
Abstract
Objective:
To report the views of parents, general practitioners and practice nurses on the proposed changes to incorporate social and emotional health checks of three-year-olds into the Healthy Kids Check, a one-off pre-school health assessment delivered through general practice.
Method:
Participants were recruited from three socio-culturally diverse urban areas of Melbourne for a qualitative study involving 28 parent interviews and six focus groups with a total of 40 practitioners. Participants discussed child social and emotional development, health-seeking and preventive health care for young children. Transcripts were thematically analysed.
Results:
Common themes showed: (i) Although both parents and practitioners were receptive to the idea of social and emotional screening, parents had limited knowledge about mental health issues for young children and the need for early intervention. (ii) All groups questioned the current capabilities of practice staff to identify problems, and practitioners expressed a need for further training and tools. (iii) Parents and practitioners cautioned that screening may increase parental anxiety and lead to unnecessary referrals. Practitioners countered this with examples of cases not recognised by parents. (iv) Participants questioned the value of earlier identification of problems without effective and accessible therapeutic pathways.
Conclusions:
For programmes to be effective, parents need to be reminded of the benefits of early intervention and encouraged to attend preventive health appointments. Practitioners require further training and tools specific to the primary care setting. Further investment in specialist and allied health services is considered essential to assure better outcomes for young children’s mental health following screening and referral. Practitioners welcome a more collaborative relationship with other professionals (e.g. early educators) in assessing children’s social and emotional development. General practice has the capability but requires a more structured approach to assessing the social and emotional health of young children.
Background and aims
At least 14% of Australian children aged 4–17 years have mental health problems (Sawyer et al., 2001) and 20% of 5-years-olds have clinically significant behavioural problems (Robinson et al., 2008). Effective preventive interventions for behavioural and emotional problems have been successfully applied to preschool children (2- to 3-year-olds) in the Australian context; however these interventions depend on early detection via universal screening in the primary care setting (Bayer et al., 2009).
General practitioners (GPs) are well placed to assess and manage child mental health problems (Vallance et al., 2011), but whilst 12% of GP contacts are with children (Britt et al., 2011), explicit social and emotional problems account for just 2.6% of these visits (Charles et al., 2011). Efforts have been made to increase GPs’ identification of mental health disorders with children (Brown and Wissow, 2010; Sayal and Taylor, 2004; Zwaanswijk et al., 2005) but little is known about how Australian practitioners view screening for social and emotional problems. US data found primary care paediatricians embraced the use of standardised screening tools for developmental and behavioural problems, but raised concerns about which instruments to choose, the need for additional time to screen, and the lack of referral services for identified problems (Tanner et al., 2009).
International research also identified that parent satisfaction with preventive healthcare services centred on the age of the child and the parent-provider relationship (Radecki et al., 2009; Roche et al., 2005). US parents regarded the social and emotional health of their children as an important indicator of school readiness (McAllister et al., 2005), but did not always recognise child behavioural or emotional problems as mental illness (Pescosolido et al., 2008) and therefore did not necessarily express concerns when attending their physicians (Sayal and Taylor, 2004; Sayal et al., 2006).
Australia’s universal child health surveillance system is conducted through local council child and family health nurses (CFHN), with state-based variations in policy and service provision (Schmied et al., 2011). In Victoria use of CFHN services decline as the child gets older, with less than 60% of children completing the final visit scheduled at 3½ years of age (Moore and Grove, 2008).
To counteract this decline ‘The Healthy Kids Check’ (HKC), a one-off health check aimed at preschool children, has been available since 2008. Administered by practice nurses (PNs) and GPs, the HKC comprises mandatory and non-mandatory components to assess growth and development, and offers opportunities for health promotion (Figure 1). The HKC is meant to function as an initial screening test, from which children identified with problems can be referred on for diagnostic testing. Proposals to include the assessment of a child’s social and emotional development and bring the check forward, from 4 years of age to 3 years (Roxon et al., 2011) have been strongly contested (Frances, 2012). However, overall the uptake of the HKC has been low, for reasons currently unknown (Medicare Australia, 2011). It is therefore opportune that the perceptions of practitioners and parents about preventive health care for children in general and mental health screening tests in particular, be explored.
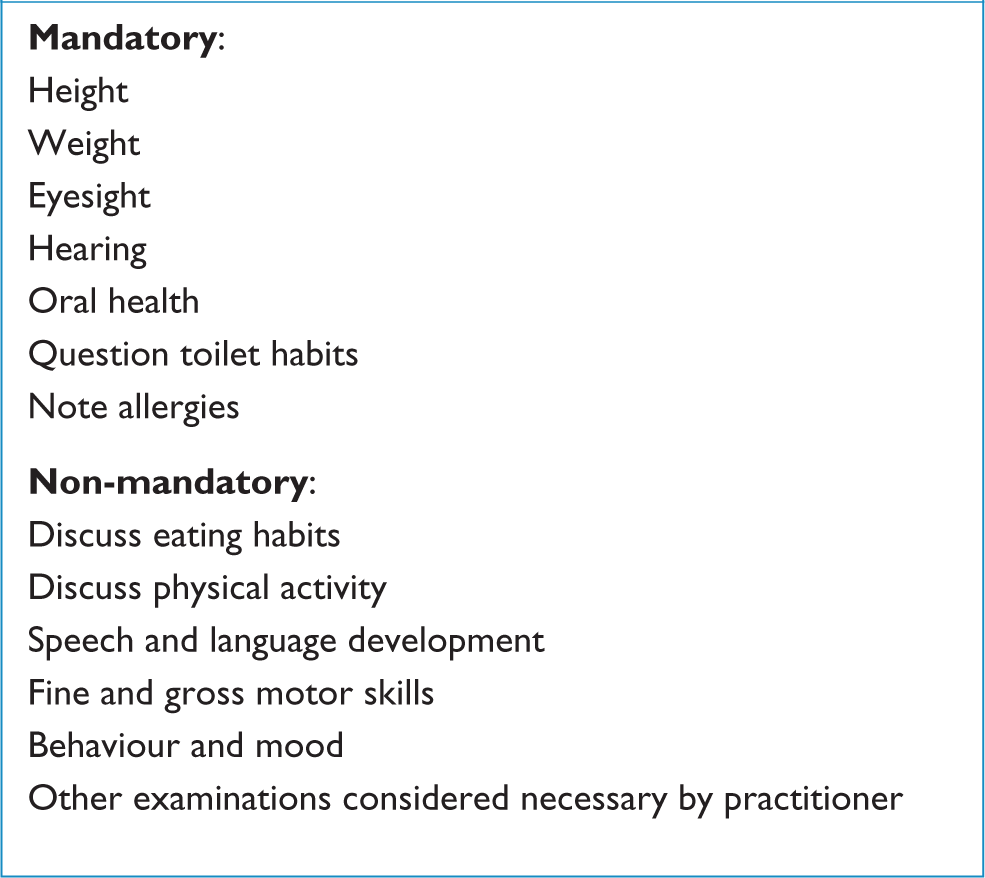
Components of the current Healthy Kids Check.
The aim of this study was to understand parent and practitioner views regarding screening for social and emotional health problems in the context of preventive health care for young children.
Methods
Three socioeconomically and culturally diverse areas of Melbourne, serviced by the Bayside (high socio-economic); Westgate (low socio-economic) and Dandenong-Casey (culturally and linguistically diverse) Divisions of General Practice, were chosen as the setting for our study. The third suburb was targeted to ensure the sample included the opinion of parents living in Australia for less than 10 years, as it was expected that their experience of accessing preventive health care could be different from parents who had either resided in Australia all their lives or acculturated to the Australian way of life.
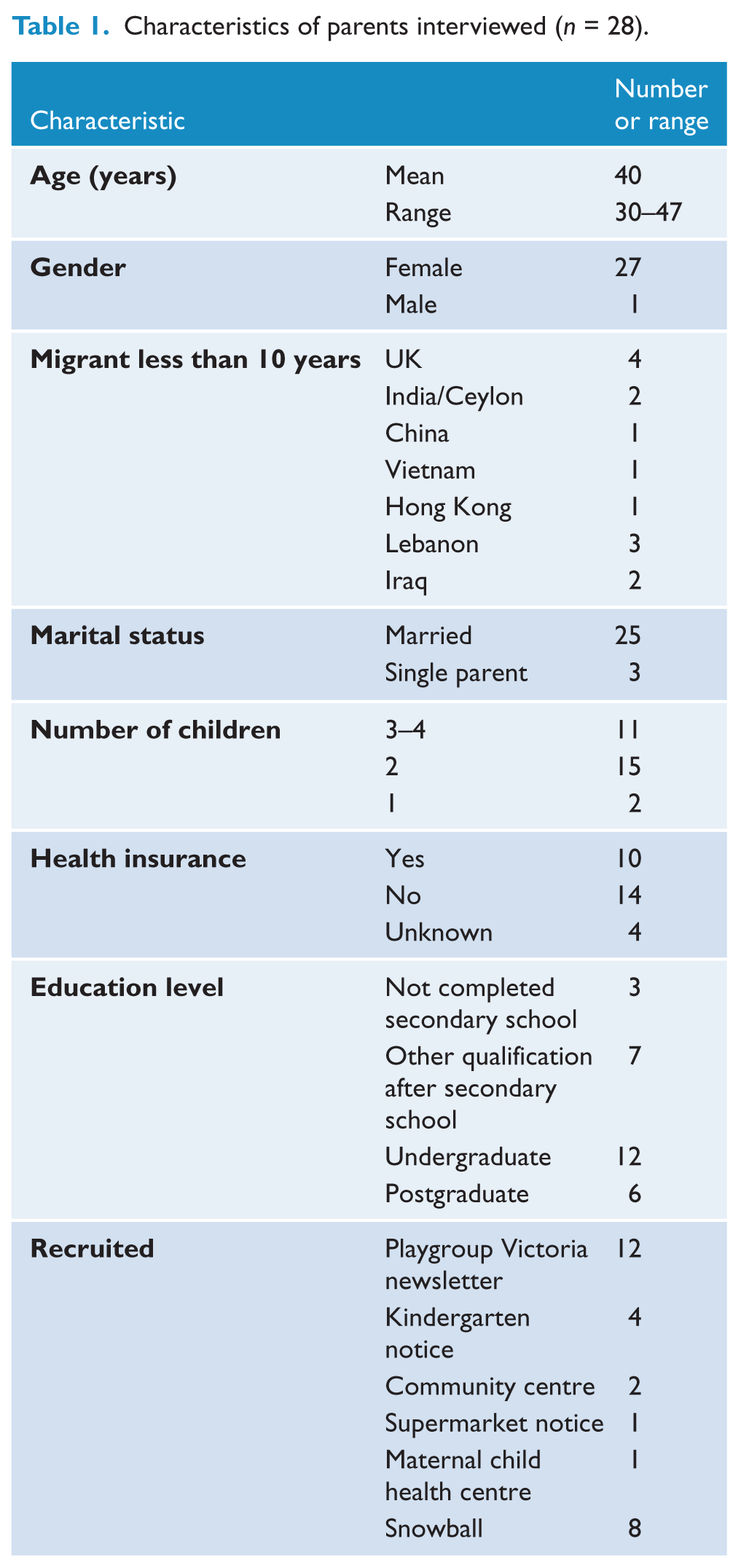
Parents were recruited from the community using flyers placed in settings likely to be frequented by young children and their parents (Table 1). Additional participants were recruited through snowballing. Participants were selected if they parented at least one child between the age of 3 and 5 years, spoke English, and had resided in Australia for more than 12 months. Telephone interviews, using a semi- structured questionnaire, were conducted between May and July 2011, with each interview lasting approximately 45 minutes. Topics covered child developmental health (e.g. growth, vision, hearing) and social and emotional health, perceptions of preventive health and health-seeking (Figure 2). Recruitment was stopped when data saturation was achieved.
Characteristics of parents interviewed (n = 28).
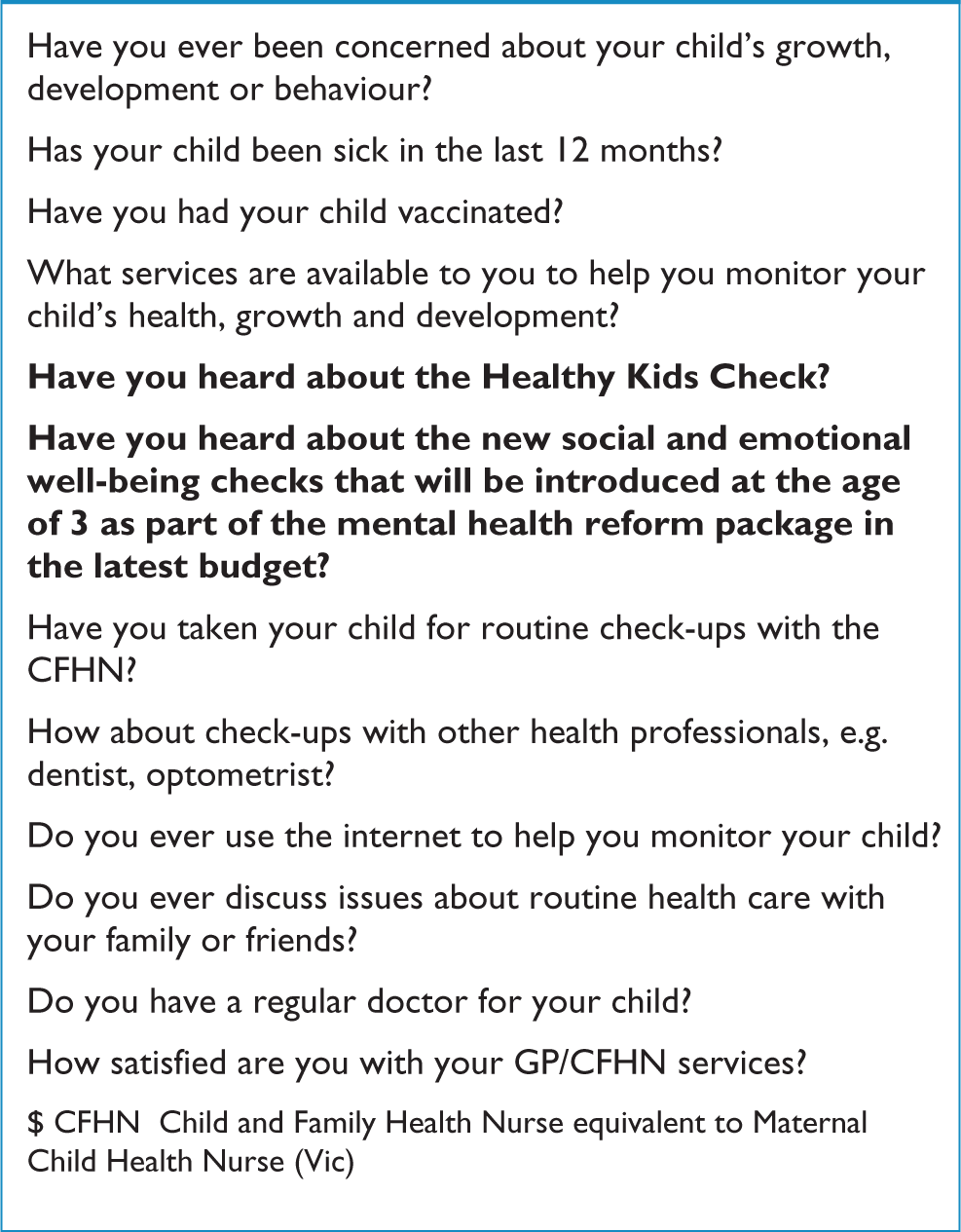
Sample of parent interview questions.
GPs and PNs were recruited through advertisements placed by the three Divisions of General Practice (now known as Medicare Locals). Three GP and three PN focus groups (5–10 participants) were conducted, two groups in each Division area, between June and October 2011. Discussion was facilitated by one researcher (KA), with notes taken by a second researcher (BB). Questions related to current provision of preventive health care to young children, including HKCs, and the anticipated changes in social and emotional health assessments (Figure 3).
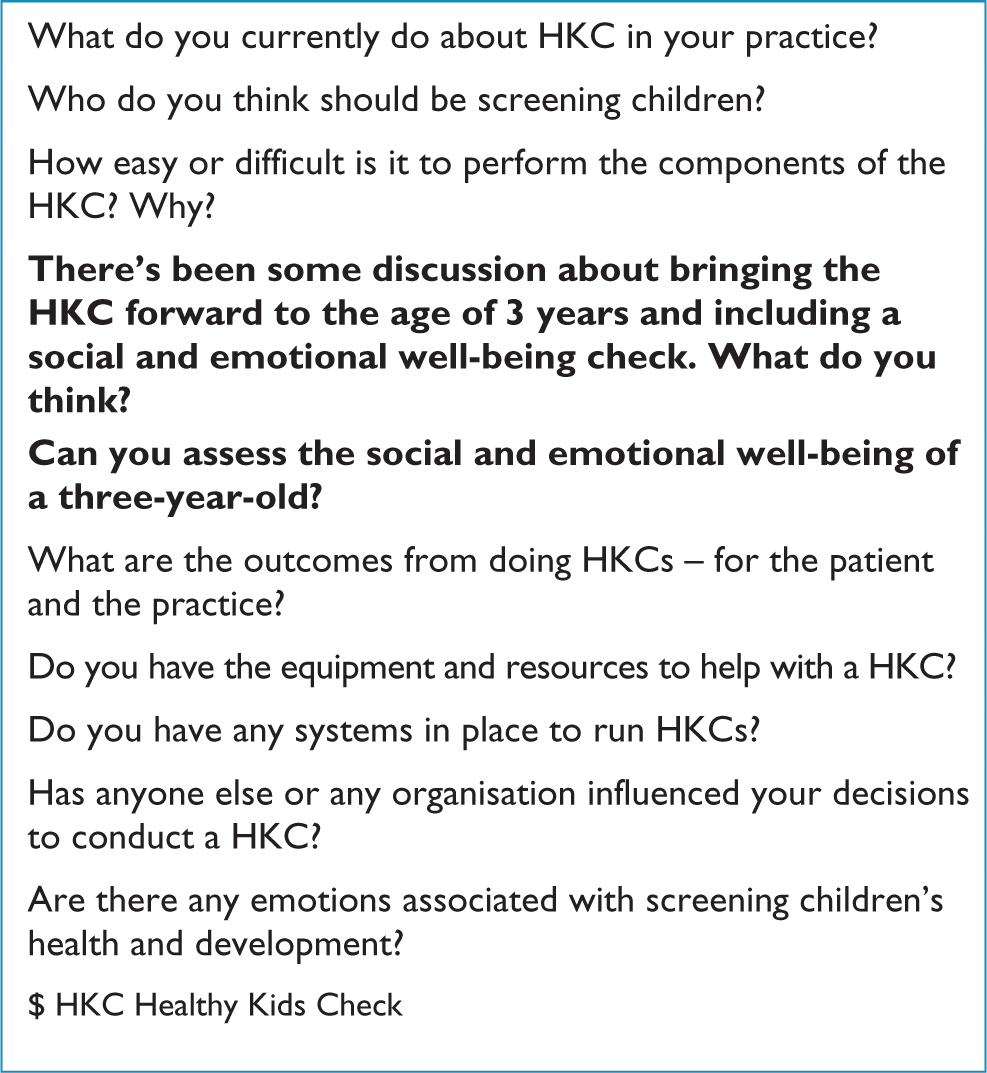
Examples of prompts for focus groups with practitioners.
Following signed consent, interviews and discussions were audio-recorded and participants were offered gift vouchers (parents $75, PNs $80, GPs $200). Approval was obtained from the Monash University Human Research Ethics Committee.
Data analysis
Verbatim transcripts were read repeatedly to gain familiarity with the data. Two researchers (KA and BB) independently coded the data and proceeded with a thematic framework analysis: key topics were identified, previously coded data were revised, in an iterative process to maintain quality within the data (Braun and Clarke, 2006; Green et al., 2007). Over several meetings, results were discussed and consensus was achieved, with a third researcher (DM) resolving differences and overseeing the linking of codes into categories. NVivo 8 software (NVivo, 2008) was used for coding and to aid analysis. All data were de-identified and pseudonyms applied to parents’ reports to maintain anonymity. For the purposes of this study, data which related to the assessment of a child’s social and emotional health, learning difficulties, behavioural problems, and developmental disorders, were coded ‘social and emotional developmental and mental health’.
Results
Twenty-eight parents were interviewed, with a mean age of 40 years; only one participant was male (Table 1). Ten participants were from culturally and linguistically diverse (CALD) communities. Twenty-two GPs (12 female; 10 male) and 18 PNs (all female) participated in discussions each lasting two hours. Four common themes were identified when the social, emotional, behavioural and mental health screening of young children was considered:
Current thinking about social and emotional health.
Capabilities of practitioners.
Challenges associated with the outcomes of screening.
The strategic benefit of labelling and access to services.
Current thinking about social and emotional health
Parents were conscious of their child’s social and emotional development and described their children’s personalities in terms of their ability to form friendships. Although they recognised this as being intrinsic to their child, they also believed that exposure to child care would help them overcome socialisation difficulties, and reduce separation anxiety, and this was seen as important preparation for school.
“She finds it quite easy to interact socially and maybe that’s because she went to child care when she was quite young, and she’s always kind of been around other children, and she’s not really the shy type.” (Belinda, 40 years, Bayside, two children)
Although generally receptive to the proposal to screen the social and emotional well-being of young children, the predominant belief among parents was that an assessment at the age of three was too early in the child’s development.
“But can they really identify mental health problems at the age of three?” (Anne, 41 years, Westgate, three children)
“Their social and emotional well-being is the big issue I think when they reach that school age.” (Justine, 42 years, Bayside, three children)
In contrast, amongst practitioners, although there was debate about the ideal age of screening, the need for early intervention, well before the age of four years, was recognised as crucial:
“I think that they should be screened at a younger age. I think that four is absolutely ludicrous. I think the ideal time is 12 to 18 months for anything to have any chance of reducing morbidity later on and the social implications and the consequences of those developmental disabilities.” (GP 1, Bayside group)
Parents and practitioners raised concerns that a one-off assessment would not accurately gauge children’s social and emotional health, with daily mood variations, temperament and the clinic environment all likely to influence behaviour.
“Well, it all comes down to the child and how comfortable they are because children can change on any given day and I think some are confident in any new surroundings and with new people and some aren’t.” (Natalie, 39 years, Bayside, two children)
“You’ve got a child who is not necessarily, because you’ve just given them immunisations, not really interacting with you.” (PN 1, Bayside group)
Practitioners discussed the ‘child within the family constellation’, the interplay between child temperament, family dynamics and social environment, which was felt to complicate the assessment of a child’s social and emotional health. They wondered if the frequency of ‘stand-alone’ social-emotional health issues justified screening for them.
“How many are just a reflection of poor socio-economic, or household issues? So I’m sure there are three-year-olds with mental health issues and fantastic families and parents, but I would have thought that was an incredibly small amount.” (GP 1, Westgate group)
Two practitioners (Dandenong GP 1 and Bayside PN 2) thought parents would be reluctant to disclose information about their child’s social and emotional development in case it reflected on their parenting skills and could cause a child to be removed from their care. This belief was not expressed by this group of parents, though they recognised that family conflict such as parental separation (3/28) could have negative social and emotional outcomes and could cause behavioural problems in their children. Those affected sought services to help with these.
“When they were little … my wife and me, including the grandparents we always have conflict, we always sort of fight, you know. That might have impacted on [my daughter].” (Li, 44 years, Dandenong, two children)
“Last year when my relationship broke down and I took [my son] there because I had concerns for him on his emotional … health and wellbeing. I asked her … to advise me how I can look after my child.” (Tien, 30 years, Dandenong, one child)
Capabilities of practitioners
Both practitioners and parents questioned the practitioners’ capabilities. Parents were uncertain that general practice personnel were skilled enough, or had enough time, to identify social and emotional disorders in young children, while PNs expressed a universal need for extra training.
“I just can’t imagine my regular GP really having that much specialist information or knowledge about that kind of thing … I don’t know, it seems like a bit of a stretch .….” (Claire, 42 years, Westgate, two children)
PN 1: “It would be such a no go zone for me personally… I think it is absolutely terrifying. It would be well out of my depth, anything to do with the psychology of a three-year-old.” (PN 1, Bayside group)
Although GPs were generally more positive than PNs about their capabilities, undertaking developmental assessments was met with mixed responses and varied according to specific skills acquired during training. Reservations were expressed about making specific diagnoses.
“I like seeing children but I’ve never been so great at the whole developmental scheme of things … The Denver Scale, I really am terrible at it.” (GP 2, Westgate group)
“I suppose there are quite a number of … kids with autism to do … an emotional check. [But] are we qualified to do it? Are we really qualified to do it? … I wouldn’t even make the diagnosis … of dementia, in patients that I’m almost certain have dementia, without going through a team of people, let alone diagnosing emotional problems in children. I think we should defer to professionals well trained in this.” (GP 2, Dandenong group)
The development of appropriate tools to assist screening was also widely discussed. Tools were seen as likely to increase efficiency and efficacy, as it was deemed important that cases should not be missed. Further, practitioners believed they would help set a minimum standard between practices.
“Rather than just saying, ‘Assess their emotional wellbeing.’ Give us the tool … a tool that everybody can use, the same tool, because if we’re all doing it separately then where’s the base to start from? I think we need to all be doing a similar emotional well-being check for it to be of any value.” (PN 1, Dandenong group)
Several members from one group of GPs had recently attended a presentation about autism and were optimistic that screening for this was practicable. In general, however, practitioners were not routinely applying behavioural screening questionnaires and only one PN had used the Parents’ Evaluation of Developmental Status questionnaire (Glascoe, 2010). The cost of questionnaires was an additional barrier cited.
Whilst some parents recognised social and emotional health screening as being the domain of the CFHNs, GPs and PNs held conflicting views about which health practitioners should conduct screening. PNs suggested that because CFHNs’ entire focus was early childhood, they would be better placed to do this, but GPs regarded a shared role as more helpful. GPs also discussed a possible role for external agencies, such as early childhood educators. They judged that a child with a social developmental problem would be more easily identified in a group situation by a professional who saw them on a regular basis.
“If you want to know if a child is ready to go to school the best people to judge that is … actually the kinder teacher … not the parents, it’s the kinder teacher, seeing the kids and their peers. Just from having the experience of going to kinder and seeing how the kids interact in a group and how easy it is to see who is a bit strange, I was thinking … wouldn’t it be more efficient to use the resource of kinder and day-care centre to kind of get a foot in there.” (GP 2, Bayside group)
Challenges associated with the outcomes of screening
The context of screening for social and emotional health problems was also viewed as problematic when it came to considering the outcomes of those assessments. The Dandenong GP focus group were fearful that screening would open ‘a can of worms’, and one GP, who worked with severely disadvantaged groups, was concerned that this would increase reporting to social services and lead to conflict between parents and practitioners. This view was concurred:
“So if we over investigate it, over discover trouble … we create a medical and social monster.” (GP 3, Dandenong group)
PNs were particularly concerned about being the ‘bearer of bad news’ if they suggested to a parent that something may be wrong when screening children.
“I don’t feel comfortable sometimes with probably talking to parents if there’s issues. It’s quite daunting … parents don’t like to hear that something’s wrong with their child.” (PN 2, Dandenong group)
Both parents and practitioners worried about the consequences of diagnosing a normal child as having a problem and unnecessarily raising parental anxiety. The stigma associated with a diagnostic label and the possibility that a child would be treated differently once a label was applied, leading to secondary changes in the child’s behaviour, were additional concerns.
Some GPs felt pressured to refer for a second opinion to “appease parents”.
“Well educated parents – they’ve already got a bit of information… saying that my child has got this, got that, can you have a look at my child, [does my child have] ADHD or something like that … Then you ask the child … [No] signs of ADHD. But the parents are trying to insist something, so [I have] to send them to the paediatrician.” (GP 3, Westgate group)
On the other hand, practitioners also recounted experiences of parents who failed to realize, or apparently denied their children had problems:
“I picked up a little boy who obviously had anxiety disorder just by the fact he had these … hand movements and stuff like that. And mum would just say, ‘I just thought he was a bit shy’.” (GP 1, Bayside group)
The strategic benefit of labelling and access to services
Whilst parents with children who did not have diagnosed disabilities were concerned about inappropriately labelling children, for families who were dealing with these problems, the diagnosis was met with relief. Julia, whose son had not been diagnosed with Asperger’s until the age of ten, said:
“This child … he’s been a very tricky child pretty much all his life. A very challenging child to have to parent, and I’ve struggled with it for a long time … He saw a psychologist at school … she thinks he has Asperger’s and he makes up rules for himself about things. And since then I’ve read a little bit about Asperger’s and I’m going, ‘Oh, the penny is dropping! Oh this is so familiar.” (Julia, 41 years, Westgate, three children)
Three families, including Julia’s family, had experienced developmental problems that presented as learning or social disorders in school, despite difficulties being apparent for years beforehand. Their stories reflected a ‘journey’ to comprehend their child’s behaviours, and the label was viewed as necessary to access funding and help.
However, the relief of the diagnosis was eventually replaced with feelings of frustration and dismay as they encountered difficulties and significant costs in accessing services. Personnel changes, insufficient and delayed appointments for services such as speech therapy, psychiatry, psychology and paediatrics were reported. Both parents and practitioners questioned the worth of screening when referrals and outcomes could not be guaranteed.
“We waited out that six or seven months and then instead of getting the appointment we got a letter saying, due to cutbacks, they’ve had to reassess their waiting lists and they’re not going to offer [our son] that two day assessment … he just got bumped off the waiting list … So … we saw an educational psychologist and had a four hour assessment that cost $1100 which we can’t claim back … It’s been a very expensive process … All we got from that appointment [was] ‘[this child] has severe dyslexia’. It didn’t really give us a pathway or a way ahead. So you kind of have the relief of going, ‘Thank God we know what’s wrong’ but then you go, ‘Well what do we do?’.” (Elisabeth, 44 years, Westgate, two children)
“I’ve just had a few of these ‘query autistic’ kids come back and you look at them and you think, ‘Oh yes, maybe a bit dodgy, I don’t know’. And then they go off for their early intervention which is one hour of play therapy a week. That’s not going to cut it.” (GP 1, Westgate group)
Discussion and implications for practice
Parents were highly concerned about the social and emotional health of their children and regarded this as an essential component of preparation for school. This reflects the findings of McAllister et al. (2005), where lower-income US families emphasized social and emotional health as important to facing the challenges of the school environment. Australian parents might therefore be quite receptive towards this aspect of developmental assessment.
Parents and practitioners had common concerns about social and emotional health assessments proposed in changes to the HKC. Whilst practitioners were well informed about problems facing young children, parents were less knowledgeable, and did not always appreciate the need for, early intervention for which there is now a significant evidence base (Kowalenko, 2012). For screening programmes to be effective, parents would need to be reminded of the benefits of early intervention and encouraged to attend preventive health appointments.
The capability of practitioners was questioned by both parents and practitioners. Parents usually assigned screening for social and emotional problems to CFHNs, recognising that time pressures in general practice may inhibit engagement. Practitioners did not apply behavioural questionnaires even when they conducted developmental assessments in their practice. Reasons for this are unknown but cost barriers were identified as one factor. An Expert Committee, appointed to oversee the development of the new ‘three-year-old HKC’, has been tasked with developing a training programme for GPs (Department of Health and Ageing, 2010). This is likely to be welcomed by practitioners, as this study identified training as a major need of both GPs and PNs.
Similarly, the development of tools which can be effectively applied within the tight time constraints of primary care are seen as fundamental for successful implementation. Concerns regarding training deficits and problems with screening tools were also widely articulated by paediatric physicians in a large US study of contemporary needs in “well-child care” (Tanner et al., 2009). Our study also identified that training programmes would also need to consider practitioner interpersonal skills with regard to the delivery of screening programmes and communication of findings to parents, as this was seen as a barrier for PNs in particular.
The reluctance expressed by some practitioners to undertake social and emotional developmental screening is reflected in the general debate surrounding prevention in primary care which centres around competing demands for practitioner time (Russell, 2005). Practitioners justifiably feel overwhelmed by an ever-expanding array of preventive activities (Yarnall et al., 2003) so it was perhaps natural that they considered other professionals could be involved in developmental assessments. Early-childhood educators already make assessments of children to determine their school-readiness. Those children found not to be school-ready may benefit from referral to general practice for developmental assessment. Part of a government ‘roadmap’ towards structural reform of the Australian mental health system includes partnerships between health and education as key to prevention and early intervention. Medicare Locals, primary healthcare organisations recently established to respond to local healthcare needs, are ideally placed to facilitate such partnerships (Davies, 2010). The US study (Tanner et al., 2009) also highlighted deficiencies linking private practice to community resources and speculated how integration could change existing surveillance and management of developmental and behavioural problems.
Significant waiting periods and large financial barriers made earlier detection ineffectual and frustrated practitioner and parent alike. Expansion of programmes which utilise public-private partnerships would alleviate demand and would increase the flexibility of services, particularly if children could access treatment according to need and before diagnostic labels have been applied. This has been argued for by Wissow et al. (2011), who advocate a “common factors approach to treatment” of children with behavioural and emotional problems, in primary care, so that a core set of interventions is commenced when socio- emotional or behavioural problems arise, and more specific treatments are accessed as diagnoses are refined. Currently, access to services before diagnosis is limited but early initiatives like ‘Playconnect playgroups’, available to children with autism and autism-like disorders, reflect a start (Playgroup Australia).
Limitations of the study
The opinions of GPs, PNs and parents who self-select for a study will not be representative of all practitioners, nor be generalisable to an entire population. It is likely that these practitioners are already more engaged in child health. Future research could target younger parents and rural communities, populations which are likely to face additional barriers when seeking preventive care and mental health services, as well as gauge the opinion of early childhood educators in taking on social and emotional assessments.
The strengths of the study are in the corroboration of opinions by parents, GPs and PNs across a wide socio- cultural spectrum. This study replicates findings from a US study (Tanner et al., 2009). Our conclusions provide an important foundation if future interventions aim to increase the delivery of social and emotional preventive health care to young children.
Conclusion
The recent debate regarding introduction of the 3-year-old check has highlighted general issues associated with screening programmes – especially the identification of false positives – with attendant risks of medicating and stigmatising normal children, and raising parental anxiety (Frances, 2012; Jureidini and Raven, 2012; Levy, 2012; Newman, 2012; Prior, 2012; Toumbourou, 2012). This was a concern underscored by both parents and practitioners, but for those parents who had experienced years of anguish before obtaining diagnoses of developmental disorders, the ‘application of the label’ was viewed more positively. GPs have always had a role in the developmental assessment of children, and have learned to incorporate assessments of parents’ mental health, parenting style and attachment issues, and remain mindful of the potential for child abuse (Royal Australian College of General Practitioners, 2011). Broadening this to include more specific aspects of social and emotional development is not beyond their brief, but could benefit from a more structured approach, supported by community collaborations, so that parents are able to provide the best opportunities for their young children’s learning, social and emotional well-being and development.
Footnotes
Funding
This research was supported by a research grant from the Shepherd Foundation.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.