
Abstract
Background:
Depression is an important health issue amongst older adults. Internet-delivered cognitive behaviour therapy (iCBT) may help to reduce barriers and improve access to treatment, but few studies have examined its use with older adults. The present study evaluated the efficacy, acceptability and feasibility of a brief iCBT program, the Managing Your Mood Program, to treat depression amongst adults aged 60 years and older.
Method:
Using an open trial design, 20 participants with elevated symptoms of depression (Patient Health Questionnaire 9-item (PHQ-9) total scores ≥ 10) received access to five educational lessons and homework summaries, additional resources, a moderated discussion forum and weekly telephone or email contact from a clinical psychologist. Eighty percent of the sample met diagnostic criteria for a major depressive episode at pre-treatment.
Results:
Completion rates and response rates were high, with 16/20 participants completing the five lessons within the 8 weeks, and post-treatment and 3-month follow-up data being collected from 17/20 participants. Participants improved significantly on the PHQ-9 and Geriatric Depression Scale (GDS), with large within-group effect sizes (Cohen’s d) at follow-up of 1.41 and 2.04, respectively. The clinician spent a mean time of 73.75 minutes (SD = 36.10 minutes) contacting participants within the trial and the program was rated as highly acceptable by participants.
Conclusions:
The results are encouraging and support the potential value of iCBT in the treatment of depressive symptoms amongst older adults.
Keywords
Introduction
Depression in older adults is an important public health issue and is associated with exacerbation of existing physical illness (Braam et al., 2005), increased risk of death (Adamson et al., 2005) and cognitive impairment (McClintock et al., 2010). Prevalence estimates vary between studies (Trollor et al., 2007), with some reporting the prevalence of depressive symptoms amongst older adults (60 years plus) at between 8% and 16% with 1% to 3% meeting diagnostic criteria for major depressive episode (Pirkis et al., 2009). This is concerning given the proportion of older adults is widely known to be increasing (Australian Bureau of Statistics, 2009).
There is now considerable evidence that cognitive-behavioural therapy (CBT) is an effective treatment for depression (Butler et al., 2006). CBT for older adults is similar to that used for younger adults, but appears to benefit from augmentation with applied gerontological knowledge, taking account of cohort beliefs, physical health status and stage-of-life transitions (Laidlaw et al., 2004). Evidence supporting the use of CBT for older adults is promising (Scogin et al., 2005), although methodological concerns have been raised and indicate the need for more clinical trials (Wilkinson, 2009).
One issue confronting the dissemination of psychological treatments for depression amongst older adults is that treatment-seeking is low (Trollor et al., 2007). Common barriers to face-to-face treatments include stigma, limited understanding of mental illness, direct and indirect costs, mobility limitations and shortages of available services. In recent years, internet-delivered cognitive behavioural therapy (iCBT) has emerged as an approach that may reduce some of these common barriers to treatment. iCBT uses the same principles as standard face-to-face CBT, but is delivered via the internet with support via email or telephone (Titov, 2011a). There is now considerable meta-analytic support for the efficacy of iCBT for depression, with moderate to large effect sizes generally being obtained when trials are supported by a clinician (Andersson and Cuijpers, 2009). To date, only one randomised controlled trial has examined the efficacy of iCBT with adults over the age of 50 years and it focused on adults experiencing subclinical levels of depression (Spek et al., 2007). It yielded promising results with effect sizes of 1.0 for a self-guided internet treatment compared with 0.45 for an untreated waitlist control group (Spek et al., 2007). More research examining the outcomes of iCBT for older adults meeting diagnostic criteria and with clinical levels of depression is required. However, the existing findings indicate the potential of iCBT in improving access to mental health services for older adults given that household internet use amongst older adults is expected to grow rapidly (Ewing and Thomas, 2010).
The present study examined the efficacy, acceptability and feasibility of a brief iCBT program, the Managing Your Mood Program, for symptoms of depression amongst adults aged 60 years and over. The Managing Your Mood Program is a five-lesson CBT program, which is delivered over 8 weeks with weekly contact from a clinical psychologist via email and telephone. Using a single-group open trial design, it was hypothesised that: (1) participants would show statistically significant improvements on measures of depression, anxiety and disability; (2) these changes would be reflected in clinically significant improvements on measures of depression and anxiety; and (3) participants would rate the program as acceptable.
Method
Participants
Applicants applied online through a clinical research website set up for iCBT trials after reading details about the study and the inclusion and exclusion criteria. No direct advertising was employed for the trial as sufficient participants were recruited via the website, which provided information about common mental health difficulties and the opportunity to participate in a variety of online treatment programs.
In order to be eligible, participants had to: (1) be a resident of Australia; (2) be at least 60 years of age; (3) have computer and internet access; (4) not be participating in CBT elsewhere; (5) not be using illicit substances or drinking more than three standard drinks a day; (6) not have experienced a psychotic mental illness; and (7) have a Patient Health Questionnaire 9-item (PHQ-9) score > 9, but not currently experiencing severe depression (defined as a total score > 19 or a score > 2 on question 9 of the PHQ-9) (Kroenke et al., 2001). Participants were excluded if they were taking regular benzodiazepine medication (i.e. more than once every 2 weeks) and, if taking a medication for anxiety or depression, were not on a stable dose of medication for at least 1 month. Participants who met these criteria were administered the Mini International Neuropsychiatric Interview Version 5.0.0 (MINI) (Sheehan et al., 1998) via telephone to establish whether they met DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) criteria for an anxiety disorder or depression.
Thirty older adults applied to participate in the trial and 20 were found to be eligible. Of the 10 participants excluded, seven had insufficient symptoms (PHQ-9 total score < 10), one participant had a diagnosed psychotic illness, one was under 60 years of age and another was not on a stable dose of anti-depressant medication. The resulting sample had a mean age of 63.4 years (SD = 5.08; range = 60–80) and 13/20 participants (65%) were female. Ten of 20 participants (50%) reported being either married or in a de facto relationship and 9/20 (45%) reported being separated or widowed. Nine of 20 participants (45%) were in full-time or part-time employment and 11/20 (55%) reported being retired, unemployed, or unable to work due to a disability. Nine of 20 participants (45%) had a tertiary education and 6/20 (30%) reported having a post-high school certificate. Sixteen participants (80%) reported having had previous mental health treatment and nine (45%) reported taking medication related to their symptoms. Seventeen (85%) met DSM-IV criteria for a current major depressive episode. In addition to depression, three (15%) met criteria for panic disorder, eight (40%) met criteria for social phobia, 12 (60%) met criteria for generalised anxiety disorder and two (10%) met criteria for post-traumatic stress disorder.
Study design
A single-group open trial design was employed comparing pre-treatment to post-treatment and post-treatment to 3-month follow-up. Participants were administered all of the questionnaire outcome measures at pre-treatment, post-treatment and at the 3-month follow-up. The PHQ-9 and Generalised Anxiety Disorder 7-item scale (GAD-7) were also administered at mid-treatment. At application all participants were administered telephone-based diagnostic interviews using the MINI to determine whether they met DSM-IV criteria for an anxiety or depressive disorder. These assessments were conducted by JZ, BFD and a senior research assistant.
One clinical psychologist (JZ) provided all clinical contact with participants and a research assistant provided administrative support. Clinical contact was recorded and occurred via telephone and email. The therapist was advised to limit weekly contact time to approximately 10 minutes per participant unless more time was clinically indicated. The therapist aimed to provide the following four components in each interaction with participants: reinforcement of progress; a summary of the key skills described in the program; normalising of difficulties commonly experienced during treatment; and encouragement to continue. The clinician was supervised by BFD and NT with scheduled meetings every second day and on an as-needed basis outside of those meetings.
The study was approved by the Human Research Ethics Committee (HREC) of St Vincent’s Hospital (Sydney, Australia) and the HREC of the University of New South Wales (Sydney, Australia). The trial was registered on the Australian and New Zealand Trials Registry (registration #ACTRN12611000009910).
Questionnaire measures
A wide range of measures were administered to help determine the impact of the program on several areas of functioning including anxiety, disability and self-reported cognitive status. Apart from the MINI diagnostic assessment, all questionnaires were administered via the internet at pre-treatment, post-treatment and the 3-month follow-up. Treatment satisfaction was assessed at post-treatment via two questions enquiring (1) whether participants would recommend the program to a friend and (2) whether the program was worth their time. Participants either responded in the positive or the negative to these questions.
Primary measures
Patient Health Questionnaire – 9-item (PHQ-9) (Kroenke et al., 2001)
The PHQ-9 is a 9-item measure of the symptoms and severity of depression. It is based on DSM-IV criteria with a total score of 10 predicting a DSM-IV diagnosis of depression and with increasing scores indicating greater symptom severity. Psychometric studies indicate the internal consistency is high (α = 0.74–0.89) (Kroenke et al., 2001) and the measure is sensitive to change (Titov et al., 2011b). Cronbach’s alpha in the present study was high (α = 0.78).
Geriatric Depression Scale – 15-item (GDS) (Sheikh and Yesavage, 1986)
The 15-item short-form version of the GDS is a widely used screening measure for depression amongst older adults. The GDS employs a dichotomous ‘Yes’ or ‘No’ response format and places less emphasis on the somatic symptoms of depression, which are often confounded in older adults due to the increased presence of physical health conditions. The short-form version of the GDS was used in the current study to reduce burden on participants. The GDS short-forms have also exhibited good internal consistency (α = 0.72–0.88) in previous studies (Jongenelis et al., 2005) and was high (α = 0.77) in the present study.
Secondary measures
Generalised Anxiety Disorder – 7-item scale (GAD-7) (Spitzer et al., 2006)
The GAD-7 is a 7-item scale and was designed as a brief screening questionnaire for generalised anxiety disorder. Evidence suggests that the GAD-7 is sensitive to DSM-IV congruent generalised anxiety disorder, social phobia and panic disorder, with increasing scores indicating greater severity of symptoms (Löwe et al., 2008). The GAD-7 has good internal consistency (α = 0.79–0.91) and good convergent and divergent validity with other anxiety and disability scales (Dear et al., 2011b; Kroenke et al., 2010). The GAD-7 is increasingly used in research and in large-scale dissemination studies as a generic measure of change in anxiety symptoms (Clark et al., 2009). In the present sample, Cronbach’s α = 0.81.
Kessler 10-item scale (K-10) (Kessler et al., 2002)
The K-10 is a 10-item measure of psychological distress. There is strong evidence supporting the relationship between the K-10 and a diagnosis of anxiety and depressive disorders (Andrews and Slade, 2001). In the present sample, Cronbach’s alpha was high (α = 0.87).
Sheehan Disability Scales (SDS) (Sheehan, 1983)
The SDS is a 3-item scale measuring functional impairment in (1) work and studies, (2) social life, and (3) family life and home responsibilities. The SDS is associated with high internal consistency (α = 0.89; Leon et al., 1997) and, in the present sample, Cronbach’s α = 0.96.
Cognitive Failures Questionnaire (CFQ) (Broadbent et al., 1982)
The CFQ is a 25-item self-report measure of cognitive deficits noticed when performing everyday tasks, where higher scores indicate a higher incidence of cognitive failures. CFQ scores have been shown to correlate with measures of anxiety and depression (Sullivan and Payne, 2007) and psychometric studies indicate that it has high internal consistency (α = 0.85–0.89) and test-retest reliability (0.82) (Broadbent et al., 1982). In the present sample, Cronbach’s α = 0.95.
Mini International Neuropsychiatric Interview Version 5.0.0 (MINI) (Sheehan et al., 1998)
The MINI is a brief diagnostic interview developed to determine the presence of Axis-I disorders using DSM-IV diagnostic criteria. Psychometric evaluations of the MINI (Lecrubier et al., 1997) indicate it has excellent inter-rater reliability (k = 0.88–1.00) and adequate concurrent validity with the Composite International Diagnostic Interview (CIDI; World Health Organisation, 1990).
Treatment protocol
The treatment protocol used in the present study was based on previous online protocols for depression and anxiety developed by the team (Dear et al., 2011a; Titov et al., 2011a), but the content was revised to provide age-appropriate case examples and examples of the skills.
The program was delivered over 8 weeks and comprised the following components: five online lessons, a summary with homework for each lesson, automatic reminder and notification emails, and a secure email system between the clinician and each participant. Participants also had access to additional online resources about assertiveness skills, challenging beliefs, problem solving, strategies for improving sleep and answers to frequently asked questions about the application of skills described in the lessons and summaries. Participants were also provided with access to a large collection of comments, which were written by past participants and covered the topics covered in each lesson. Importantly, all lesson materials were released sequentially and serially over the 8 weeks and participants were unable to access lessons in later weeks without first having accessed earlier lessons. The structure of the program, content of lessons and timeline for the release of the additional resources is shown in Table 1.
Primary and secondary program content and the timeline for content release.
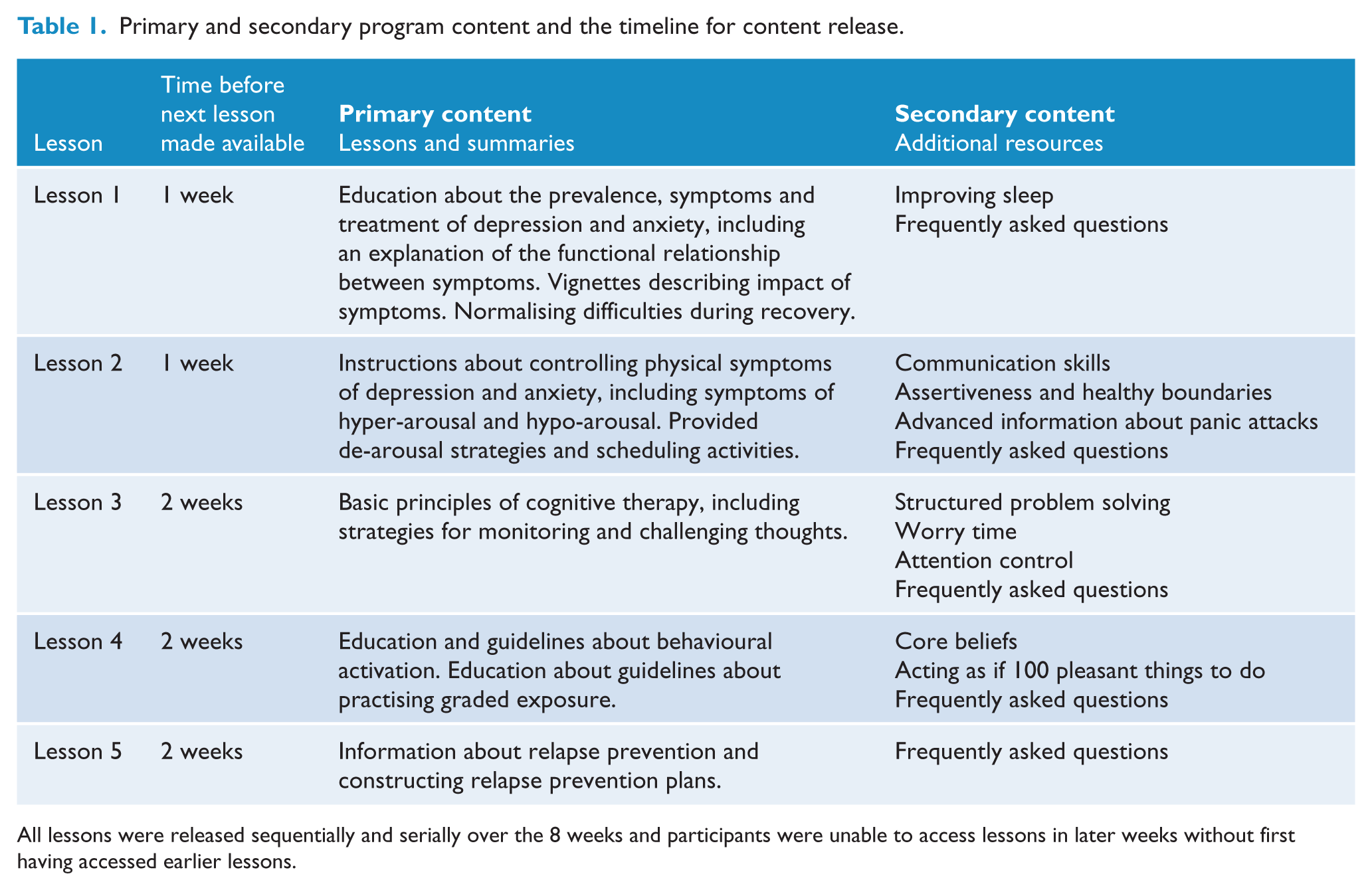
All lessons were released sequentially and serially over the 8 weeks and participants were unable to access lessons in later weeks without first having accessed earlier lessons.
Statistical analyses
All post-treatment analyses involved an intention-to-treat (ITT) design where missing data were addressed by carrying forward the first available data (i.e. baseline-observation-carried-forward model; BOCF). Pre-treatment to post-treatment and post-treatment to follow-up changes in questionnaire scores were analysed using paired-sample t-tests. Effect sizes (Cohen’s d) were calculated for within-group changes using the pooled standard deviation.
Two criteria of clinical significance were employed. First, pre-treatment, post-treatment and follow-up PHQ-9, GDS and GAD-7 scores were compared with clinical cut-offs to provide an index of remission. This was defined as the proportion of participants who initially scored at or above and then subsequently below the following cut-offs: PHQ-9 total score ≥ 10 (Kroenke et al., 2001); GDS ≥ 6 (Jongenelis et al., 2005); and GAD-7 total score ≥ 8 (Löwe et al., 2008). Second an estimate of recovery was made by identifying the proportion of participants in each group who demonstrated a significant reduction in their symptoms (defined here as a reduction of 50% of pre-treatment PHQ-9, GDS or GAD-7 scores), as described in recent dissemination studies (Clarke et al., 2009). A clinically significant change on the GAD-7 was examined because of the significant numbers of participants meeting diagnostic criteria for a comorbid anxiety disorder.
Results
Adherence, attrition, response rates and treatment satisfaction
Sixteen of 20 participants (80%) completed the five lessons within the 8 weeks of the program and the average number of lessons completed was 4.60 (SD = 0.75). One participant (5%) formally withdrew during the program for medical reasons which prevented further participation. Post-treatment and 3-month follow-up data were collected from 17/20 (85%) participants. Participants who completed the post-treatment satisfaction questionnaires reported a high level of satisfaction and 14 participants (82%) said they would recommend the course to a friend and 14 (82%) also reported that the program was worth their time doing.
Primary outcome measures
Paired-sample t-tests comparing pre- and post-treatment scores (see Table 2) revealed significant reductions on the PHQ-9 (t19 = 5.41, p < 0.001) and GDS (t19 = 5.98, p < 0.001). Paired-samples t-tests comparing post-treatment scores with follow-up scores on these primary measures did not reveal any significant changes across the two time points (t19 range = −0.27 to 0.28, p range = 0.78 to 0.79). These significant differences correspond to large within-group effect sizes (d range = 1.41 to 2.04) from pre-treatment to post-treatment and from pre-treatment to follow-up.
Means, standard deviations and effect sizes (Cohen’s d with 95% confidence intervals) of the primary and secondary measures.
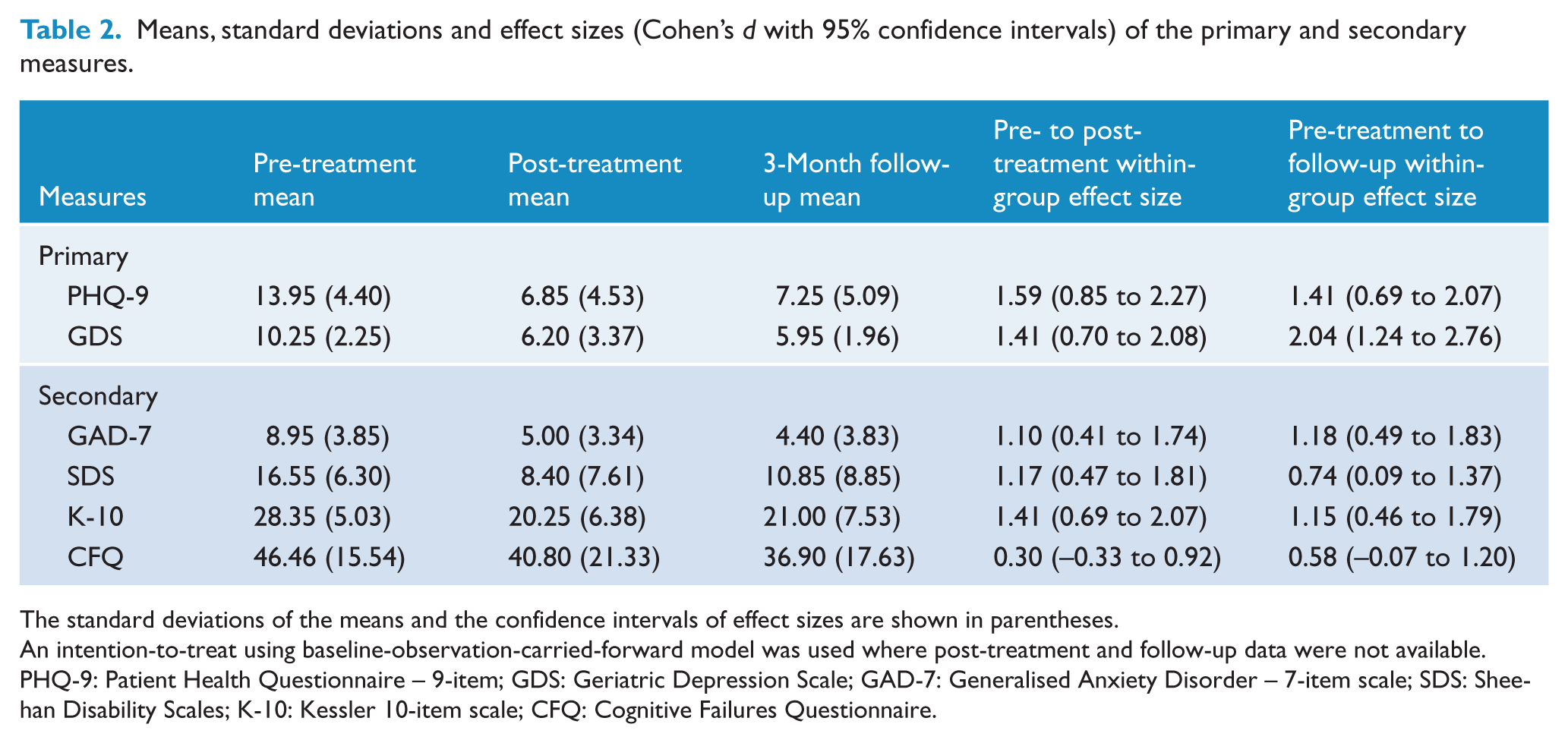
The standard deviations of the means and the confidence intervals of effect sizes are shown in parentheses.
An intention-to-treat using baseline-observation-carried-forward model was used where post-treatment and follow-up data were not available.
PHQ-9: Patient Health Questionnaire – 9-item; GDS: Geriatric Depression Scale; GAD-7: Generalised Anxiety Disorder – 7-item scale; SDS: Sheehan Disability Scales; K-10: Kessler 10-item scale; CFQ: Cognitive Failures Questionnaire.
Secondary outcome measures
Paired-sample t-tests revealed significant reductions from pre-treatment to post-treatment (Table 2) on the GAD-7 (t19 = 4.23, p < 0.001), K-10 (t19 = 5.29, p < 0.001) and the SDS (t19 = 4.12, p < 0.001), but not the CFQ (t19 = 1.24, p = 0.227). Paired sample t-tests revealed no change in scores between post-treatment and follow-up (t19 range = −1.14 to 0.70, p range = 0.26 to 0.66), but a difference emerged between pre-treatment and follow-up scores for the CFQ (t19 = 2.45, p = 0.024).
Within-group effect sizes based on pre-treatment to post-treatment change were large (> 0.80) for the GAD-7, SDS and K-10 (d range = 1.17 to 1.41). Pre-treatment to follow-up effect sizes were large for the GAD-7 and K-10 (d range = 1.15 to 1.18), but moderate for the SDS (d = 0.74). Effect sizes for the CFQ were small from pre-treatment to post-treatment (d = 0.30) and moderate from pre-treatment to follow-up (d = 0.58).
Clinical significance
The numbers and percentages of people scoring above identified cut-offs of clinical significance and achieving at least a 50% reduction in their scores on the PHQ-9, GDS and GAD-7 are shown in Table 3.
Proportion of participants above and below cut-off scores of clinical significance and proportion demonstrating at least 50% reduction in pre-treatment scores.
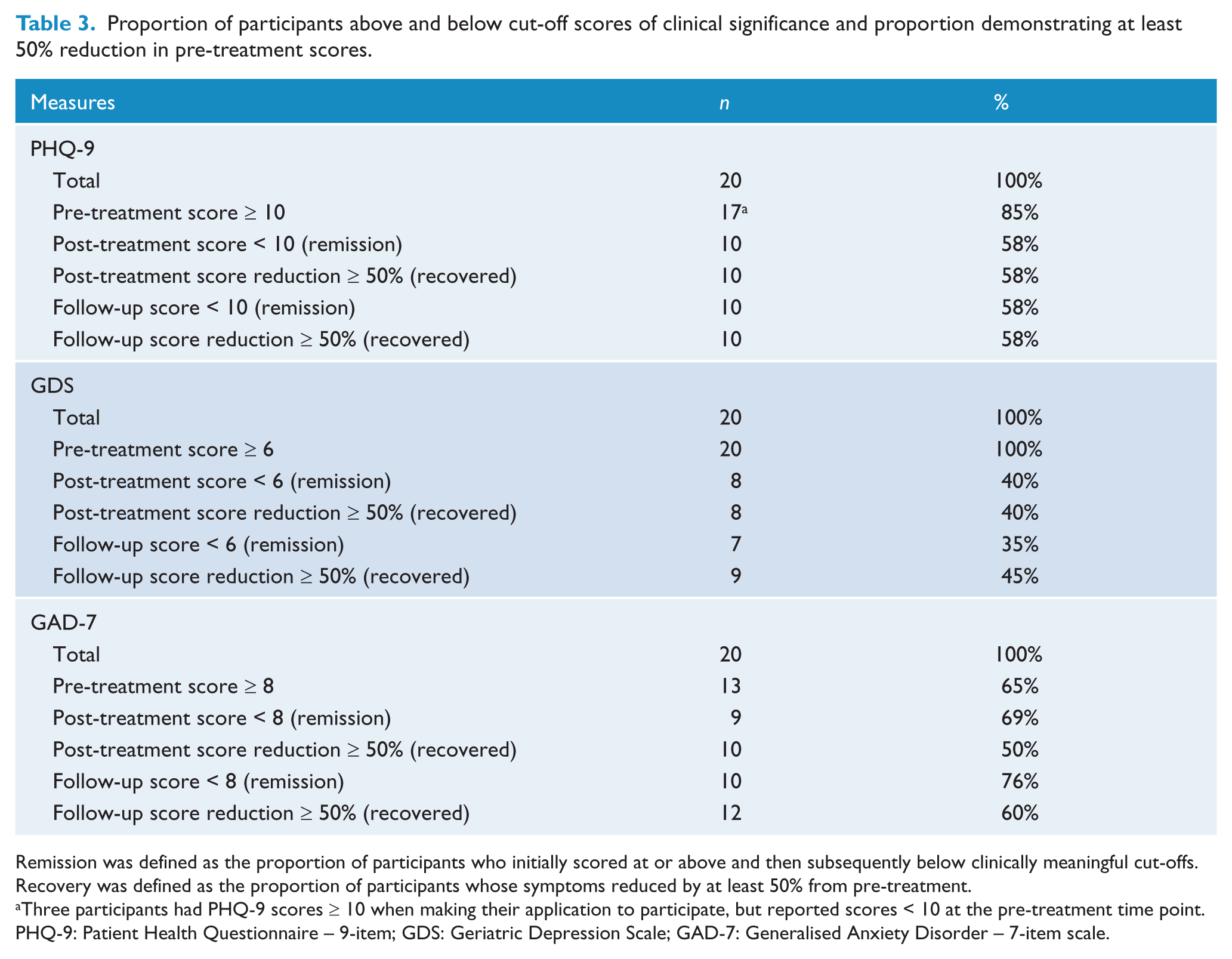
Remission was defined as the proportion of participants who initially scored at or above and then subsequently below clinically meaningful cut-offs.
Recovery was defined as the proportion of participants whose symptoms reduced by at least 50% from pre-treatment.
Three participants had PHQ-9 scores ≥ 10 when making their application to participate, but reported scores < 10 at the pre-treatment time point.
PHQ-9: Patient Health Questionnaire – 9-item; GDS: Geriatric Depression Scale; GAD-7: Generalised Anxiety Disorder – 7-item scale.
Time spent and contact events
The mean total therapist time per participant was 73.75 minutes (SD = 36.10), including sending and reading emails, and telephoning participants. An additional average 40 minutes per participant was required for administrative purposes, including time required to conduct the diagnostic telephone interviews. Participants were sent an average of 16.16 automatic emails (SD = 2.45; total of 323) and an average of 1.6 manual emails (SD = 1.18; total of 32) during the program. The clinician also made a total of 216 telephone calls (mean = 10.8 per participant; SD = 1.64).
Discussion
The primary aims of the present study were to examine the efficacy, acceptability and feasibility of the Managing Your Mood Program, a brief iCBT program for symptoms of depression in adults over the age of 60 years. The Managing Your Mood Program is a five-lesson iCBT program, which is delivered over 8 weeks and, in this trial, was provided with weekly contact from a clinical psychologist. All participants had PHQ-9 total scores ≥ 10 at pre-treatment and 80% met DSM-IV diagnostic criteria for a major depressive episode. It was hypothesised that: (1) participants would show statistically significant improvements on measures of depression, anxiety and functional disability; (2) these changes would be reflected in clinically meaningful improvements on primary measures of anxiety and depression; and (3) participants would rate the program as acceptable. These hypotheses were supported.
Large within-group effect sizes were found on the PHQ-9 and GDS (d range = 1.41 to 2.04), two widely used measures of depression. Large effect sizes were also observed on a general measure of anxiety (GAD-7: d range = 1.10 to 1.18) and a measure of distress (K-10: d range = 1.15 to 1.41). These effects were all maintained from post-treatment to follow-up and were reflected in indices of clinically meaningful change. Specifically, using the PHQ-9, GDS and GAD-7, 40% to 69% of participants were classified as in remission at post-treatment and 40% to 58% were classified as recovered. These results were sustained at follow-up, with 35% to 76% classified as in remission and 45% to 60% classified as recovered. Importantly, these results are similar to those observed in studies evaluating guided-iCBT for depression in adults (Andersson and Cuijpers, 2009) and are also consistent with the findings of the only study to specifically examine an iCBT treatment amongst older adults with subclinical symptoms of depression (Spek et al., 2007). However, these findings extend existing studies by examining the efficacy and acceptability of iCBT for older adults with clinical levels of depression. Significant improvements were also observed on a measure of functional disability, indicating that the improvements generalised to other domains.
Importantly, rates of adherence and participant satisfaction were both high and consistent with those reported for other iCBT treatments (Dear et al., 2011a; Titov et al., 2011a). The results were also obtained with relatively little clinician input (i.e. 73 minutes), indicating the potential of this approach as a cost-effective intervention for older adults with depression. This was achieved by relying on the program to automatically and systematically teach the core skills, while additional resources, which participants could select based on personal preference, addressed other common difficulties experienced by people recovering from depression. The clinician was therefore able to focus on reinforcing progress, normalising difficulties and encouraging participants to continue.
Two additional and important findings to emerge from the present study were the decrease in the numbers of cognitive failures (d = 0.59) reported by participants and the significant improvement in scores on general measures of anxiety (GAD-7: d = 1.10 to 1.18). There is considerable literature describing both the presence of cognitive deficits amongst people with depression (McClintock et al., 2010) and a relationship between self-reported numbers of cognitive errors in day-to-day activities and levels of depression (Sullivan and Payne, 2007). Although it is still unclear whether the greater numbers of cognitive failures reported by people with depression reflects an increased tendency to make mistakes or the general pessimistic self-evaluations of their functioning or both (van Doorn et al., 2010), the magnitude of perceived improvements in cognitive function are encouraging. Similarly, the intervention appeared to improve symptoms of anxiety, even though the program did not specifically target anxiety. These findings are consistent with data indicating the transdiagnostic effects of CBT, and the fact that many participants also met criteria for anxiety disorders, suggest older adults might benefit from transdiagnostic iCBT programs similar to those used successfully with younger adults (Dear et al., 2011a; Titov et al., 2011a).
The present study has a number of important limitations. First, it was an uncontrolled open trial with a relatively small sample and, while the results are consistent with similar iCBT programs for depression (Titov et al., 2011a), an evaluation of this program using a stronger research design is required. Second, with an average age of 63 years and being well educated, the sample of older adults used in the present study was at the younger end of the spectrum of elderly individuals. It is therefore unclear how the results of the present study would generalise to older groups who, for example, may have more comorbid serious physical medical conditions (e.g. stroke, arthritis, etc.) or might be less familiar with internet use. In addition, the present study employed clinician support and an internet-treatment seeking group, which may limit the generalisability of the findings. On the other hand, 80% of the sample had received some form of mental health treatment in the past and so constitute a treatment-seeking sample. Last, some caution is needed concerning the interpretation of the effect sizes observed given the small sample size employed and the broad confidence intervals observed for some measures. Nevertheless, given the promising findings of this trial and its limitations, future studies will examine the efficacy of iCBT amongst older adults using a randomised controlled trial (RCT) design comparing both guided and self-guided versions.
In summary, the Managing Your Mood Program obtained large effect sizes on established measures of depression and anxiety, which were sustained at the 3-month follow-up and were consistent with the outcomes of similar previous studies of guided iCBT programs amongst younger adults. The levels of program completion and acceptability were also high. Overall, the findings of the present study are encouraging regarding the use of iCBT with older adults and large RCTs evaluating the program are underway.
Footnotes
Funding
This project was funded by a Strategic Research Grant from beyondblue: The National Depression Initiative. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of interest
None declared.
Contributors
BFD drafted the treatment protocol, supervised the trial, conducted the analyses and drafted the manuscript. NT designed the study, drafted the treatment protocol, supervised the trial, conducted the analyses and drafted the manuscript. JZ was the clinician in the trial, reviewed the treatment protocol and reviewed the manuscript. CL, LJ and JS assisted in the running of the trial and reviewed the manuscript. TA, PS, HB and RGK reviewed and contributed to the manuscript. All authors have contributed to and have approved the manuscript.