costs. Such work is critical for providing the evidence base necessary to determine how, when and to whom services should be directed. The current study provides important initial foundations for informing future services. Our data showed that: (1) childhood mental health difficulties are associated with additional healthcare costs from birth; (2) at an individual level, costs increased with the persistence of problems; and (3) at a population level, even transient difficulties contributed substantially to healthcare system costs. Importantly, these findings were upheld after adjusting for major confounding factors such as SEP, parent mental health and child physical health. This provides support for intervention efforts to focus on early prevention in addition to treatment, across the full spectrum of mental health difficulties, not solely the severe clinical end. Our analyses also suggest that the new mental health services rebated by Medicare are not used by the majority of young children who experience a mental health difficulty, and thus a key time point for intervention may be missed for these children.
Footnotes
Funding
This article uses confidential unit record files from the Longitudinal Study of Australian Children (LSAC) survey. The LSAC project was initiated and funded by the Commonwealth Department of Families, Housing, Community Services, and Indigenous Affairs and was managed by the Australian Institute of Family Studies. The findings and views reported in this article are those of the authors and should not be attributed to either the Commonwealth Department of Families, Housing, Community Services, and Indigenous Affairs or the Australian Institute of Family Studies. We thank all the families participating in the LSAC study. Drs Mensah, Bayer and Gold were funded by NHMRC Population Health Capacity Building Grants (FM, JB: 436914 and LG: 425855), NHMRC Early Career Research Fellowships (FM: 1037449; LG: 1035100), and Australian Rotary Health Postdoctoral Fellowship (JB). Professors Wake and Nicholson were supported by NHMRC Career Development Awards (MW: 546405; JN: 390136). MCRI research is supported by the Victorian Government’s Operational Infrastructure Support Program, and the Parenting Research Centre receives funding from the Victorian Government Department of Education and Early Child Development. We acknowledge the peer review provided by the LSAC analysis group comprising staff from the Parenting Research Centre and Murdoch Childrens Research Institute.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.