
Abstract
Objective:
Relapses in psychosis are costly and may have irreversible consequences. Relapse prevention is thus critical in the treatment of schizophrenia. Apart from medication discontinuation, a consistent relapse predictor has not been identified due to limitations in previous studies. We aim to investigate relapse predictors in a large cohort of patients with first-episode psychosis.
Method:
This is a retrospective cohort study designed to evaluate relapses in first-episode psychosis patients in 3 years. A total of 1400 patients’ case records were retrieved from a hospital database. Potential relapse predictors including demographic variables, baseline clinical measures, medication adherence, and residual positive symptoms upon clinical stabilization were collected.
Results:
The cumulative relapse rates were 19.3% by year 1, 38.4% by year 2, and 48.1% by year 3. Multivariate Cox-proportional hazards regression analysis revealed that medication non-adherence, smoking, schizophrenia diagnosis, younger age, and shorter baseline hospitalization were associated with an increased risk of relapse in 3 years.
Conclusions:
Nearly half of patients relapsed after 3 years following their first-episode psychosis. Smoking as a predictor of relapse is an intriguing new finding supportive of a link between nicotinic receptors and the dopamine system. Their relationship deserves further investigations with potential clinical implications for relapse prevention.
Introduction
Relapse prevention is one of the most important and challenging targets in the treatment of psychotic disorders. Relapse is the exacerbation or re-emergence of positive symptoms, which often co-occurs with functional and behavioural changes (Burns et al., 2000). Previous double-blind medication discontinuation studies revealed a 1-year relapse rate of 41–79% in first-episode psychosis patients (Kane et al., 1982; Crow et al., 1986; Hogarty and Ulrich, 1998; Chen et al., 2010). A relapse rate of 40% was found in a naturalistic study in Hong Kong in patients with first-episode psychosis by the end of 3 years (Chen et al., 2005b). Relapses and rehospitalizations impose substantial costs to patients, caregivers, and the healthcare system (Weiden and Olfson, 1995). After each relapse, patients will have poorer treatment response and longer time to remission (Lieberman, 1996). The identification of relapse predictors will help devise prevention strategies.
Medication non-adherence is at present the only consistent relapse predictor with high predictive power (Robinson et al., 1999; Chen et al., 2005b; Ucok et al., 2006). Many interventional strategies, such as combination of educational and behavioural approaches, have therefore been proposed to improve medication adherence (Hogarty et al., 1991; Xiong et al., 1994; Zygmunt et al., 2002; Dolder et al., 2003). Further studies are needed to identify more useful relapse predictors other than non-adherence. It is also noted that, in a small proportion of patients, factors other than medication discontinuation are predictive of relapse (Chen et al., 2010).
Results of other relapse predictors were mixed and inconclusive. Some demographic and clinical factors have been suggested, including male gender (Angermeyer et al., 1989; Tohen et al., 1992), younger age at first onset of psychotic episode (Haro et al., 2006a), and lower level of education (Lay et al., 2006; Rosca et al., 2006). However, these findings were not replicated in other studies (Johnstone et al., 1990; Lenior et al., 2005). In chronic patients, symptom severity was associated with greater risk for subsequent relapse (Lenior et al., 2005; Hides et al., 2006; Schennach et al., 2012). In some first-episode studies, longer duration of untreated psychosis (DUP) was associated with relapse and rehospitalization (Crow et al., 1986; Larsen et al., 2000); a few studies suggested a diagnosis of schizophrenia to be related to relapse (Csernansky and Schuchart, 2002; Lenior et al., 2005), while others failed to find a relationship (Linszen et al., 1997; Robinson et al., 1999). Certain naturalistic studies have also suggested that a history of hospitalization may indicate higher chance of relapse and rehospitalization (Olfson et al., 1999; Wong and Chung, 2006). In a recent meta-analysis of risk factors for relapse in first-episode psychosis, results showed that medication non-adherence, persistent substance use, criticism from carers, and poorer premorbid adjustment increased the risk of relapse (Alvarez-Jimenez et al., 2012). However, the predictive power of these clinical factors and demographic variables were low. Overall, the relapse predictors identified thus far in the literature were either inconsistent or weak, probably due to differences in diagnostic criteria used across studies and their relatively small sample size.
The present study was part of a retrospective cohort study in Hong Kong evaluating the 3-year outcome in 1400 first-episode psychosis patients receiving phase-specific early intervention or standard psychiatric care (Chen et al., 2010). In this analysis, we explored potential predictors for relapse in 3 years: (a) demographic variables; (b) clinical factors and symptom severity at baseline; (c) type of treatment received at baseline (phase-specific early intervention or standard care); (d) residual symptoms at clinical stabilization; and (e) medication adherence at clinical stabilization.
Materials and methods
Study setting
This was part of a retrospective cohort study evaluating the 3-year outcome in 1400 patients receiving phase-specific early intervention in the Early Assessment Service for Young people with psychosis (EASY) service or standard care prior to EASY. EASY is a territory-wide service for young people with first-onset psychotic disorders aged between 15 and 25 in Hong Kong launched since 2001 (Chen, 2004; Wong et al., 2012). In this study, 700 patients in the EASY service were managed by an early intervention multidisciplinary team; each patient had a designated case manager specifically trained for early psychosis intervention, who provides individualized care plan and assertive follow up for 2 years; atypical antipsychotics or low-dose conventional were used as first-line treatment; medication adherence was encouraged; and relapse risk is communicated and emphasized by case managers and clinicians. For the other 700 patients who received standard care, their management consisted mainly of inpatient treatment for the first episode (via accident and emergency department, or after months of referral waiting time), followed by relatively sparse outpatient follow up with little psychosocial support; they were managed by general psychiatric teams without specialized training for early intervention of psychosis.
Participants
Case records were retrieved from the Psychiatric Case Register in Hong Kong. They consist of 700 consecutive patients from the EASY programme between 2001 and 2003, and 700 consecutive patients who received standard care between 1998 and 2001 (i.e., before the launch of the EASY programme). The two groups were individually matched for gender, diagnosis, and age (±3 years) (Chen et al., 2011). Cases were included in the study if they had any of the following diagnoses according to the International Classification of Diseases and Related Health Problems tenth revision (ICD-10): schizophrenia (ICD-10 code F20), acute and transient psychotic disorders (ICD-10 code F23), schizoaffective disorders (ICD-10 code F25), psychosis not otherwise specified (ICD-10 codes F28 or F29), and affective disorders with psychotic features (ICD-10 codes F30.2, F31.2, F31.5, F32.3 or F33.3). Patients with significant organic condition, drug-induced psychosis, or mental retardation were excluded. Patients who had received prior psychiatric treatment for more than 1 month before first known to the Register were also excluded. Informed consent from individual patients was waived by the institutional review board and ethics committees of the applying sites.
Assessments
Relapse status was recorded each month during the 3-year follow-up period. We defined relapse as the recurrent or exacerbation of positive symptoms necessitating a change in management, such as hospitalization or revised medication regimen (Chen et al., 2011). Exacerbation of positive symptoms was operationally defined as a rating of 3 (“mildly ill”) or above in positive symptoms in Clinical Global Impressions – Severity Scale (CGI-S) (Guy, 1976). The CGI-S is an impression measure of the overall clinical picture of patients. It is rated on a 7-point scale ranged from normal, borderline, mild, moderately, markedly ill, severely ill, to most extremely ill by trained researchers based on narrative descriptions as recorded in case notes.
Potential predictors including demographic, baseline, and clinical stabilization (defined as the 1-month period following the end of the first-episode psychosis) variables were recorded. The demographic variables were gender, age, years of education, and smoking status (non-smoker, current smoker, or ex-smoker).
The baseline clinical variables were: age of onset; mode of onset (acute 1–7 days, subacute 1–4 weeks, gradual >4 weeks); substance use; hospitalization duration (days of first psychiatric admission during the first psychosis episode); treatment group (early intervention or standard care); diagnosis; positive, negative, and affective symptoms as measured using the CGI-S, and DUP. DUP was defined as the period (in days) between first appearance of psychotic symptoms and use of effective psychiatric treatment as assessed by clinicians. For the purpose of analysis, a cut-off of 30 days was used to categorize patients into groups of short or long DUP.
The clinical stabilization variables were: medication compliance (good/fair, poor, or unplanned discontinuation, discontinuation without discussion with clinicians) based on (a) routine assessment by clinicians as recorded in case notes; (b) drug dispensing records during inpatient stay; and (c) patients’ self-report of remaining amount of medications as recorded in the case records; residual positive symptoms was defined as absent or present (score 3–7 on CGI-S positive symptoms)
Data extraction procedures and inter-rater reliability
Except for demographics and baseline clinical variables, data were extracted from case notes by dividing the 3-year follow-up period into 36 equal intervals, each lasting 1 month, according to a structured format with operationalized definitions by trained researchers with psychology background. Raters were not blind to the purpose of the study, patients’ outcomes, or their treatment groups. Only data that could be reliably extracted from the case records were retrieved and analyzed.
Inter-rater reliability were tested using intra-class correlation coefficient (ICC) in 12 cases. Satisfactory concordance was demonstrated between clinician and trained researcher ratings, with ICC of 0.78 for DUP and 1.00 for duration of hospitalization; the concordance between trained researchers were similar, with ICC 0.70 for DUP and 1.00 for duration of hospitalization. During the data collection period, weekly consensus meeting among clinicians and researchers were held to resolve ambiguity.
Statistical analysis
Cox proportional hazards regression was used to identify candidate relapse predictors by examining the time to relapse and its relationship with independent variables. The event was a binary variable (relapsed or not relapsed) describing the observed relapse outcome in 3 years. The time variable was the time to relapse, drop out, or uneventful study completion.
A univariate Cox proportional hazards regression was first run for each variable. Only variables showing results with p-value ≤0.1 smaller were included in the final multivariate Cox proportional hazards regression (stepwise forward method). In the multivariate analysis, a p-value <0.05 were considered statistically significant. The hazard ratio (HR) was calculated: an HR of 1 indicates the same relative risk of relapse compared with the reference group; an HR <1 indicates lower relative risk, and an HR >1 indicates higher relative risk. Statistical Package for Social Sciences (SPSS) version 19.0 was used for statistical analyses.
Results
Characteristics of study population
Table 1 shows the characteristics of the study population. The cumulative relapse rate was 19.3% (n=270) by year 1, 38.4% (n=537) by year 2, and 48.1% (n=674) by year 3. Approximately 17.7% (n=248) of the population had multiple relapses (defined as >2 relapses in 3 years).
Characteristics of the study population.
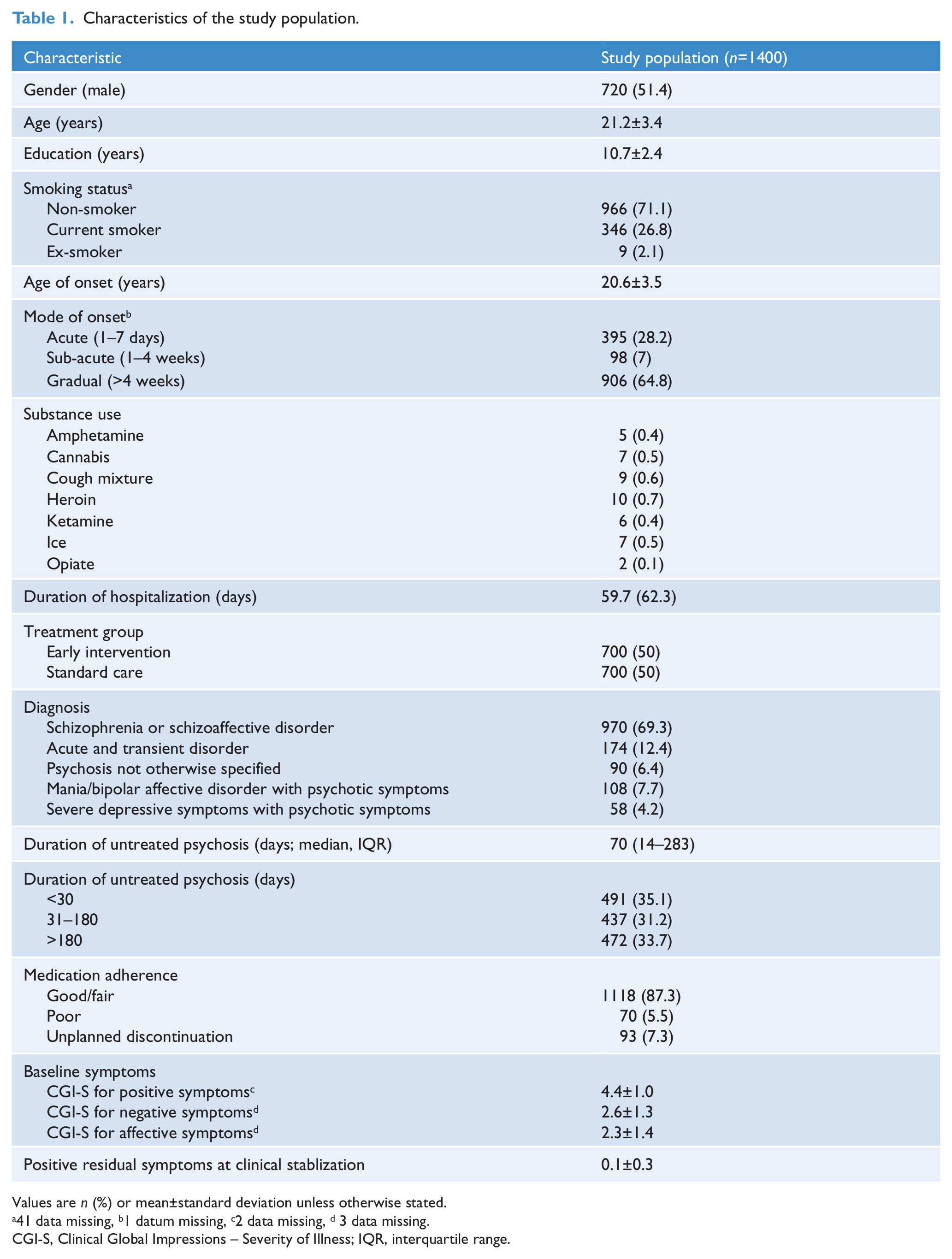
Values are n (%) or mean±standard deviation unless otherwise stated.
41 data missing, b1 datum missing, c2 data missing, d 3 data missing.
CGI-S, Clinical Global Impressions – Severity of Illness; IQR, interquartile range.
Predictors of relapse
Each of the demographic, baseline, and stabilization clinical variables was entered into the univariate Cox-proportional hazards regression. Univariate results showing a p-value of 0.1 or smaller were age (p=0.028), years of education (p=0.072), diagnosis of schizophrenia (p<0.000), DUP (p<0.045), smoker status (p=0.028), baseline affective symptom severity (p=0.002), duration of baseline hospitalization (p=0.07), and medication adherence at clinical stabilization (p<0.000).
Predictors identified in the univariate analyses were included in the final multivariate analysis (n=1365). Table 2 shows that medication non-adherence (HR 2.36, 95% CI 1.76–3.17, p<0.001), current smoker status (HR 1.42, 95% CI 1.15–1.76, p=0.001), a diagnosis of schizophrenia (HR 1.41, 95% CI 1.13–1.77, p=0.003), younger age (HR 0.97, 95% CI 0.939–0.997, p=0.032), and shorter duration of baseline hospitalization (HR 0.998, 95% CI 0.996–1.000, p=0.029) increased the risk of relapse in first-episode psychosis patients by the end of 3 years.
Significant predictors of first relapse in multivariate Cox-proportional hazards regression (n=1365).
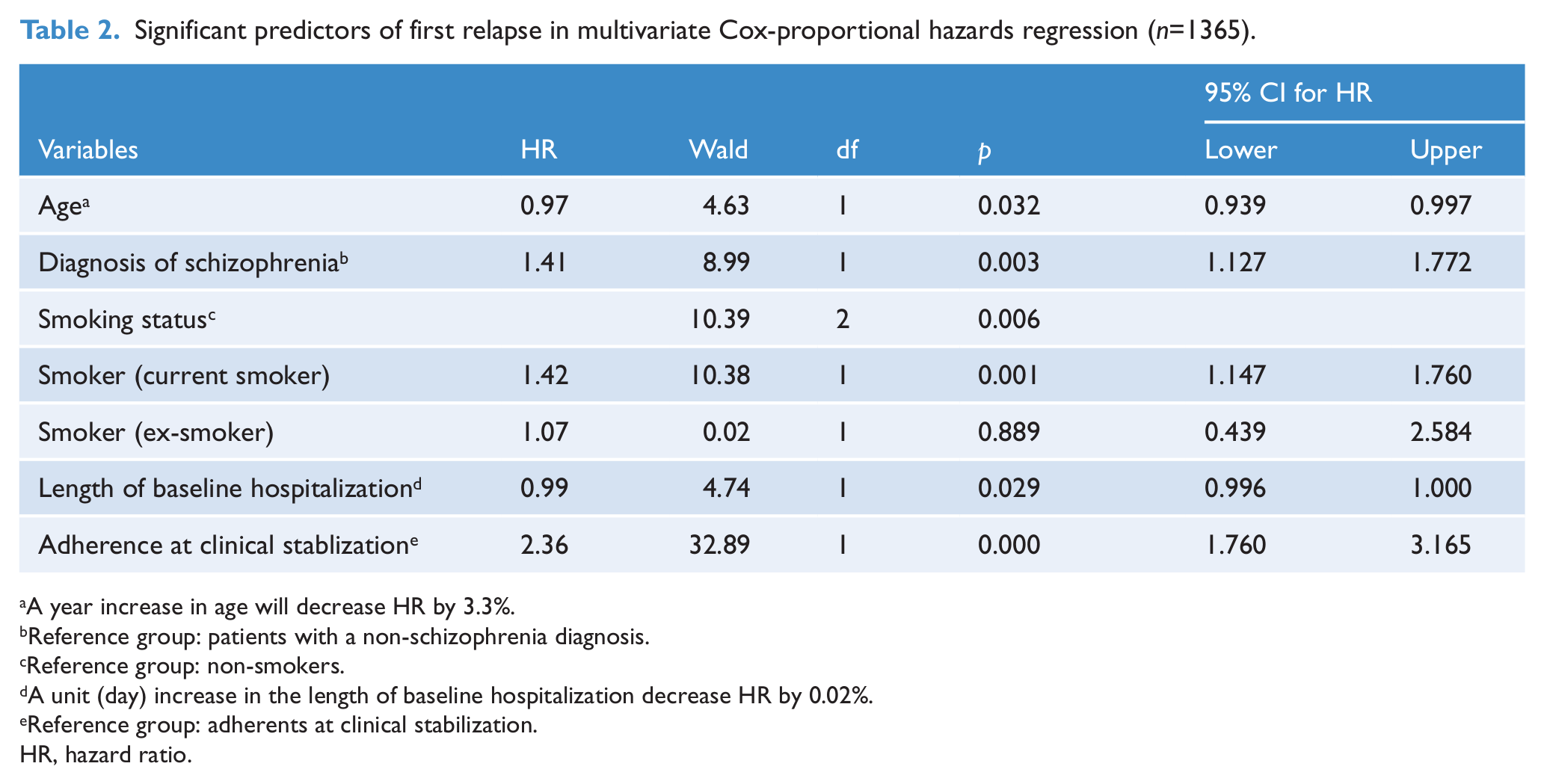
A year increase in age will decrease HR by 3.3%.
Reference group: patients with a non-schizophrenia diagnosis.
Reference group: non-smokers.
A unit (day) increase in the length of baseline hospitalization decrease HR by 0.02%.
Reference group: adherents at clinical stabilization.
HR, hazard ratio.
Discussion
We explored the predictors of relapse at 3 years after the first episode of psychosis in a large cohort of 1400 patients. An increased risk of relapse in 3 year was significantly predicted by medication non-adherence, smoking, a diagnosis of schizophrenia, younger age, and shorter length of hospitalization at baseline.
Medication non-adherence was found to be a strong predictor for relapse in our patients with first-episode psychosis. This is consistent with previous studies regardless of the definitions of non-adherence used: from the narrowest sense of no medication taken for a defined period of time (Doering et al., 1998) to the less stringent definition of taking less than half (Sullivan et al., 1995) or 70% (Chen et al., 2005b) of the prescribed medication, all previous studies have demonstrated a significant role of medication discontinuation in relapse. In our study, medication non-adherence is a problem even among patients who received regular psychoeducation about the importance of compliance and the related risk of relapse. A potential explanation is that patients may underestimate and misinterpret the risks suggested by clinicians and case managers. A study by Windschitl and Weber (1999) demonstrated that interpretation of an exact value of percentage is susceptible to context effect. Another study found that people had considerable variability in interpreting the same verbal phrase, e.g. “likely” (Wallsten et al., 1986). It is of clinical importance to ensure the message about risk is accurately understood by patients. However, among the very few studies on risk perception, one showed that half of the patients underestimated the risk of relapse to be 30% or less (Chen et al., 2005a). About 20% of the patients even denied any risk at all. Further studies that examine the relationship between the perception of relapse risk, medication adherence, and relapse are important.
Interestingly, being smokers had 1.42-times higher chance of relapse compared with non-smokers. Although substance abuse has been identified as a powerful relapse predictor in many studies (Swofford et al., 1996; Haro et al., 2006b; Wong and Chung, 2006; Schennach et al., 2012), little evidence has been suggested regarding smoking and relapse. The identification of smoking as a predictor of relapse in patients with psychosis is an interesting, novel finding. Tobacco smoking is regarded as the most common way of nicotine administration. Nicotine acts centrally within the ventral tegmental area to release dopamine, as well as in the thalamic reticular nucleus and the hippocampus on GABAergic neurons. Studies have shown that nicotine enhances those neurocognitive processes that are known to be dysfunctional in psychosis, such as memory, attention, and learning (Grottick and Higgins, 2000; Hahn and Stolerman, 2002). Reports suggested that some important brain nicotinic receptor subunits were involved in cognition (Grottick and Higgins, 2000) while their deficiency may also contribute to the aetiology of schizophrenia (Freedman et al., 1995). Given the direct link between nicotinic receptors and the dopamine system, and their involvement in the neurocognitive dysfunctions observed in psychosis, the current finding of smoking being a predictor of relapse is a plausible and a potentially important observation with intervention implications. It is important to determine whether smoking itself results in changes in the nicotinic system that are contributory to the relapse risk, and whether the cessation of smoking would result in a reduction of relapse risk. On the other hand, cigarette smoking was found to interfere with the metabolism of various medications (Zhang et al., 2006) and relapse may occur due to decreased bio-availability of antipsychotics. Further studies are needed to clarify the potential adverse effects of cigarette smoking on the bio-availability of psychotic medications. Furthermore, many studies suggested that cigarette smoking is closely related with substance abuse, especially in adolescence (Myers and Kelly, 2006). This raises the possibility that smoking may be a secondary or mediator variable associated with relapse in first-episode psychosis. However, little evidence regarding this notion was found in the present study as only around 3% of the cohort reported to have substance use. The prevalence of substance abuse in Hong Kong is far less than that reported in the Western culture. Hence, the linkage between cigarette smoking and substance use may not be as clear as those demonstrated in the Western populations. The role of smoking deserves more attention as it is a relatively neglected area in outcome predictor studies (Murray, 2003; Tregellas et al., 2007). This will be an important area for further investigations.
Another significant finding is that the diagnosis of schizophrenia is moderately associated with relapse. Research has demonstrated that the diagnosis of schizophrenia is related to poorer outcome as compared with schizoaffective disorders (Csernansky and Schuchart, 2002) or other schizophrenia-related disorders (Loo et al., 1997; Lenior et al., 2005; Rosca et al., 2006). However, results were mixed and negative findings have been suggested (Linszen et al., 1997; Robinson et al., 1999). The inconsistency may be due to the fact that different patient samples and diagnostic tools were used across different studies. Moreover, younger age was shown to be a modest relapse predictor. One of the possible explanations is that younger patients tend to stop medication themselves (Hui et al., 2006), which may lead to higher medication non-adherence and an increased risk of relapse. Shorter length of baseline hospitalization was also related to relapse. As reported in the main study (Chen et al., 2011), the type of intervention (early intervention vs. standard care) turned out to be insignificant in predicting relapse. We postulate patients with early intervention had significantly shorter hospital stay and early signs of relapse might have been managed with intensive outpatient care. Therefore, favourable outcome in relapse could not be seen in the early intervention group. It should also be noted that assessing fidelity to treatment guidelines was difficult with the current study design of case note review. Currently, findings on the effectiveness of intervention are still inconclusive and mixed. There is no particular psychological treatment which has shown a definite reduction in relapse rate. In a recent meta-analysis on 109 relapse predictors, none of them was related to psychological treatment (Alvarez-Jimenez et al., 2012). The notion that psychological treatment as a relapse predictor is still an understudied area.
Our investigation has also confirmed local finding on relapse rates in a 3-year prospective longitudinal study (Chen et al., 2011). We found that the first, second, and third year cumulative relapse rates were 20, 40, and 50%, respectively. It is comparable to local naturalistic first-episode psychosis study where 20, 33, and 40% relapse rates were found in the first, second, and third year (Chen et al., 2005b). Additionally, the current findings on relapse rate are comparable to other early psychosis studies programmes. For instance, a 2-year longitudinal cohort study on early psychosis treatment programme conducted in Canada showed that the 2-year relapse rate was 35.7% (Addington et al., 2007). We believe that the current retrospective method may provide a reliable and comparable estimate on the risk of relapse as compared to prospective method. Of note, the lack of consensus in relapse definition may be one of the possibilities leading to inconsistent findings of relapse rates in different studies.
There are some limitations in the study which need to be addressed. First, there were some potential drawbacks in the current definition of relapse, leading to overestimation of relapse in some cases since a CGI severity score of 3 is a relatively low threshold, as well as under-stimation in some cases where patients relapsed but did not involve a change in medication. Also, some other criteria such as duration, negative symptoms, and functioning levels had not been included in defining relapse. Secondly, some potential imperative predictors such as stressful life events have not been included. Thirdly, since data were retrieved from case records, additional information on psychopathology, psychosocial, and case histories were not available. Lastly, because of the nature of case note review, raters were not blind to the purpose of the study and the outcomes of patients. Training was therefore given to raters in order to minimize bias from data collection. Based on the novel findings in relation to cigarette smoking, we believe that some clinical recommendations are warranted. We suggest that psychoeducation about smoking and its association with increased relapse risk should be given to young patients with first-episode psychosis. Smoking cessation interventions should also be taken into consideration.
Footnotes
Acknowledgements
The authors would like to acknowledge all coordinating clinicians, staff and patients from the participating hospitals, clinics, medical records department, as well as research assistants, who helped arrange the logistics and data collection.
Funding
The study was supported by Health and Health Service Research Fund by the Food and Health Bureau, the Government of Hong Kong Special Administrative Region. The grant number was 03040141.
Declaration of interest
EH-ML has participated in paid advisory board for AstraZeneca and Eli Lilly. EY-HC has participated in paid advisory board for Otsuka, has received educational grant support from Janssen-Cilag, and has received research funding from AstraZeneca, Janssen-Cilag, Pfizer, Eli Lilly, Sanofi-Aventis, and Otsuka. All other authors declare that they do not have any conflicts of interest. The other authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.