
Abstract
Objective:
Over the last decade, Australia has seen an increase in investment in mental health services, primarily through the funding of headspace and Better Access to Mental Health Outcomes programs. Concurrently there has been a policy focus on prevention and early intervention, suicide reduction and ‘hard-to-target’ groups such as Indigenous groups. It is not clear, however, whether research funding targeting health services or prevention or promotion has been prioritized, or whether funding priorities in general have shifted over the last decade.
Methods:
A total of 1008 Australian-authored research publications and 126 competitive research grants in 2008 were coded in terms of their target of research, research goal setting and target group. These characteristics were compared with the research priorities of 570 stakeholders, burden of disease estimates and similar data collected 10 years earlier.
Results:
The proportion of research funding for affective disorders, dementia and psychosis has increased, but not for anxiety disorders or suicide. Funding for childhood disorders has decreased. Funding for prevention and promotion is low and decreasing. With respect to research publications, substance abuse was associated with the most publications, followed by affective disorders, anxiety disorders and psychosis. When publications and funding are compared to stakeholder priorities and the burden of disease, the areas of suicide and self-harm, personality disorders, anxiety disorders, childhood conditions and dementia are all insufficiently funded.
Conclusion:
Despite mental health policy reforms through the last decade, there has been little change in the focus of research funding or publication output. There is modest evidence for a shift in support towards affective disorders as a major focus for research. However, the remaining gaps were very similar to those identified 10 years earlier showing that suicide, personality disorders and anxiety disorders are under-researched.
Introduction
Jorm et al. (2002) established a methodology for examining research priorities within mental health research. The methodology developed a framework that was applied to a year of research publications and grants. Existing research funding and publications were compared to a range of priority standards – namely, the prevalence of various mental disorders, the burden of disease, the research priorities of stakeholders, and national policy goals. Ten years ago, depression and suicide were under-researched; prevention and promotion, psychological and social interventions and service evaluations were under-represented; and community and primary care settings were relatively neglected as research settings. With respect to subgroups, the report found that Aboriginal and Torres Strait Islander peoples, children and adolescents, and socially and economically disadvantaged people were lacking adequate levels of research interest.
Since the initial Jorm report and subsequent research papers (Griffiths et al., 2002; Jorm et al. 2002), the targets of research funding and the topics of research publications may have shifted, arising, in part, from the influence of new policy and service initiatives in the sector. Established in 2000, ‘beyondblue: the national depression initiative’ had its own stream of direct funding, incorporating the establishment of the Victorian Centre for Research Excellence Grants (beyondblue, 2001, 2010). Australian Rotary Health Grants established grants for community-based mental health research (Australian Rotary Health, 2008, 2012), the Australian Primary Health Care Research Institute was established (Australian Primary Health Care Research Institute, 2010), with a focus on research in primary care settings, and the Howard Government funded e-mental health services, which may have stimulated research. Headspace (Headspace, 2011) and EPPIC (Early Psychosis Prevention and Intervention Centre, 2012) were established as policy initiatives to improve the health of young people. The National Action Plan for Promotion, Prevention and Early Intervention was launched in 2000 (Commonwealth Department of Health and Aged Care, 2000); and the Fourth National Mental Health Plan was launched in 2009 (Commonwealth Department of Health and Ageing, 2009), also with a focus on the promotion of prevention activities.
This paper aims to examine whether there has been a shift in the targets of mental health research over the last decade in association with changes in mental health developments. The specific aims of the paper are to examine for 2008 (a decade after the original review) the content of current research publications and the nature of the grants awarded. These will be compared with two recognised standards by which research priorities might be benchmarked: stakeholders’ views about priorities for mental health research and the burden of disease contributed by each mental health disorder. The original findings of the Jorm review (2002) of data collected 10 years earlier will be compared with the current results.
Method
Grants
Abstracts and funding details for all beyondblue (BB)- and Australian Rotary Health (ARH)-funded grants in 2008 were provided directly from the funding bodies. For NHMRC grants, the public information obtained from the NHMRC website (National Health and Medical Research Council, 2011) was used. These data include scientific title, simplified title, research keywords, health keywords, broad research area and field of research, in addition to metadata for each grant (chief investigator, amount awarded, institution and state). Based on these data, NHMRC grants beginning in 2008 were selected for analysis if they were identified by the NHMRC as mental health related (data are presented by National Priority Areas) or if they contained any mental health-related keywords. Initially, 136 grants were identified. However, a secondary check by two coders identified that 10 of these grants did not contain any mental health-related content based on the available information. After their removal, the final pool of 126 grants ($58,188,442) included 79 NHMRC Project Grants (total funding $52,883,278), 24 BB grants (total funding $4,098,323) and 23 ARH grants (total funding $1,206,841). Based on the available data, each grant was independently coded by two researchers (JG, KK and/or PB). Each grant was rated using a proforma coding sheet to categorise the grant by institution type, state where the research was conducted, type of mental disorder, subpopulation group, research goal and participant or setting type. After coding, discrepancies between the two coders were harmonised by mutual consent. In cases where agreement could not be reached, a third coder made a decision as to which of the codes was most appropriate. These were then compared with grants awarded in 2000.
Publications
To assess the current state of mental health research in Australia, abstracts from all journal articles published by Australian researchers in 2008 were examined for inclusion. The aim was to select a random sample of at least 1000 articles for detailed categorisation. Searches were undertaken across all fields (including title and abstract) using the databases PubMed, Medline, PsycInfo and Informit (formerly The Australasian Medical Index). Both Medline and PubMed were searched, as earlier research indicates that the treatment of wildcards, the inclusion of ‘in press’ articles and the combining of search terms appear to be handled differently. The author affiliation field was limited to ‘Australia’ to select only Australian-authored papers. Duplicate papers were excluded from the complete set of papers. During the first phase, a total of 5297 abstracts including 1270 duplicates were returned by the Medline/PsycInfo combined Ovid search (total = 4027 abstracts), 3114 were returned by the PubMed search, and 137, including one duplicate, were returned by the Informit search (total = 136 abstracts). After removing 2742 duplicates from between databases, 4535 abstracts from the three databases were screened to exclude studies that did not meet the criteria for the review. Specifically, to be included, the study had to report new data or a new analysis of existing data – systematic reviews, meta-analyses, letters, comments and theoretical articles were excluded. In addition, papers which, based on the abstract, clearly had no mental health component were excluded in this first pass. This screening process resulted in 2132 abstracts. Finally, the authors of a further 248 papers had no Australian affiliation, leaving 1884 papers in the final pool.
A total of 1008 of these papers were randomly selected for coding. During the coding process, 165 of the 1008 abstracts were judged not to meet the inclusion criteria and these were excluded from further consideration. Subsequently, an additional set of 165 papers was randomly selected to replace those excluded such that the final sample size of coded studies reached at least 1000. After assessment for eligibility was completed, 1008 papers met the criteria and were coded in full. The schematic of paper selection is illustrated in Figure 1. Each paper was independently coded by two researchers (AG, HC, JG, KG, KK and/or PB). Papers were allocated to coders such that no two researchers coded a disproportionate number of papers together. Each abstract was rated using a proforma coding sheet to categorise studies by institution type, state or territory where the research was conducted, type of mental disorder, subpopulation group, research goal and participant or setting type. Up to five disorders and up to four subpopulations, goals or participants/settings were coded for each paper. Where multiple categories were coded, analysis of the papers was weighted to account for all coded categories in equal proportion. These were compared to the 685 publications identified in the previous analysis of 1998 research output (Jorm et al., 2002).
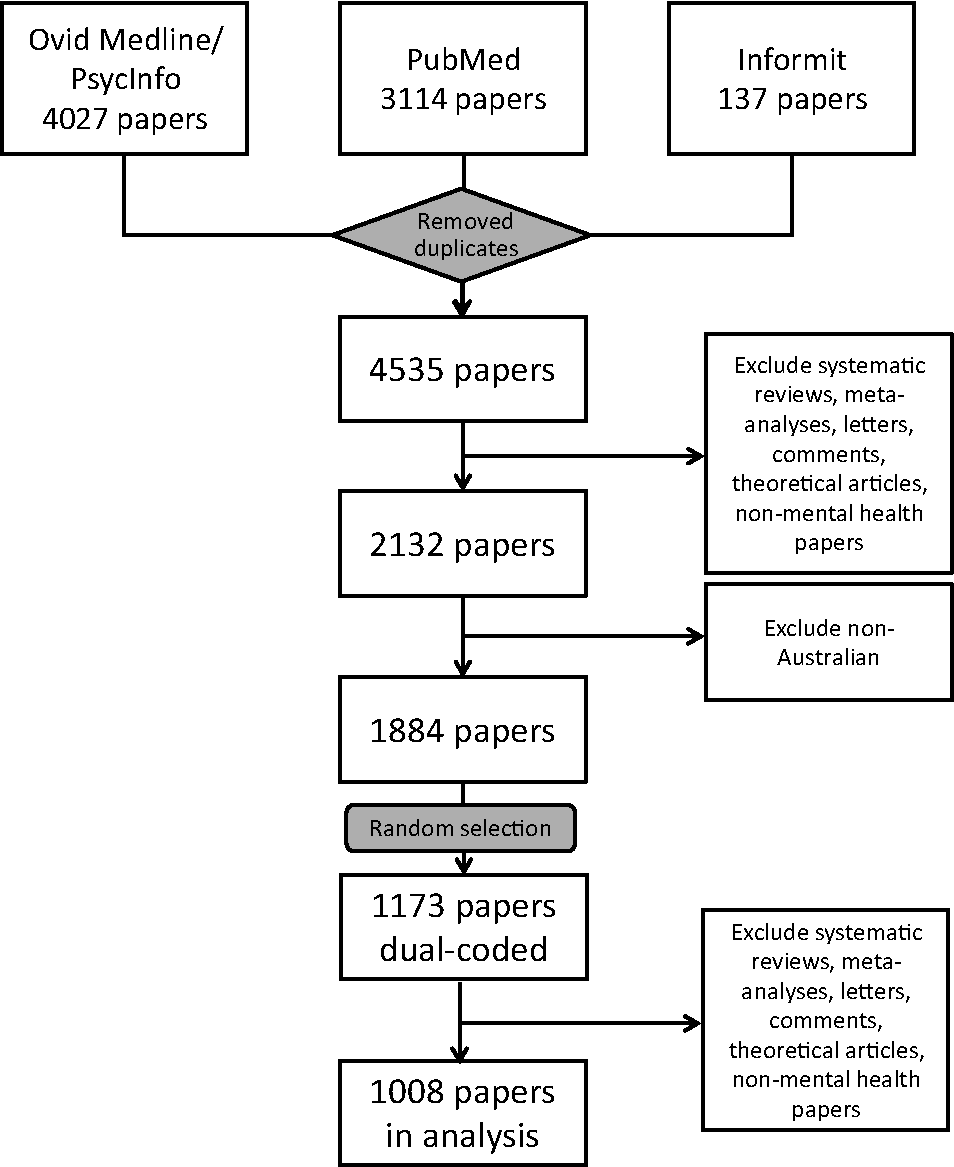
Flow diagram of papers for analysis.
Stakeholder review
An online survey was used to gather stakeholders’ views. Stakeholders were identified by the advisory board that commissioned the review. A total of 139 invitations were sent to a broad range of individual and group stakeholders. Invitees included prominent mental health researchers, research departments, key contacts for federal and state government departments, and mental health consumer groups, carer groups and peak bodies. A total of 672 stakeholders responded to the survey. The survey was fully completed (responses in all sections) by 570 of these respondents. This survey replicated the earlier survey available in full in the 2001 report (Jorm et al., 2002).
Estimates of burden of disease
Research publications and research funding were also compared to relative burden of disease. Burden of disease estimates were taken from The Australian Institute of Health and Welfare (2007) (Begg et al., 2003), which includes disability-adjusted life year (DALY) estimates for: depression and anxiety (combined), bipolar disorder, substance use disorders, dementia, schizophrenia, eating disorders, personality disorders, childhood disorders, suicide, and homicide and violence . To separate affective and anxiety disorder DALY estimates, the proportions of burden used in the previous Jorm report were applied to the more recent combined estimate, with 59.4% attributed to affective disorders and 40.6% to anxiety disorders.
Results
Grants
Although the proportion of NHMRC funding to mental health research has not increased over the past 10 years (Christensen et al., 2011), the total amount of mental health research funding in Australia has increased in net terms over the last 10 years. Based only on NHMRC Project Grants for comparability, total funding increased from $9.5m in 2000 to $23.4m in 2008 and $33.4m in 2011. The funding amounts in the following figures are weighted by the proportion of the grant devoted to mental health research and, where applicable, weighted to account for grants that were coded in multiple categories (i.e. grants investigating multiple disorders had funding distributed equally across those disorders). Figure 2 compares the percentages of grant funding in the years 2000 and 2008 as a function of type of mental disorder. The percentage of grants for research on affective disorders has increased, while the proportion of funding to childhood disorders has decreased dramatically. There has been a proportional increase in research into dementia and the broader category of ‘mental health disorders’. The proportion of substance abuse funding has dropped since 2000.
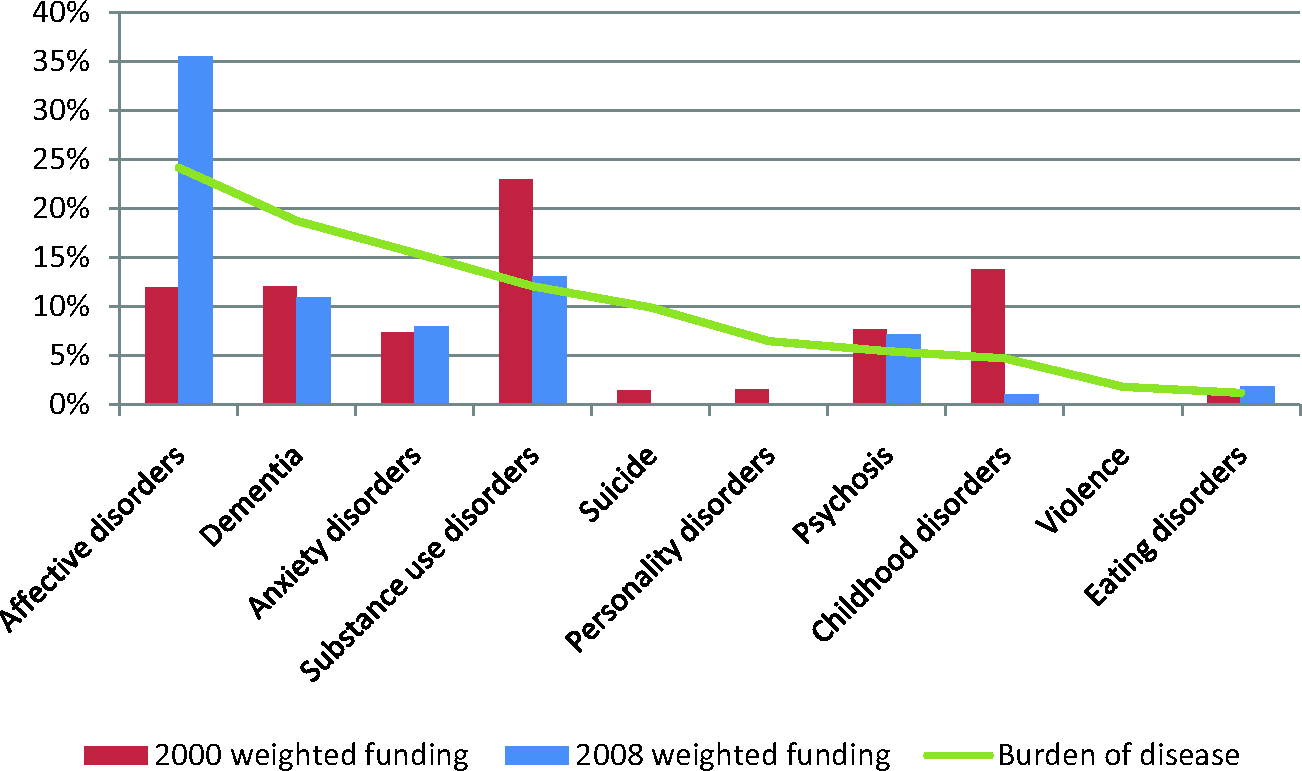
Percentage of grant funding by mental disorder category in 2000 and 2008 analyses. Burden of disease (relative % DALY) for identified disorder categories is also presented (green line).
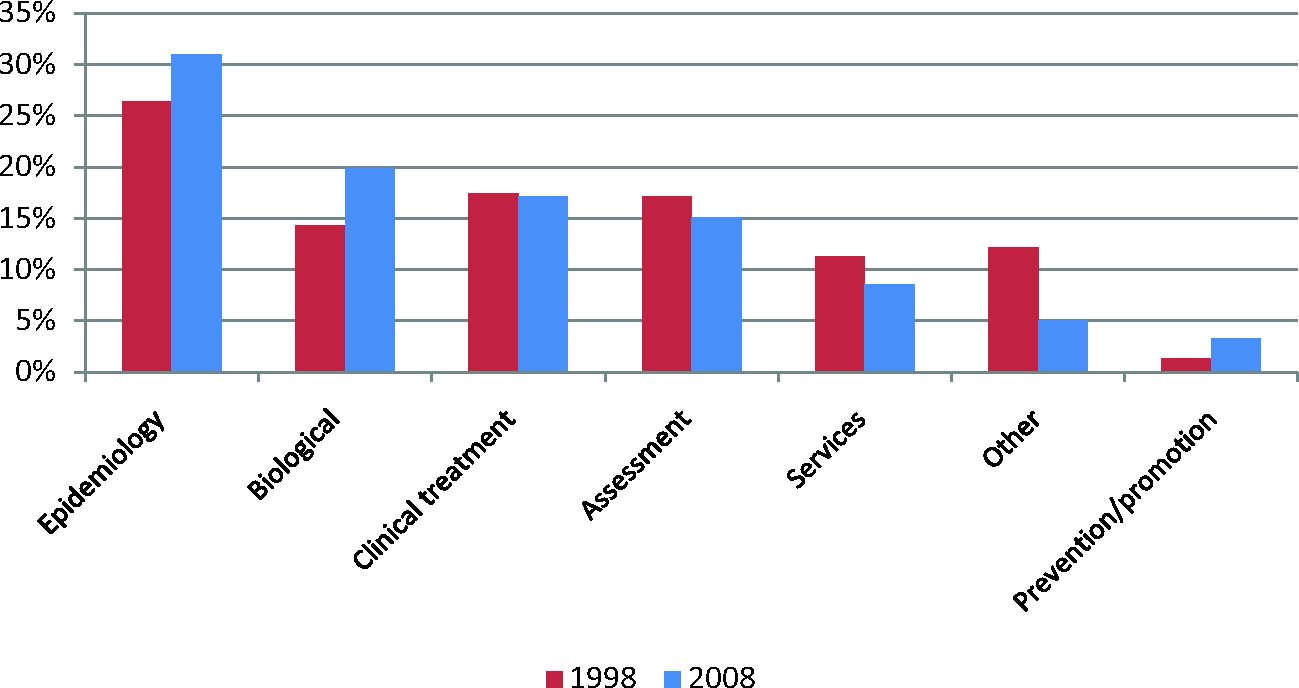
Figure 3 indicates that treatment and epidemiology receive proportionately more funding than they did, but that the proportion awarded to biological grants has reduced. The proportions of prevention and promotion grants and assessment grants are small and decreased between 2000 and 2008. The proportion of services research, while increasing, is also smaller relative to treatment, epidemiology and biological research.
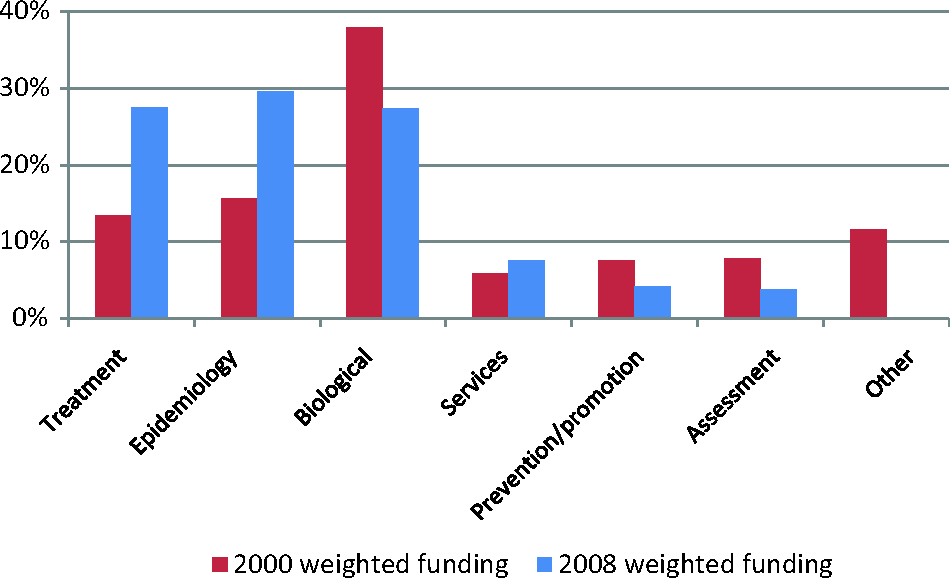
Percentage of grant funding by research goal in 2000 and 2008 analyses.
Publications
There has been a large increase in publication output, from 685 in 1998 to approximately 1800 in 2008. Figures 4 and 5 indicate any changes over the 10-year period for research publications as a function of mental disorder category and research goal. Unlike grant funding, very little has shifted over the period, perhaps suggesting a lag between new areas of grant funding and publications on these topics.
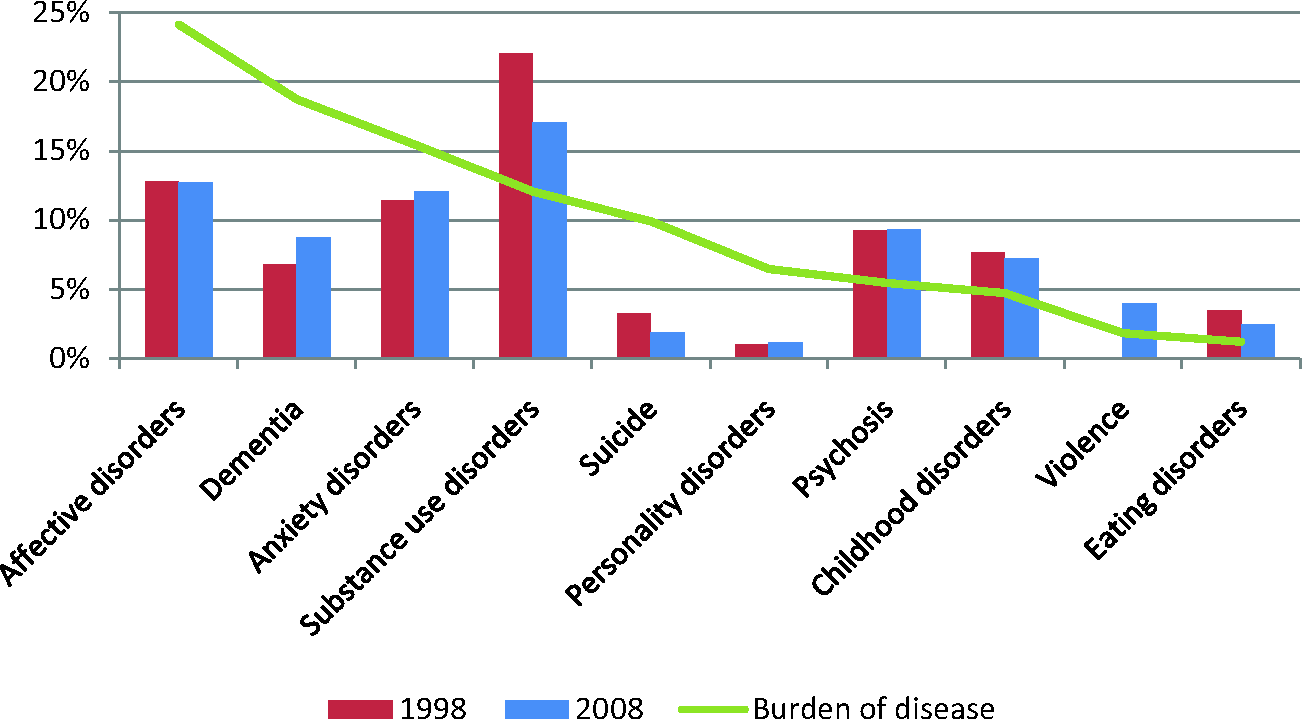
Category of mental disorder in published papers (weighted to account for multiple disorders). Burden of disease (relative % DALY) for identified disorder categories is also presented (green line).
Goal of research identified in published papers (weighted to account for multiple goals).
Comparison to burden of disease
The comparison of burden of disease with funding in 2000 and 2008 is shown in Figure 2 (green line) while the comparison of burden of disease with publications in 1998 and 2008 is shown in Figure 4 (green line). In calculating the disease burden percentages, only the disorders included in the figures were used, so that the numbers add up to 100%.
From Figures 2 and 4, it appears that affective disorders are now receiving a proportion of mental health funding that is consistent with disease burden relative to other mental disorders, but this has not yet translated to research output. Dementia and anxiety disorders appear to be underfunded and both are lagging in publication output. The gap is more pronounced for suicide and personality disorders, which receive proportionately little funding and account for very little of the publication output, despite contributing 7–10% of the burden of disease associated with mental disorders. Substance use disorders are relatively better-funded and contribute a greater percentage of publications than would be expected based on burden of disease. Psychosis and eating disorders appear to be funded approximately in line with disease burden, although their rates of publication are higher. Childhood disorders have gone from being well-funded proportionately relative to other mental disorders in 2000 to relatively underfunded in 2008, although publication rates remain satisfactory.
Comparison to stakeholders’ priorities for research
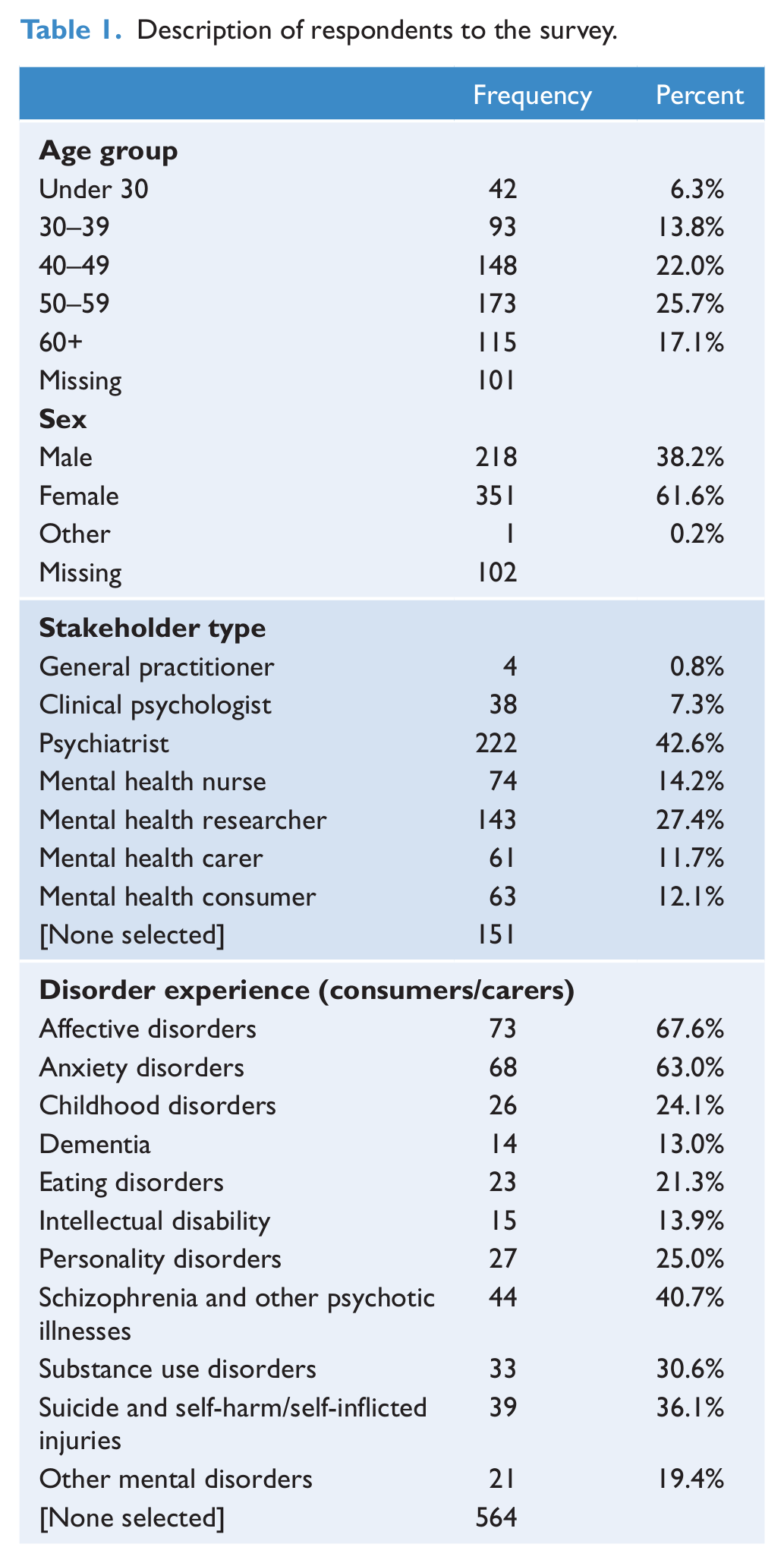
The survey was fully completed (responses in all sections) by 570 of the 672 respondents. A summary of characteristics of respondents who completed the stakeholder survey in full is shown in Table 1.
Description of respondents to the survey.
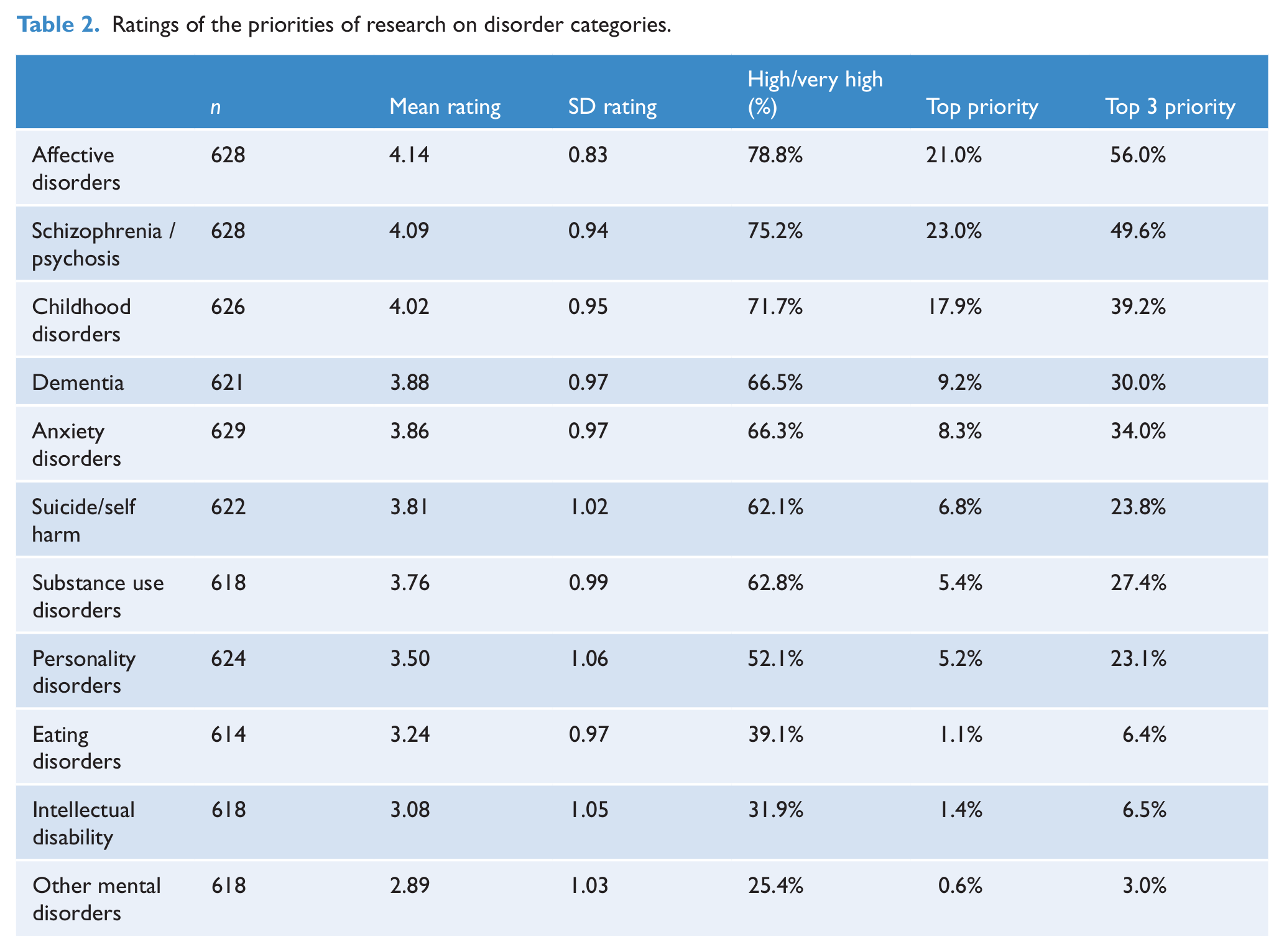
Relatively little disagreement about priorities for mental health disorder were discernable across health professionals and consumer carers .Consequently, Table 2 categorises the ratings across all stakeholder groups according to the mental disorder categories. The areas considered to have the highest priorities were affective disorders, psychosis and childhood disorders (Table 2).
Ratings of the priorities of research on disorder categories.
Rankings were also compiled for research goals. The top priority goals were prevention of mental disorders (44% of respondents rated this in their top three), followed by psychological and social treatments (30%) and evaluation of services (28%). Lowest priorities were historical research, animal models and the assessment and classification of disorders. The highest rated priorities for research in target groups were children/young adults (63%), Indigenous peoples (37%) and economically and socially disadvantaged people (37%). Direct comparisons of these ratings with 1998 ratings were not undertaken given the difference in the constitution of the stakeholders between the two surveys.
Discussion
Summary
There has been little change from the previous report in the types of disorders that are most commonly researched in Australia. While there has been a decrease in the proportion of substance use-related publications, this is still a dominant area of research. This dominance does not clearly conform to stakeholder views of priorities for mental health research or to relative disease burden, and must presumably be due to other factors. While there has been an increase in the proportion of grant funding to affective disorders, there has been no increase in the proportion of publications. There has been little change in the proportions of funding or publishing in psychosis over the past decade, indicating that psychosis research is maintaining its status rather than growing. Dementia research accounts for a larger proportion of funding than in 2000, and has also seen an increase in the proportion of publications.
Anxiety disorders and childhood disorders are now receiving a smaller proportion of funding, although the proportion of publications has remained fairly stable. As in 1998, there is negligible funding for research on suicide and self-harm, and, as a possible consequence, the proportion of publications in this area has continued to fall sharply. Likewise, there is very little research conducted on personality disorders in Australia. Based on the comparison to stakeholder priorities, there should be considerably more research effort devoted to childhood conditions and suicide and self-harm. The need for more research funding and output on suicide and self-harm, personality disorders, anxiety disorders and dementia is reflected in comparisons to both relative burden of disease and stakeholder priorities.
Stakeholder priorities for research tended to conflict with the current picture of research activity. This divergence was most pronounced in examining the goals or topics of research. There is very little funding or publication related to prevention of mental disorders and promotion of mental health. However, this was the top priority for stakeholders. Prevention and promotion also received a significantly smaller proportion of funding in 2008 compared to 2000.
Limitations
This report presents a rigorous, double-coded stocktake of mental health research in Australia, with a comprehensive assessment of stakeholder priorities in mental health research. It replicates the previous analysis of research priorities (Jorm et al., 2002) and enables assessment of trends in research over the decade. However, there are some limitations to the analyses that should be acknowledged.
We have only analysed 1 year of publications and grants and due to resource and time constraints, we only included the primary mental health project funding schemes and a randomly selected subsample of the publications for 2008. We analysed and coded 126 grants with total funding of $58.2m, compared with 323 grants at $20.4m from 1998. We did not include other types of funding, including smaller grant schemes, funding for researchers and non-competitive funding.
The analysis of 1008 papers goes well beyond the previous analysis of 685 papers (Jorm et al., 2002). Whilst the information that was available about the grants was not as comprehensive as for the previous analysis, the current report nevertheless coded the major sources of research funding, including funding through the NHMRC and beyondblue. Further, the limited information available and inclusion of different grant schemes led to some difficulties in comparing 2008 funding results with 1998 funding results. The stakeholder disorder rankings also limited the extent to which the importance of co-morbid disorders could be rated. Invitations for the stakeholder survey were sent to a broad range of stakeholders. However, we had little control over whether the invitations were distributed more widely, particularly when we requested that invitations be sent on to members of organisations. As a consequence, some stakeholder groups were better represented than others. Nevertheless, the overall sample of 672 stakeholders was similar in size to the sample of 686 stakeholders who completed the previous survey (Jorm et al., 2002).
It is also likely that different respondent groups were more familiar with or interested in particular types of disorders. For example, dementia is not commonly dealt with by psychiatrists, clinical psychologists or mental health nurses, potentially impacting on their views on research priorities for this area. Likewise, stakeholders may also have had varying degrees of knowledge about the current state of mental health research in Australia. Although the survey was explicit about its focus on research, some stakeholders may have had difficulty distinguishing between priorities for research and priorities for services.
Key findings
Overall, we identified the following disorders as being underfunded in Australia: suicide, personality disorders and anxiety disorders. Research topics that were underfunded were prevention and promotion, psychological and social interventions, service evaluation and staff training. Population subgroups that need more research funding are children and adolescents, Aboriginal and Torres Strait Islander peoples and socially and economically disadvantaged people.
Conclusions
There is much discussion about priorities being set for medical research funding. Mental health policy in the last decade has focused on prevention and promotion, primary health care, and adolescent services. However, overall, these developments have not strongly shifted the focus of research funding or publication, although there is some evidence that there is now a shift in support for affective disorders as a major focus for research. There has been no parallel shift in research for young people or those with childhood conditions. In fact, there has been a relative drop in funding for research on childhood and adolescent groups in the last decade. Stakeholder views remain very similar to the previous survey, in wishing for, but not receiving priority research for Indigenous peoples and people experiencing social and economic disadvantage. Despite the Government’s focus on prevention and promotion as goals in public policy, prevention and promotion research remains underfunded, and efficacy studies are few. Research into suicide, which is now a number one priority of the new National Mental Health Commission, has decreased relative to other fields of mental health research in the last decade.
In short, as noted by one of the anonymous reviewers of this paper, the cake of funding has grown, but the way it is divided up is unchanged. How this slicing of the cake might be determined or might change is not so clear. The recent release of both the Wills review of health research in NSW (Wills et al., 2012) and the recommendation paper of the McKeon report (McKeon et al., 2012) suggests that a move from purely investigator-driven research to research that works through health systems, NGOs, industry and integrative health centres, such as the Health–Science Alliance, will be promoted in the next few years.
Footnotes
Acknowledgements
Thanks are due to Ms Katherine Petrie for formatting the manuscript and Amelia Gulliver who assisted with the coding of the research papers.
Funding
This research was funded by the Mental Health Advisory Board of the Commonwealth Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.