
Abstract

Introduction
Employment is a central part of recovery for many patients, is generally good for mental health, and the evidence on how best to support people with a mental illness into jobs is well established. In Australia and New Zealand the employment rates of people with a mental illness remain extremely low, at less than 25% (Waghorn et al., 2012; Walsh, 2010) and employment support is not widely available as part of clinical practice. If evidence-based employment programmes were part of routine treatment at least 45% of people could be supported into employment and enabled to build careers (Drake et al., 2012).
This viewpoint provides a summary of the international research on the effectiveness of Individual Placement and Support (IPS) an approach to supported employment for people with a mental illness also referred to as evidence-based supported employment (EBSE). It describes the intervention and explores methods for its successful implementation. It argues that to address this evidence to practice gap a systematic implementation programme is needed across New Zealand and that psychiatrists and their professional bodies are well placed to influence and accelerate this implementation in publically funded mental health services. They can lead the development and delivery of employment-focused health services and influence public policy, funding and community expectations.
The science of supported employment
Data on the employment rates of people who are in contact with community mental health services is not routinely collected in New Zealand. However, Walsh (2010) was able to gather some data from audits conducted in eight District Health Boards which included information on employment status. From this, an average employment rate of 10% was estimated in 2004 increasing to just 17% in 2005. This figure compares with an employment rate of 45% for people across all disability groups and an employment rate of 77% at that time for the population without a disability (Statistics New Zealand, 2008). Aspirations however remain high as people see employment as a key part of their recovery (New Zealand Mental Health Commission, 2001).
Growing aspirations but continued low employment rates across developed countries has meant that methods of supported employment have been increasingly the focus of research, with more than 16 randomised controlled trials (RCTs) conducted internationally validating IPS supported employment. IPS takes a ‘place then train’ approach which helps people gain employment and then supports them in the job, against traditional vocational rehabilitation which focuses on pre-job training prior to employment placement, that is ‘train then place’.
IPS employment services outperform traditional vocational services by nearly three times achieving 62% employment outcomes compared to 23% (Bond et al., 2008). Employment outcomes are defined as competitive jobs which are available to anyone in the labour market to apply for, have permanent status rather than temporary or time-limited, pay at least minimum wage and are not set aside for people with disabilities (with the exception of peer specialist roles). Around two-thirds of people who gain employment through IPS services work more than 20 hours per week and secure their first jobs ten weeks earlier than the controls (Bond et al., 2008). Longitudinal studies give evidence on job tenure. Two such studies, following people for 10 years, showed that more than half who secured employment through IPS programmes were employed for at least 50% of the ten years (Becker et al., 2007; Salyers et al., 2004).
In 2007, the results of the first European IPS RCT were published aiming to understand the application of the evidence outside North America. The trial was conducted in six countries and had tight inclusion criteria to ensure the profile of participants was consistent: people with experience of psychosis, extensive unemployment (greater than one year) and who had experienced major role dysfunction for more than two years. IPS programmes outperformed the best available vocational services in each country, regardless of benefits systems or labour market conditions (Burns et al., 2007). The only factor which had a significant impact on the effect size was the local unemployment rate: as this went up the effect size reduced. The European study also examined the relationship between getting a job and going into hospital and, in contrast to concerns often held amongst clinical staff that employment can exacerbate a person’s symptoms, concluded that ‘going into employment does not make a person unwell’ (Burns et al., 2007).
The features of IPS and the fidelity scale
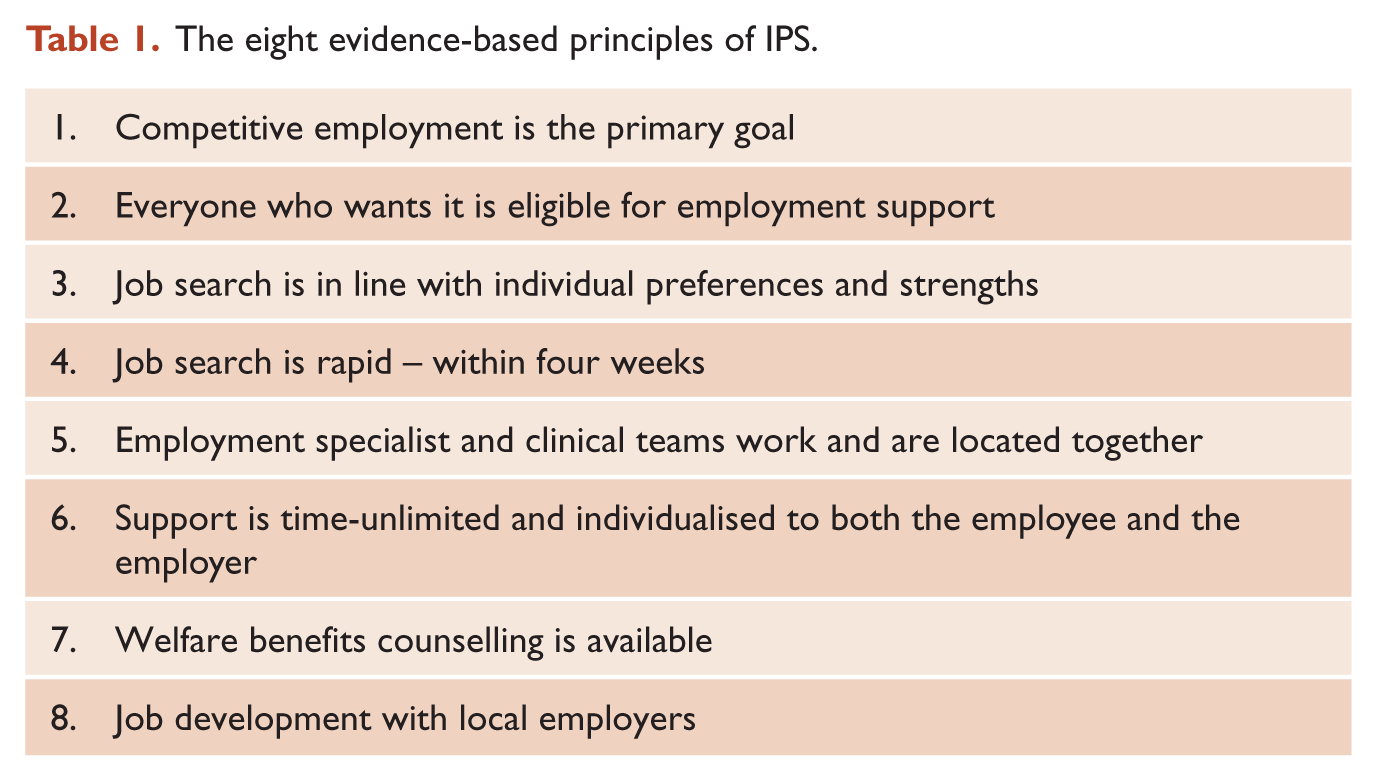
IPS is based on eight principles (Table 1) which all have their own underpinning evidence (Bond, 2004). The closer a supported employment programme aligns itself to these principles the better the outcomes achieved (Bond et al., 2008) (Table 1).
The eight evidence-based principles of IPS.
As with other evidence-based practices (EBPs), a standardised fidelity scale has been developed from the research. The supported employment scale consists of 25 items related to the key components of the practice. The use of a scale in this way for a psychosocial intervention contrasts with other interventions, such as cognitive behavioural therapy, where no fidelity scale is yet developed.
The importance of fidelity scales is illustrated in a recent RCT conducted in England which found no difference in outcomes between the control and the supported employment intervention group (Howard et al., 2010). Measurement against the scale based on descriptions provided by the authors indicated that the failure to demonstrate difference between groups was most likely due to poor programme implementation including, for example, the low intensity of the service and the lack of governance arrangement between the mental health and employment service agencies.
Adherence to the fidelity scale helps ensure the employment programme is patient centred and individually tailored. It involves integrating employment support into mental health treatment through the location of an employment specialist within a multi-disciplinary team. The employment specialist is either employed by the publically funded health service or by an external employment service provider, such as a Non-Government Organisation (NGO). Through this approach employment becomes an integral part of the care plan and is offered to everyone who is receiving treatment from the clinical team and who has an interest in gaining a job. The importance of referring all motivated patients to employment specialists without applying explicit or implicit exclusion criteria is crucial as individual characteristics such as age, gender, race, education, marital and housing status, diagnosis and symptoms including substance dependence do not predict who will or will not get and keep a job (Campbell et al., 2009).
Cost-effectiveness and resource allocation
Larger trials following people over more than two years are needed to better understand the cost-effectiveness of IPS programmes, however, there is some emerging evidence. In the United States Drake et al. (2010) suggested that given the returns from reduced welfare benefits payments, increased taxes and decreased use of mental health services, investment in IPS programmes could be at little or no cost to government. The European RCT also found that use of community mental health services and hospital admission rates reduce when people gain employment (Burns et al., 2007).
In the current fiscal environment resource allocation away from treatments or interventions which are less effective relative to their costs is key to increasing access to EBPs. A Canadian study estimated that supported employment could be funded across the province of Quebec for everyone who is likely to need it for half the cost of what was currently being invested in less effective or ineffective services (Latimer et al., 2011).
Addressing the science to practice gap
The very low employment rates of people with a mental illness provide the moral imperative for action, to make employment support services in line with the principles of IPS a routine part of mental health services in New Zealand. For many years the country has funded supported employment services which are separate from mental health services. This is largely as a result of the fact that funding for employment services can be sourced from two government departments, the Ministry of Social Development (MSD) and the Ministry of Health, and there is no agreement on whose core business it is. There is a lack of policy guidance and common funding methods meaning that the decisions on whether and how to fund and deliver services in line with the evidence base rest with local planners and funders. Service providers therefore remain vulnerable to personnel changes and local funding choices.
Despite this, IPS programmes do exist in parts of New Zealand which show the real-world application of the efficacy trials (Waghorn et al., 2011; Porteous and Waghorn, 2009). Effective implementation has involved on-site leadership to help overcome organisational and cultural barriers to enable both the employment and the mental health service to function as one integrated service to the benefit of individual patients. In one site this also involved converting an existing clinical role, an occupational therapist position, into an employment specialist post.
A key aspect of IPS programmes is that mental health services view assistance towards recovery and social inclusion as part of their core business and acknowledge that case management alone will not achieve this. Once accepted, employment support is offered routinely as part of an integrated treatment package. For many clinicians, this can challenge their professional training and clinical experience. It takes time, commitment to full integration and most importantly demonstrations of success to bring about the change in attitudes and culture needed to maximise the impact of the employment specialist within the clinical team (Shepherd et al., 2012).
A systematic implementation programme is needed in New Zealand to move beyond the early stages of implementation to sustained implementation. Key components of this programme need to be identified based on the available evidence from other countries and then tested to understand local effectiveness. The development nationally of early intervention services in New Zealand more than a decade ago illustrates the feasibility of relatively quickly translating new evidence and models of care into day to day service delivery if a national perspective is taken.
The United States has the ‘Johnson and Johnson - Dartmouth Community Mental Health Programme’, a systematic programme of IPS implementation with technical support provided across 13 states. A smaller implementation programme is available in the UK through the Centre for Mental Health. Both the US and UK programmes are committed to bridging the science to practice gap. They regularly conduct fidelity reviews to check practice against the evidence base and feed this back to practitioners for service improvement. This is an approach which is consistent with the evidence from implementation science (Fixsen et al., 2005) and needs to be more thoroughly applied in New Zealand.
Employment-focused mental health services
The New Zealand Minister of Health has signalled a desire for clinical leadership in health service planning and delivery, as well as the need for savings through service efficiencies (Ministry of Health, 2012). The evidence is clear that health services must be delivered in parallel with, not sequentially with, vocational services and people do not have to be symptom free before returning to work (Shepherd et al., 2012).
Employment-focused healthcare is a term that is used in the vocational rehabilitation literature across all health conditions. Psychiatry and psychiatrists have an opportunity to advocate, educate and lead in this area. What would this look like in psychiatry? It is important for psychiatrists to familiarise themselves with the evidence that now exists about the efficacy of employment interventions and to incorporate this in their approach to patient care. Knowledge of a patient’s circumstances and their aspiration for meaningful employment should be as central to care as knowledge about their family/wha-nau, social supports and living situation. These issues are a core part of a patient’s wellbeing and recovery just as they are to all members of the community. At an individual physician level conversations about working life and aspirations to work should be part of routine consultations. Clinicians are critical carriers of hope in relation to return to work and need to ensure they don’t perpetuate a negative cycle of hopelessness (Marwaha et al., 2008). Despite the evidence and the aspirations of patients clinicians may have misperceptions that employment and employment programmes are a barrier to recovery. A series of self reflective questions could address these perceptions – ‘Am I aware of how competitive employment contributes to recovery?’ and ‘do I believe that competitive employment is feasible for clients with severe and persistent mental illnesses?’ Along with questions directed to patients about whether they are working, would like to work and what help the clinician can offer them with this.
Professional bodies such as the Royal Australian and New Zealand College of Psychiatrists are well placed to play an important role in influencing public policy and community expectations about the need for effective employment interventions as part of mental health treatment. The College can advocate that government policy and national planning should include reference to this aspect of integrated mental health service delivery and guide funders and planners on its importance and the fact that national, regional and local measures of health systems performance should use indicators of role functioning and social inclusion, including employment. Supporting people to remain in or return to work is an important clinical outcome of the treatment of patients of working age and should be a health key performance indicator. Furthermore, college training and continuing education of psychiatrists should include familiarisation with the evidence on employment and mental health.
Conclusion
People who experience a mental illness want to work and there is now good evidence on the best approach to supporting patients to secure and sustain jobs. IPS is a proven psychosocial intervention which translates across countries and into real-world mental health services. It is effective and looks to be cost effective or at least cost-neutral. Other countries are testing methods to improve and embed implementation but as yet there is no proven method for implementing IPS on a larger scale in Australia and New Zealand. The low employment rates of people with a mental illness combined with the evidence provide a strong moral obligation and an opportunity for psychiatry, for the College and for psychiatrists to take a lead in adapting practice to the evidence, in the education of psychiatrists and by influencing national and regional policy, funding and planning so as to identify and test methods of implementation which will bring this evidence into routine clinical practice.
Footnotes
Acknowledgements
The authors would like to thank the peer reviewers for their constructive and valuable comments.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.