
Abstract
Objective:
A small subgroup of patients is primarily responsible for the large number of aggressive and violent incidents in psychiatric inpatient units. This study aims to identify the developmental, social and interpersonal histories of repeatedly aggressive patients in order to better understand their treatment needs.
Methods:
A total of 1269 consecutive inpatients were studied over 18 months, identifying 64 who were repeatedly aggressive; 128 non-aggressive patients were randomly matched to the aggressive patients by age, sex and diagnosis. Developmental, social, interpersonal and familial histories were obtained from a chart review.
Results:
Repeatedly aggressive patients were significantly more likely to have had a history of aggression, physical and sexual abuse, and experienced interpersonal problems and parental divorce.
Conclusions:
Aggressive patients do not just need short-term skills training, but interventions that target interpersonal and personality disorder deficits associated with their developmental histories.
Introduction
A small number of patients in inpatient mental health facilities are responsible for a disproportionately large number of aggressive incidents (Barlow et al., 2000; Grassi et al., 2006; Kraus and Sheitman, 2004; Lussier et al., 2010; Saverimuttu and Lowe, 2000). Although recent studies have explored factors relating to aggressive acts in inpatient samples (Carr et al., 2008; Cornaggia et al., 2011; Ilkiw-Lavalle and Grenyer, 2003; Ketelsen et al., 2007; Papadopoulos et al., 2012), fewer have comprehensively studied the characteristics of those who are repeatedly aggressive. A handful of older studies have described the demographic, clinical and admission characteristics of repeatedly aggressive mental health patients (Barber et al., 1988; Cheung et al., 1997; Convit et al., 1990; Krakowski and Czobor, 1994; Krakowski et al., 1989a, 1989b; Owen et al., 1998; Saverimuttu and Lowe, 2000); however, few studies have studied the historical risk factors of these patients in comparison with non-aggressive patients. One recent study (Lussier et al., 2010) explored the sociodemographic and the legal and psychiatric history of repeatedly aggressive patients compared to non-aggressive patients in a forensic inpatient sample and found that prior legal problems (violent and other), early onset of mental illness and prior hospitalisations were associated with repeated aggressive incidents. Studies designed to investigate social, developmental and familial history of repeatedly aggressive patients will enable a better understanding of these patients and may assist in the development of specific and tailored interventions.
The purpose of this research was to investigate the differences in the social, developmental and familial history of repeatedly aggressive patients compared to matched, non-aggressive, control patients in a psychiatric inpatient setting in order to better understand their treatment needs.
Materials and methods
Patients
Consecutively admitted inpatients (n = 1269) were studied over 18 months, identifying 64 who were repeatedly aggressive. The 64 aggressive patients were then matched to 128 control patients from the larger inpatient sample. All patients in the sample (n = 1269) who were the same sex, age and diagnosis as the 64 aggressive patients and who had never been involved in an aggressive incident were eligible for the control group. The final 128 controls were randomly selected from all eligible patients and it was ensured that all aggressive patients had two matched non-aggressive controls. The aggressive group were identified as patients who had demonstrated two or more aggressive incidents within the 18-month study period (the average number of incidents per aggressive patient was 3.75). The research was approved by the Institutional Review Board and written signed consent was obtained by participants.
Procedure
The patients studied were admitted into psychiatric inpatient units during the 18-month study period from the Illawarra region of NSW, Australia – a population catchment area of about 430,000 (2008–2009) (Australian Bureau of Statistics, 2010). Four inpatient units operated within the same Area Health Service. Three of the units were acute, and one was a subacute rehabilitation unit. Of the three acute units, one was a high-dependency locked unit for acutely disturbed patients, one was a secure unit for both acute voluntary and involuntary patients, and one was a secure unit for patients with less severe problems. Because transfer between units was common, separate analyses on aggression by unit could not be made and incidents occurred across all units. Data on aggressive incidents were obtained prospectively using an incident report form, as they occurred. Data on patient demographics, and developmental, social and familial histories were obtained retrospectively by chart review using a specifically designed coding form developed to record variables that had been previously identified in the literature and other variables identified as potentially important by the research team. Aggression was defined in this study as all behaviours involving physical and verbal aggression displayed by patients against themselves, others or property, irrespective of outcome (Barlow et al., 2000).
Chart review
Demographics and service utilisation
The demographic and service utilisation data recorded included current age and age at first admission, marital status, number of children, employment status, country of origin, years of education, number of social supports, number of people residing with, and the number of consultations over the study period with psychiatrists and allied health staff (i.e. psychologists, social workers and occupational therapists).
Aggressive incidents
The Aggressive/Assaultive Incident Report Form (Barlow et al., 2000) was used by staff following an aggressive incident. Information recorded on the form included patients’ admission status (i.e. voluntary or admitted under the Mental Health Act, 2007) level of care received during the incident (i.e. under constant supervision, routine visits by staff) and details about the incident (type of behaviour, causal factors, use of weapons, intervention and damages). The incident report form was developed as part of the organisation’s commitment to the reduction of violence in the units. Thus, completion of the form was mandated by management as a compulsory report on all forms of aggression. As such the compliance rate was high, and on-going staff support and debriefing ensured that all recorded incidents of aggression were reliably made at the time of the incident (not retrospectively), giving confidence in the reliability and validity of data.
Developmental, social and familial history
Developmental history variables included history of physical abuse and/or sexual abuse, substance use, adoption, learning difficulties, adolescent pregnancy, serious physical accidents, poor physical health and any suicide attempts. Social history variables included history of legal problems, aggression, placement in foster care and/or juvenile justice centres, relocation from country of origin and interpersonal difficulties with family, friends or acquaintances. Familial (parental and sibling) history variables included drug and alcohol use, psychiatric history, detainment in an adult correctional facility, parental divorce and death of a parent or sibling. Selection of the variables was based on review of the literature and what had previously been hypothesised to have an impact on aggressive acts.
Data analysis
Because the chart review was performed by two researchers, Cohen’s kappa was used to calculate inter-rater reliability on a subset of 20 cases. Inter-rater agreement between the two raters on social, demographic and familial items was excellent (Cohen’s κ = 0.91, p < 0.001). Descriptive statistics report the sociodemographic, diagnostic and service utilisation characteristics of the aggressive and control samples, along with the nature, causes and intervention for aggressive incidents. Sociodemographic, service utilisation and social, development and familial characteristics are compared using odds ratio (OR) analyses and comparison of means tests at an alpha level of 0.05.
Results
Demographics and service utilisation
Patients were matched according to sex, age and diagnosis, with sociodemographic and diagnostic characteristics of aggressive and control samples presented in Table 1. Comparisons of means and chi-squared analyses did not yield any significant differences at an alpha level of 0.05 in other sociodemographic variables including age at first admission, number of children, years of education, total number of social supports, country of origin, marital status, employment status and living arrangements.
Demographic and diagnostic characteristics of repeatedly aggressive (n = 64) and non-aggressive (n = 128) patients.
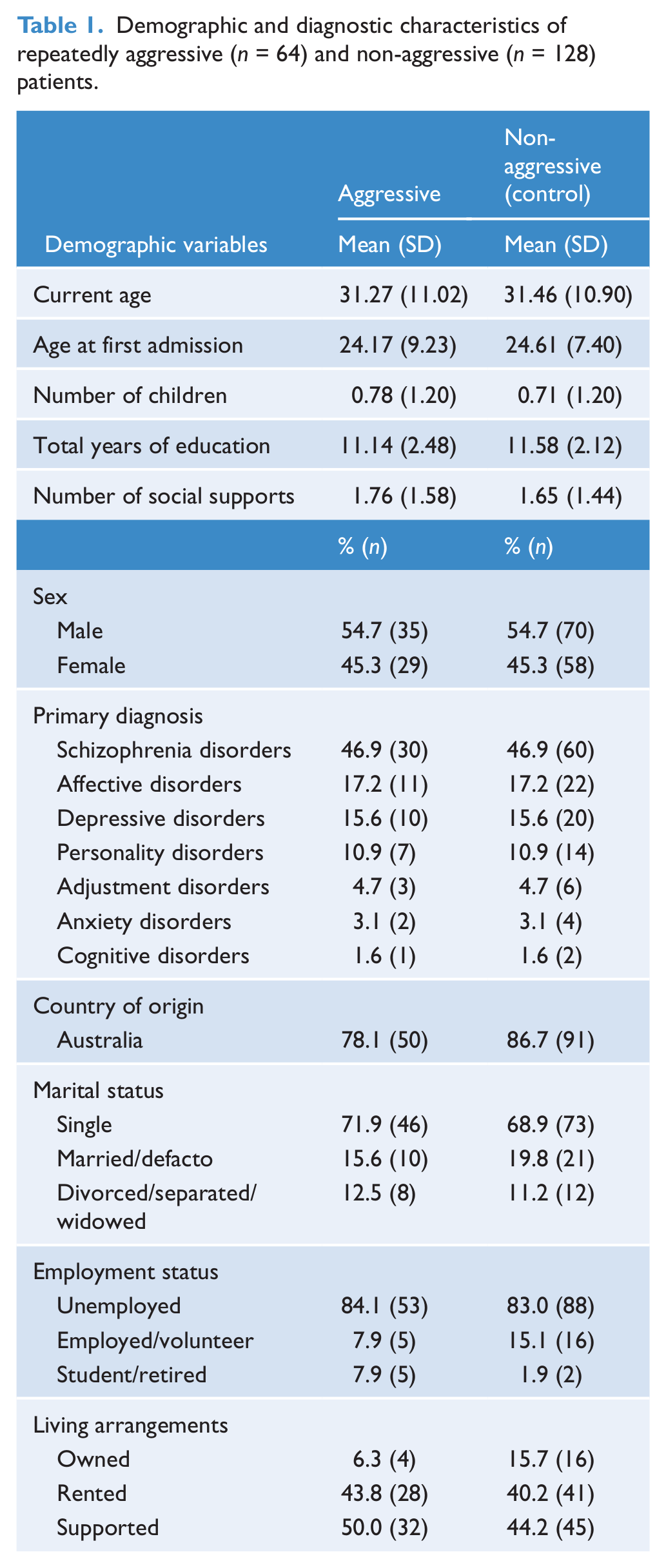
The mean length of stay per admission for the aggressive patients (M = 17.69, SD = 16.05) was significantly higher (t = 3.26, p < 0.001) compared to the control patients (M = 10.34, SD = 10.51). Repeatedly aggressive patients also had significantly more consultations (M = 11.35, SD = 9.08) with psychiatrists (t = 3.37, p < 0.001) than controls (M = 7.12, SD = 5.52). There were no significant differences between aggressive and control patients on the number of consultations with other allied health staff. Odds ratios with 95% confidence intervals (CIs) were conducted between male and female aggressive patients for the significant variables found for developmental, social and familial histories.
Aggressive incidents
When the incident occurred, repeatedly aggressive patients were usually involuntarily detained under the Mental Health Act, 2007 (76.0% of the time; 62.5% were scheduled and 13.5% of the time they were classified as temporary patients under a legal order made by a magistrate). Another 22.9% of the time, repeatedly aggressive patients were voluntary patients, and 1.1% of the time they were admitted because they had failed to comply with a community treatment order. Half of the incidents occurred during the day (50.0%), with 33.3% in the afternoon and 16.7% at night. Almost two-thirds of incidents (65.3%) occurred while repeatedly aggressive patients were under 15-minute interval observations by staff, 20.0% when they were under 30-minute observations and 14.7% when they were under 60-minute observations.
The total number of aggressive incidents by repeatedly aggressive patients was 236 (mean per patient = 3.75, SD = 2.54). Most of these incidents involved physical aggression (81.3%), while 18.7% involved only verbal aggression. Out of all aggressive incidents, 56.7% were addressed towards staff, 15.6% towards other patients, 14.4% towards themself and 13.3% towards objects. Interestingly, 36.7% of females in the aggressive group engaged in at least one self-harming incident, whilst only 14.7% of males did: OR = 3.36 (CI = 1.01–11.21, p = 0.04). A total of 10.5% of incidents involved weapons such as knives, forks, chairs, razorblades and cords obtained from pyjamas or dressing gowns, and had resulted in damage to property 15% of the time. Injuries during the incidents occurred 21% of the time – to themself (9%), visitors (6%), staff (4%) or other patients (2%). Almost 42% (41.9%) of the aggressive acts were managed by intramuscular injection. Other management strategies included an interpersonal approach involving negotiations with the patient (31.2%), the administration of oral medication (12.9%), seclusion (6.5%), physical evasive techniques (3.2%), the administration of an intravenous injection (3.2%) and physical restraint (2.2%).
As recorded by staff on the Aggressive/Assaultive Incident Report Form, the most frequently cited cause of the aggressive incidents was the current experiencing of psychotic symptoms (64.5%). Other causes included involuntary detainment, general personality characteristics, confinement, not wanting to take compulsory medication, family issues and substance abuse.
Social, developmental and familial characteristics
The results presented above suggest that aggressive patients tended to spend more days in each admission, and were also more likely to have social, developmental and familial problems. This might lead to the hypothesis that length of stay is a function of the problems experienced, and subsequently the frequency of aggressive incidents is positively associated with the length of stay in the unit. In addition, a longer length of stay would increase the opportunity for aggression to be detected. Thus, to test this hypothesis, three regression analyses were performed to determine whether certain social, developmental or familial variables predicted length of stay.
Findings from the regression analyses suggested that length of stay is modestly, albeit significantly, affected by the following variables: history of sexual abuse; placement in foster care; placement in juvenile justice; divorced parents. Thus, to some extent, the social, developmental and familial variables influence length of stay. To control for this, we controlled for length of stay in analyses. Table 2 provides the proportion of and ORs of recidivists and non-recidivists who have experienced the developmental, social and familial variables listed, after accounting for the confounding variable of length of stay. For five of the 20 variables, the cell count for either group was zero (adolescent pregnancy, experiencing a serious physical accident, history of legal problems, placement in a juvenile justice centre and having parents who were/are in gaol), and thus ORs could not be calculated for these variables. Other findings of variables with small cell values should also be interpreted with caution.
Odds ratios (ORs) and 95% confidence intervals (CIs) for developmental, social and familial variables in the prediction of repeated aggression on inpatient mental health units compared to matched control inpatients.
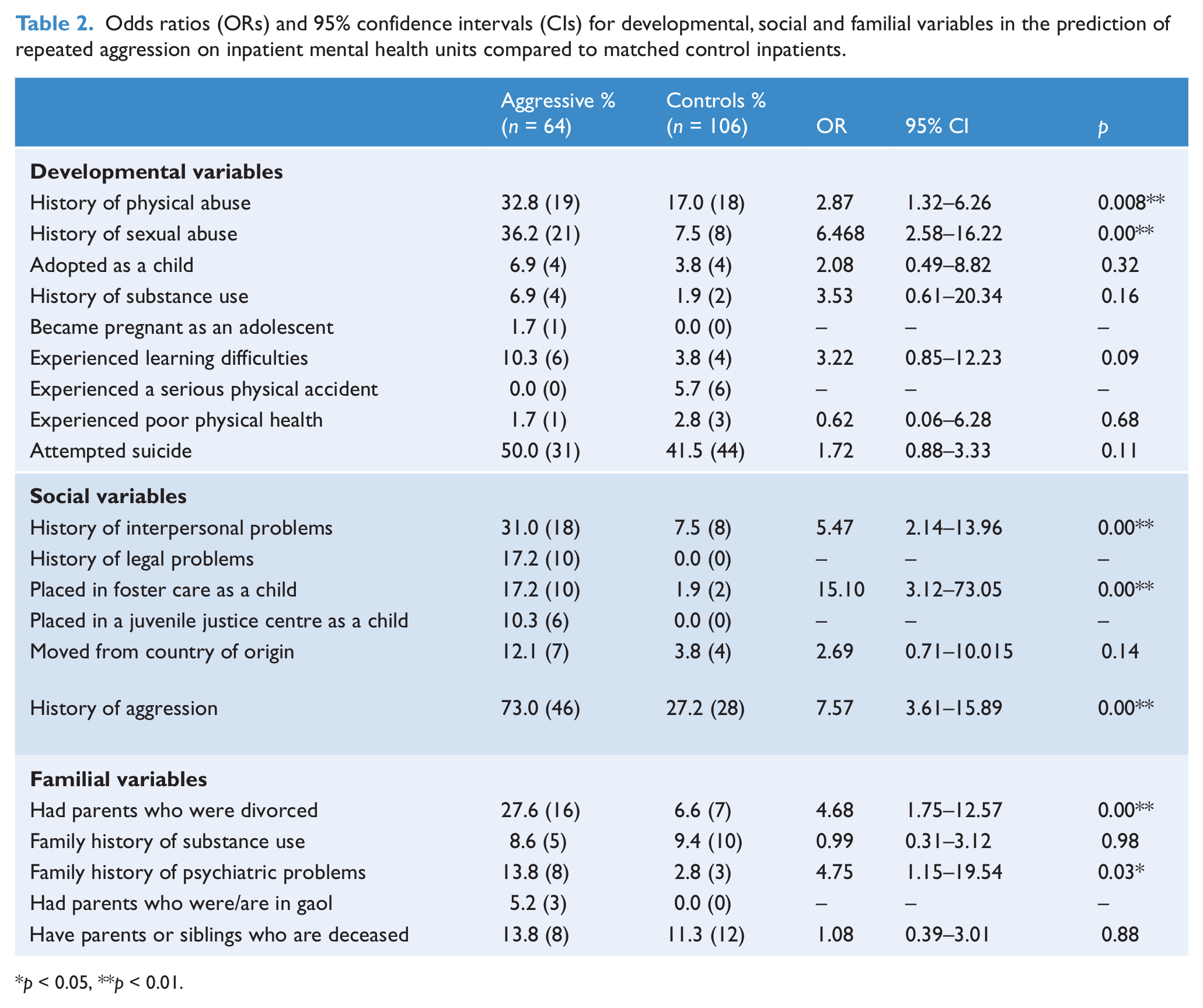
p < 0.05, **p < 0.01.
The only significant developmental variables were physical and sexual abuse, with aggressive patients 2.39 times more likely to have a history of physical abuse (p = 0.02) and 6.94 times more likely to have a history of sexual abuse (p < 0.001). No significant differences were found between the aggressive and control groups for adoption, history of substance abuse, learning difficulties, poor physical health or a history of suicide attempts. Of the social variables, aggressive patients were significantly more likely to have a history of aggression (OR = 7.25, p < 0.001) and interpersonal problems (OR = 5.53, p < 0.001) than control patients. They were also more likely to have been placed in foster care as a child (OR = 10.87, p < 0.001) or had moved from their country of origin (OR = 3.50, p = 0.04). Of the familial variables, aggressive patients were more likely to have had parents who divorced (OR = 5.38, p < 0.001) than controls, and were also more likely to have had parents or siblings with a history of psychiatric problems (OR = 5.49, p = 0.01). No significant differences were found for a family history of substance abuse, or for having parents or siblings who are deceased.
Males were significantly more likely than females to have a history of interpersonal problems (OR = 5.26, CI = 1.46–18.87), a history of aggression (OR = 4.50, CI = 1.35–15.15) and more likely to have had legal problems (OR = 17.54, CI = 71.43–5.99). Females were significantly more likely than males to have a history of sexual abuse (OR = 4.62, CI = 1.44–14.76).
A logistic regression model that included sex and all the variables that were significant at p < 0.05 found that a history of physical abuse and placement in foster care were not independently associated with aggression. Inclusion of length of stay in the multivariate model rendered migration a non-significant risk factor for aggression, suggesting that migrant patients might be more likely to be repeatedly aggressive due to longer length of stay. The inclusion of length of stay in the model did not affect the association between any other psychosocial factor and repeated aggression.
Discussion
This study examined the developmental, social and familial characteristics of repeatedly aggressive mental health inpatients in comparison to a control sample of mental health inpatients matched by age, sex and diagnosis. Only a small number of prior studies examining the characteristics of aggressive patients have used a control group, with some comparing aggressive patients to the general inpatient population and others failing to use any comparison group. Further, most prior studies have generally focused on physical aggression only. This study has attempted to overcome the limitations of previous studies by (i) matching the aggressive patients with two non-aggressive patients by age, sex and diagnosis, therefore increasing the validity of the findings, and (ii) incorporating all aggressive incidents, including self-harm and verbal aggression. The findings of this study might assist in identifying the risk factors of patients who are likely to engage in repeated aggression against themselves or others, and will have implications for the identification of treatment or supervision needs.
The aggressive sample in this study had an average of 3.75 aggressive incidents, and most of the time when incidents occurred they were compulsorily detained under the Mental Health Act (2007) suggesting that they were psychiatrically troubled enough to pose a danger to themselves and others. Thus, most often these patients were placed under close supervision by staff. More often, the aggressive patients were involved in physical aggression, and their aggression was mostly directed at staff. Staff had generally perceived the cause of aggression as being primarily a result of their psychiatric illness. A significant proportion of incidents related to self-harm behaviour, with females being often involved (Saverimuttu and Lowe, 2000). This study also found that females engaged in self-harm most often, which may be associated with comorbid borderline personality disorder for some patients, whereas males generally directed their anger towards others.
Specific characteristics related to an individual’s developmental, social and familial history are associated with an increased risk of aggression. In this study, repeatedly aggressive patients were more than twice as likely to have a history of physical abuse, and more than seven times as likely to have a history of sexual abuse. However, only sexual abuse remained significant after including all significant social, developmental and familial characteristics in a logistic regression model. A significant effect for physical abuse but not sexual abuse has been reported in previous studies (Krakowski et al., 1988). To the best of our knowledge no studies to date have reported or examined the association between sexual abuse and aggressive behaviour by inpatients. Krakowski and colleagues (1988, 1989b) did report an association between aggressive behaviour and a history of suicide attempts and substance abuse. This present study, however, did not support these previous findings.
Repeatedly aggressive patients were six times more likely to have a history of interpersonal problems, and seven times more likely to have a history of aggression, with males being significantly more likely than females to have such histories. Males, again, were 17 times more likely to have had criminal convictions or be awaiting criminal proceedings. These findings are consistent with criminal conviction rates. For example, in the same jurisdiction (NSW), four-fifths of individuals found guilty of crime are males (Statistical Services Unit, 2008). These factors, in addition to having a history of being placed in a juvenile justice centre, suggest that some of the males may have comorbid features of antisocial personality disorder.
Repeatedly aggressive patients were also five times more likely to have had divorced parents. While we found no increased risk between aggressive and control patients if their parents had a history of substance use disorders, or had previously been in goal, others, for example Barber et al. (1988) and Krakowski et al. (1989a), report findings that reflect a positive association.
These patients in inpatient mental health settings present as notable management problems for staff within these facilities. They impact the unit environment, other patients and staff. Generally, the management of repeatedly aggressive patients involves interventions that are primarily designed to produce immediate effects; for example, the administration of intramuscular injections which in this study occurred 41% of the time, and are less driven by theoretical formulations about why the patient is aggressive (Harris and Rice, 1997). Several preventative and management interventions have been recommended for these patients, including improving patient communication skills, increasing feelings of control, power and self-esteem, teaching patients to be assertive rather than aggressive, helping patients to achieve control over drug and alcohol use, stress reduction skills and conflict resolution (NICE, 2005). Long-term treatment interventions targeting aggression have found combined pharmacological and behavioural treatments to be an effective intervention (Harris and Rice, 1997). It has been argued that non-threatening approaches are needed to manage aggressive patients that address anger management (Lewis, 2002), with an emphasis on individualised treatment programs (Fisher, 2003). Programs designed to teach mental health staff working in these facilities to identify the causes and indicators of aggression, and equip staff with skills to more effectively manage aggressive incidents (Grenyer et al., 2004; Ilkiw-Lavalle et al., 2002; Middleby-Clements and Grenyer, 2007), might also impact on the occurrence and severity of aggression in inpatient settings.
The findings of this study should be considered in light of its limitations. First, the information gathered from chart reviews was limited to pre-recorded information. Second, this study matched patients with non-aggressive control patients from the same unit for age, sex and diagnosis, and although an accepted methodology, it is still subject to unknown biases.
Conclusion
This study has found that repeatedly aggressive patients are more likely to have histories of significant deprivation, neglect, abuse and interpersonal problems. Although studying historical factors enables us to understand the predisposing factors for such behaviours, this study highlights the need for long-term management approaches for repeatedly aggressive patients to address their interpersonal and personality disorder deficits. These approaches should address not only the psychiatric illness, but should also incorporate behavioural and interpersonal approaches for patients to learn and develop skills to manage and deal with their anger.
Footnotes
Acknowledgements
The authors would like to gratefully acknowledge the patient participants and inpatient staff.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
Funding was received from NSW Health.