
Abstract
Objective:
Most patients with bipolar disorder experience depressive symptoms outside of an episode of depression as defined by DSM-IV criteria. This study explores the frequency of brief depressive episodes, lasting 1 to 4 days, using daily self-reported mood ratings.
Method:
Mood ratings were obtained from 448 patients (281 bipolar I, 167 bipolar II) using ChronoRecord software (91,786 total days). Episodes of depression and days of depression outside of episodes were determined. The intensity of depressive symptoms (mild versus moderate to severe) was compared.
Results:
Using the DSM-IV length criteria, 61% of all depressive days occurred outside of a depressed episode. Decreasing the minimum length criterion to 2 days, both the number of patients experiencing a depressed episode (128 to 317) and the mean percent of days spent in a depressed episode by each patient (7.9% to 17.8.%) increased by about 2½ times, and 34.3% of depressed days remained outside of an episode. Depending on the episode length, the proportion of days within an episode with severe symptoms varied from ⅓ to ¼ for episodes lasting from 14 to 2 days, and ¼ for single-day episodes. There was no significant difference in the frequency of brief depressive episodes between bipolar I and II disorders. For all episode lengths, patients taking antidepressants spent 4% more days within an episode and 6% more days with depressive symptoms outside of an episode than those not taking antidepressants.
Conclusion:
Brief depressive episodes lasting 1 to 4 days occur frequently in bipolar disorder and do not distinguish between bipolar I and II disorders. Symptoms of moderate to severe intensity occur on ¼ to ⅓ of the days in brief depressive episodes. This study did not address brief depression in those without bipolar disorder. Patients taking antidepressants experienced more brief depressive episodes. Controlled trials are needed to assess the impact of antidepressants on subsyndromal depressive symptoms.
Introduction
Depressive symptoms predominate in most patients with bipolar disorder (Baldessarini et al., 2010; Judd et al., 2002, 2003a; Post et al., 2003). Frequently, these depressive symptoms are brief in duration, do not meet the criteria for a DSM-IV episode of depression, and are referred to as subsyndromal or subthreshold symptoms (Angst and Merikangas, 1997; Bauer et al., 2007; Judd et al., 2002, 2003a; Paykel et al., 2006). Subsyndromal depressive symptoms are associated with considerable functional and psychosocial impairment (Altshuler et al., 2002; Bauer et al., 2009; Goldberg and Harrow, 2011; Judd et al., 2005; Marangell et al 2009), and an increased risk of relapse (Perlis et al., 2006). We previously investigated the occurrence of brief depressive episodes lasting 2–4 days using daily self-reported data from 203 patients who were diagnosed with bipolar disorder (Bauer et al., 2007). We found that brief depressive episodes occurred frequently in both bipolar I and bipolar II disorder, and that symptoms of severe intensity occur during brief episodes in the same proportion as in episodes that meet the DSM-IV criteria. The purpose of this study is to repeat the prior analysis using a larger sample, to include a length criterion of a single day, and to further characterize the brief depressive episodes that occur in bipolar disorder.
Methods
All participants were outpatients, aged 18 years or older, with a diagnosis of bipolar disorder by DSM-IV criteria that was made by the prescribing psychiatrist during a clinical interview. The participants agreed to record mood daily for 6 months using computer software in their native language (ChronoRecord Association, Inc., Fullerton, CA, USA). All participants volunteered, provided informed written consent, and received pharmacological treatment as usual throughout the study. The participants were recruited from university mood clinics by the participating physicians, or by word of mouth, and received no compensation other than being allowed to use the software indefinitely. Data from our prior investigation (Bauer et al., 2007) were included in this analysis, although some patients provided additional data.
Daily mood ratings
All mood ratings were self-reported daily using Chrono Record software. ChronoRecord was previously validated with the Hamilton Depression Rating Scale (HAMD) and Young Mania Rating Scale (YMRS), as described elsewhere (Bauer et al., 2004, 2008). To record mood, ChronoRecord contains a 100-unit visual analogue scale between the extremes of mania and depression. During a half-hour training session, personal anchor points were set by the patient to describe the most depressed and most manic states they ever experienced. The patient’s anchor point for mania, and daily self-ratings of mania or hypomania reflect activation levels for either euphoric or dysphoric mood (Bauer et al., 2004). The patients were instructed to enter a single daily mood rating that best described their overall mood for the prior 24 hours, and to calibrate the rating to their anchor points. Based upon the validation studies (Bauer et al., 2004, 2008), a mood entry less than 40 was considered depression, 40–60 euthymia, and greater than 60 hypomania/mania. The range of depression varied between mild symptoms (an entry of 20–39) to moderate to severe symptoms (an entry of 0–19). The range of mania varied from hypomania (an entry of 61–80) to moderate to severe symptoms of mania (an entry of 81–100). Every day, the patients also recorded their sleep, medications taken and any significant life events.
Data
Data were collected from 513 patients with bipolar disorder who resided in the USA (361, 71%), Canada (58, 11%), Germany (55, 11%), Poland (16, 3%), Chile (12, 2%) and Australia (11, 2%). The demographic characteristics of the 513 patients were compared with other published studies of patients with bipolar disorder in Table 1. Although the patient sample in this study contains somewhat more females and members of an ethnic minority, the demographic profile of the patients in this study was similar to that of patients in other studies of bipolar disorder.
Comparison of patient demographics with other studies of bipolar disorder.
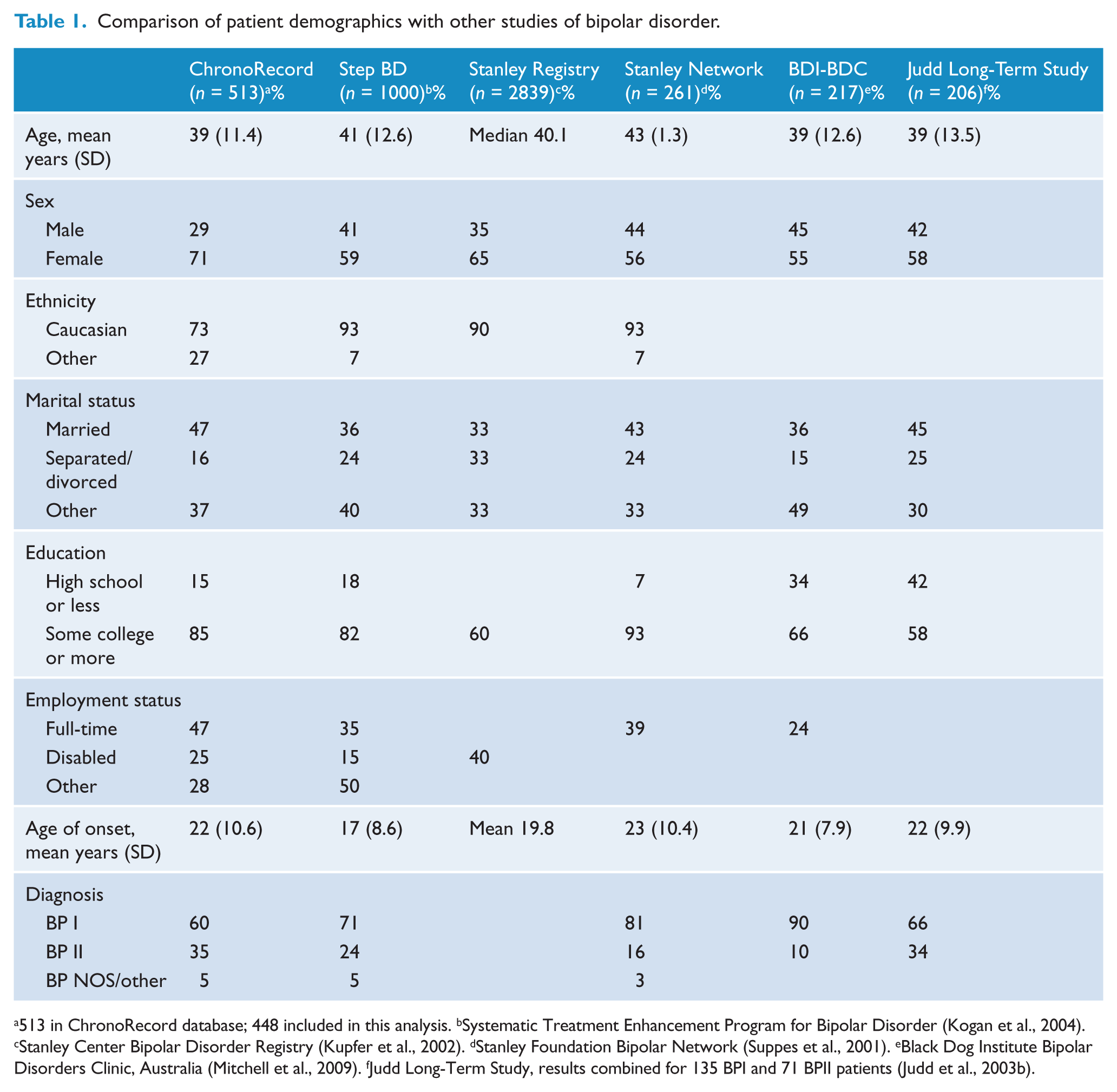
513 in ChronoRecord database; 448 included in this analysis. bSystematic Treatment Enhancement Program for Bipolar Disorder (Kogan et al., 2004). cStanley Center Bipolar Disorder Registry (Kupfer et al., 2002). dStanley Foundation Bipolar Network (Suppes et al., 2001). eBlack Dog Institute Bipolar Disorders Clinic, Australia (Mitchell et al., 2009). fJudd Long-Term Study, results combined for 135 BPI and 71 BPII patients (Judd et al., 2003b).
Statistical analysis
The demographic characteristics, mood ratings, and psychotropic medications taken by the patients were obtained. Patients were included in this analysis if they returned a minimum of 150 days of data. To be considered using a medication, a patient had to take any dose of the drug for at least 50% of the days. The demographic characteristics and medications of the patients with bipolar I and bipolar II disorder were compared using chi-squared tests for frequency of categorical variables, or independent t-tests for mean values of continuous variables. Unequal variance was assumed for all t-tests. Episodes of hypomania and depression based on the DSM-IV length criteria were determined for each patient using a published algorithm to calculate episodes from daily self-reported mood data (Denicoff et al., 1997). The episodes were then re-calculated using minimum length criteria of 4, 3, 2, and 1 days. As the episode duration was decreased, the mean percent of days in a depressed episode was compared with that for 14 days using pairwise t-tests for all patients. When comparing the mean percent of days in a depressed episode between groups (bipolar I or bipolar II, and patients taking or not taking antidepressants), independent t-tests were used. A p-value of less than 0.05 was considered statistically significant for all tests. SPSS 20.0 was used for all calculations.
Results
A total of 469 unique patients provided sufficient data to be included in the study: 281 with a diagnosis of bipolar I disorder, 167 with bipolar II disorder, and 21 with bipolar NOS. The small group with a diagnosis of bipolar NOS was excluded, so a total of 448 patients were included in the analysis. The 448 patients returned a total of 91,786 days of data (mean 204.9). There was no significant difference in the mean days of data returned when comparing those with bipolar I or II disorder (191.9 versus 226.7, p = 0.308), or those taking or not taking antidepressants (189.9 versus 219.6, p = 0.333). The demographic characteristics of the 448 patients are shown in Table 2, comparing the patients with bipolar I and bipolar II disorder. The patients with bipolar I disorder had more hospitalizations (2.8 (SD 4.1) versus 1.7 (SD 4.2), p = 0.015), were less likely to be female (184, 66% versus 126, 75%, p = 0.027), were less likely to be taking antidepressants (118, 42% versus 104, 62%, p < 0.001) or lamotrigine (91, 32% versus 76, 46%, p = 0.005) and more likely to take lithium (87, 31% versus 32, 19%, p = 0.006) than those with bipolar II disorder. No other significant differences in demographic characteristics or medications were found between those with bipolar I and bipolar II disorder.
Patient demographics (n = 448).
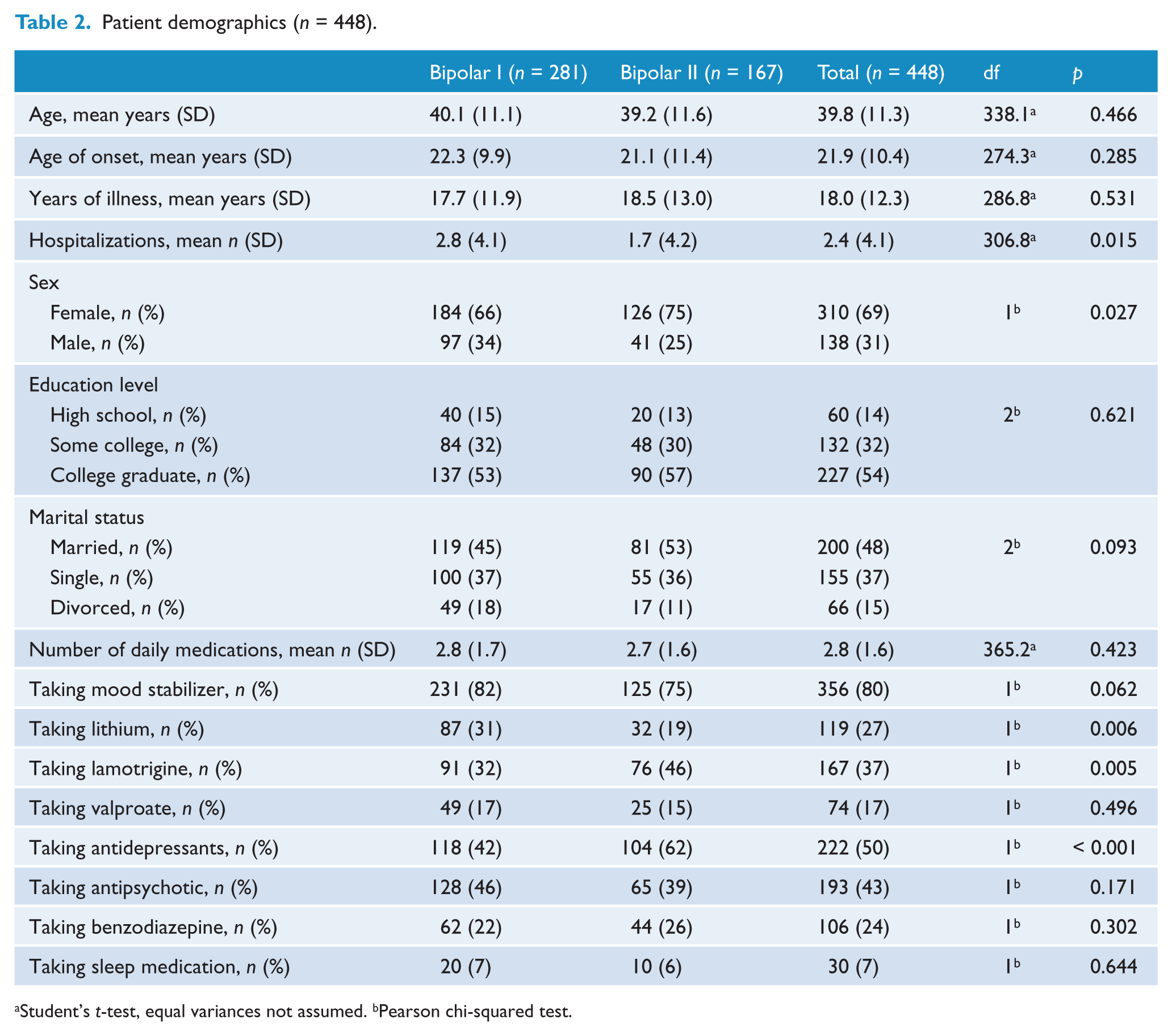
Student’s t-test, equal variances not assumed. bPearson chi-squared test.
Of the total 91,786 days of data from all patients, 18,845 (21%) were rated as depressed. Using the DSM-IV criteria, 128 (29%) patients experienced at least one depressed episode, with 39% of the 18,845 depressed days occurring within a depressed episode and 61% outside of an episode. Table 3 presents the effects of decreasing the minimum length criteria for an episode of depression. When the minimum episode length was decreased from 14 to 2 days, there was an increase of about 2½ times in both the number of patients experiencing a depressed episode (128 to 317) and the mean percent of days spent in a depressed episode by each patient (7.9% to 17.8%). When the minimum episode length was decreased to 2 days, 65.7% of depressed days occurred in a depressed episode and 34.3% outside of an episode. When the minimum episode length was decreased from 14 days to 1 day, the number of patients experiencing a depressed episode tripled (128 to 381), and the mean percent of days spent in a depressed episode by each patient was more than 2½ times greater (7.9% to 20.8%). With a 1-day length, some depressed days remained in hypomanic episodes based on the algorithm. Using data from all patients, the increase in the mean percent of days spent in an episode as the minimum length decreased was significant in all cases (p < 0.001 for all pairwise comparisons).
Impact of changing the minimum episode length for depression on patients with bipolar disorder (n = 448).
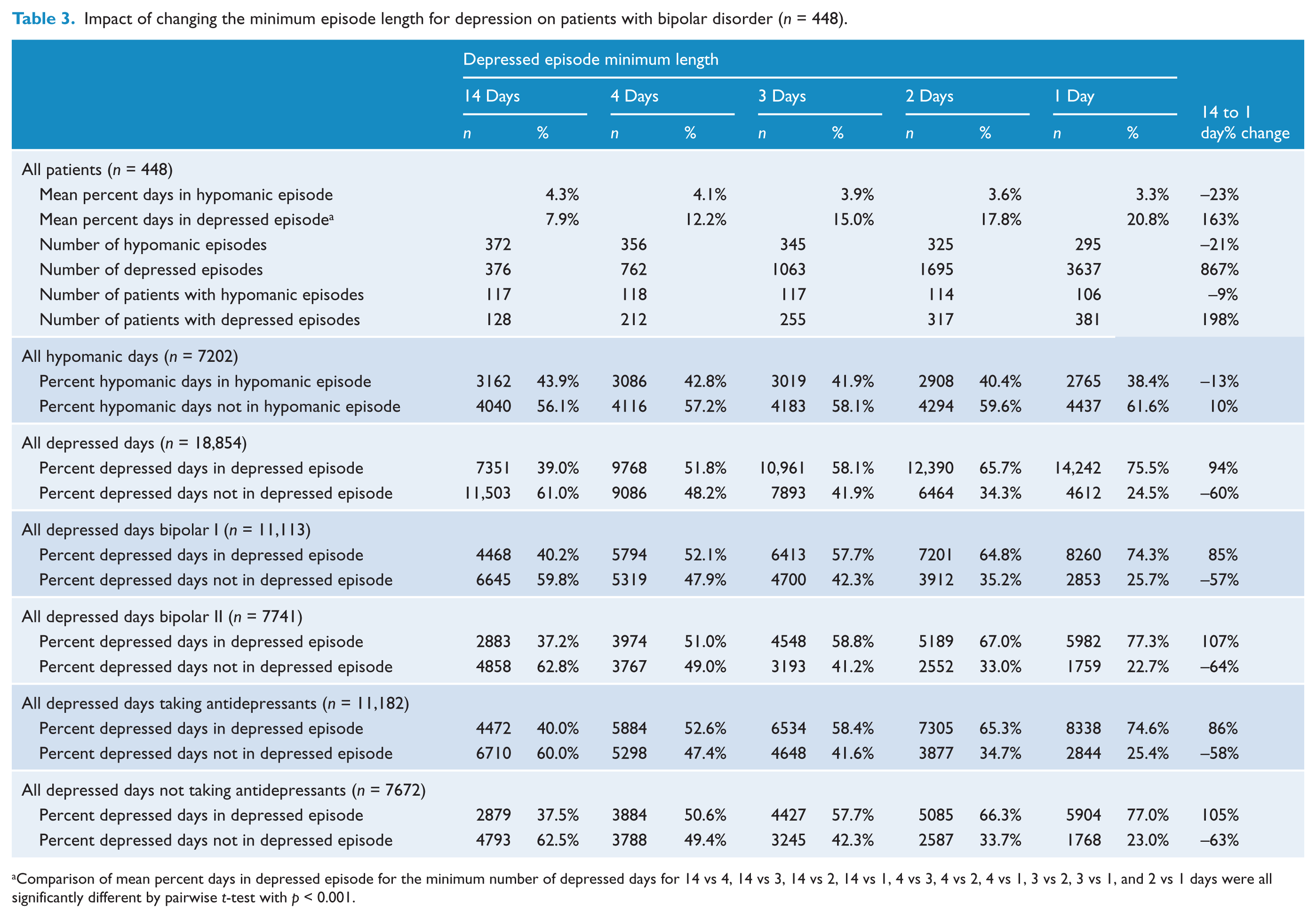
Comparison of mean percent days in depressed episode for the minimum number of depressed days for 14 vs 4, 14 vs 3, 14 vs 2, 14 vs 1, 4 vs 3, 4 vs 2, 4 vs 1, 3 vs 2, 3 vs 1, and 2 vs 1 days were all significantly different by pairwise t-test with p < 0.001.
Of the total 18,854 depressed days, 4473 (24%) were rated as having moderate to severe intensity. Using a 14-day episode length, only 2505 (56%) of the 4473 days with severe symptoms occurred within a depressed episode. As shown in Table 4, patients routinely experienced symptoms of moderate to severe intensity outside of DSM-IV episodes. For patients with bipolar I disorder, the proportion of days with severe symptoms within an episode ranged from 33.8% with an episode length of 14 days to 25.7% with an episode length of 2 days, and 23.0% for an episode length of 1 day. For patients with bipolar II disorder, the proportion of days with severe symptoms within an episode ranged from 34.5% with an episode length of 14 days to 27.7% with an episode length of 2 days, and 25.0% for an episode length of 1 day. The pattern of change was also similar when comparing patients taking or not taking antidepressants. Depending on the episode length, patients reported severe symptoms on about ¼–⅓ of all days within episodes lasting 2–4 days, and on ¼ of single-day episodes (Figure 1).
Impact of changing the minimum episode length on symptom severity (n = 448).
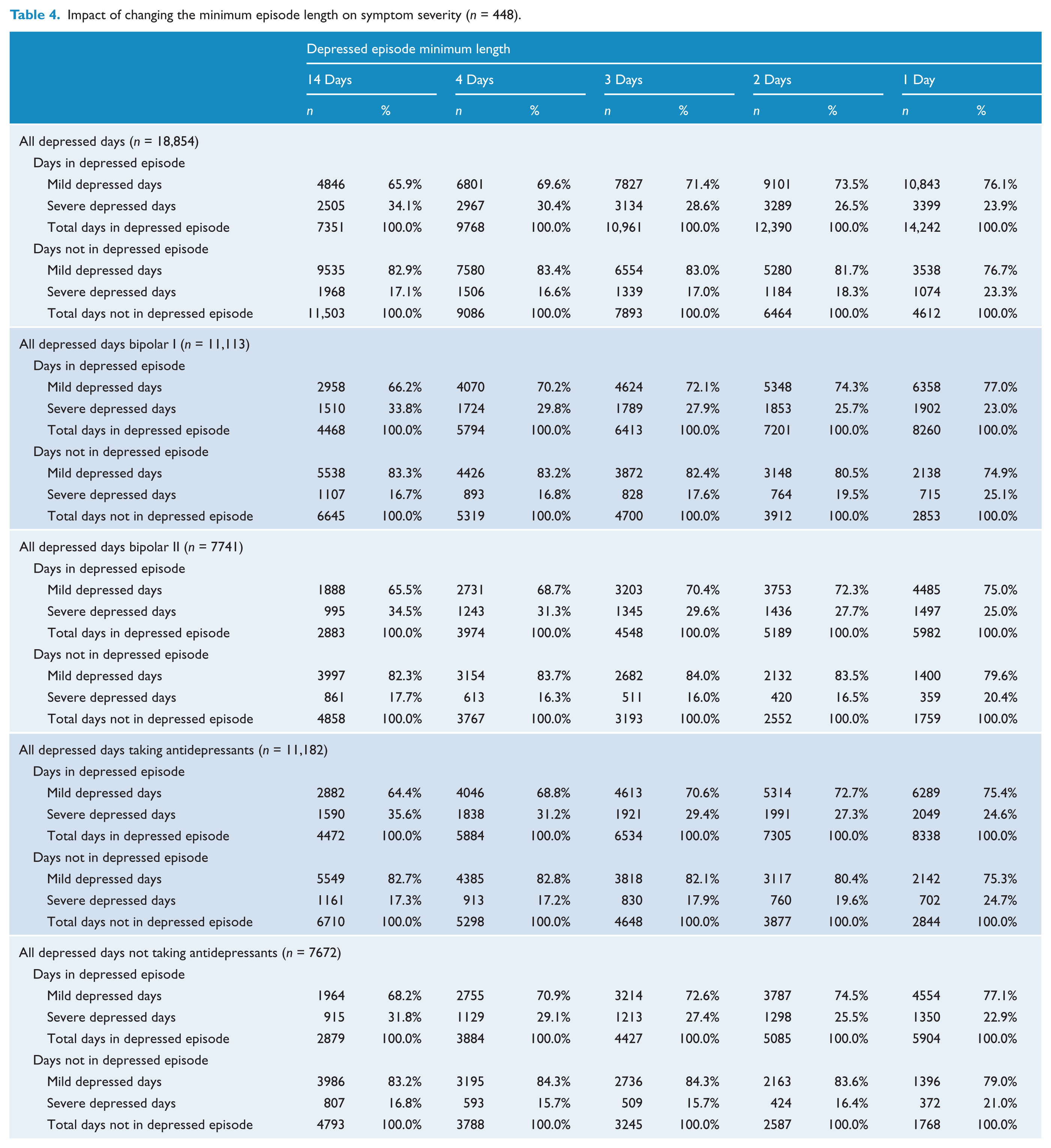
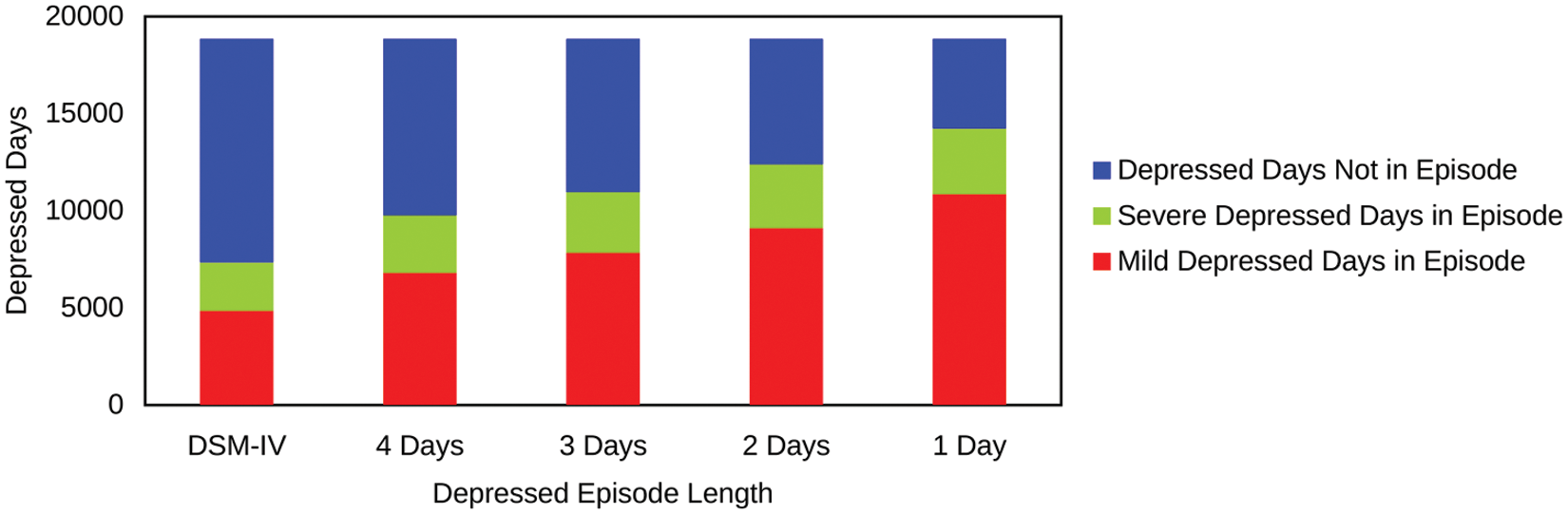
Distribution of depressed days by episode length and severity in patients with bipolar disorder.
Regardless of episode length, there was no significant difference in the distribution of patients with at least one episode between those taking or not taking antidepressants. However, patients taking antidepressants reported a larger mean percent of depressed days, when considering all days both within and outside of an episode, than those not taking antidepressants (26.6% versus 18.8%, p = 0.001). The mean percent of days spent in a depressed episode was significantly larger for patients taking antidepressants by about 4% for all episode lengths (Table 5A). The mean percent of depressed days outside of an episode was also significantly larger for patients taking antidepressants by about 6% for all episode lengths (Table 6A). However, for any episode length, there was no significant difference in the mean percent of days with severe symptoms outside of an episode between those taking and not taking antidepressants (Table 6B).
Percent of days in a depressed episode by episode length and taking antidepressants (n = 448).
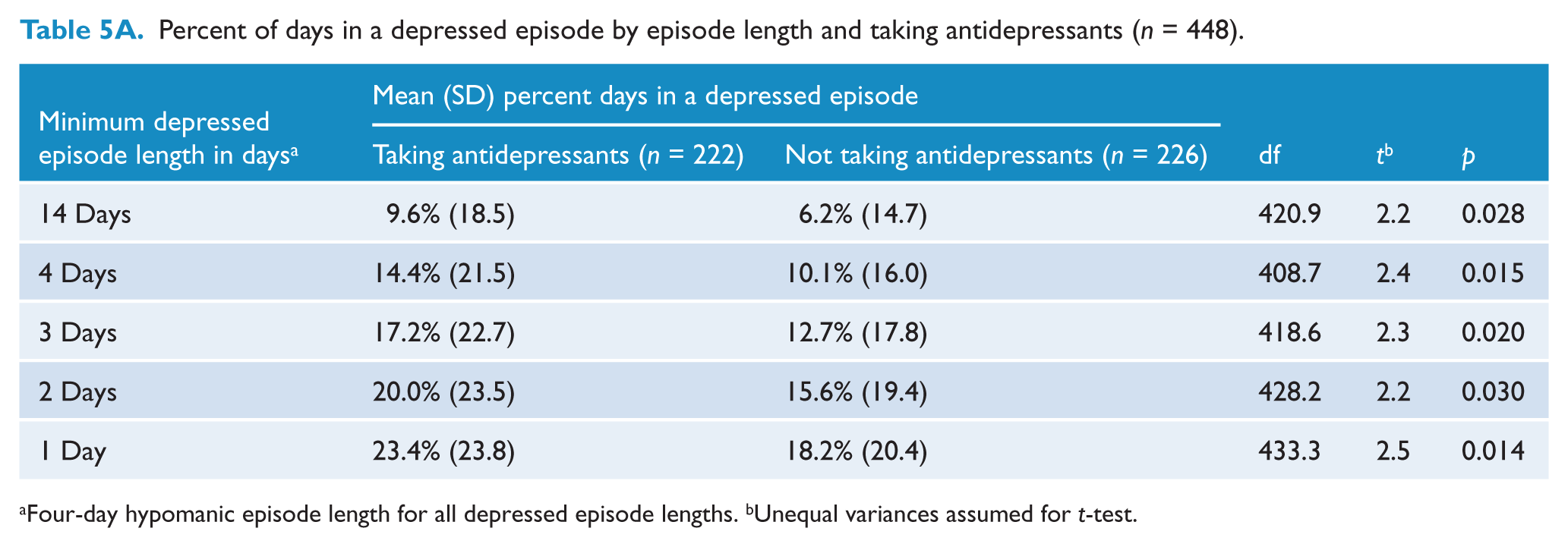
Four-day hypomanic episode length for all depressed episode lengths. bUnequal variances assumed for t-test.
Percent of days in a depressed episode by episode length and diagnosis (n = 448).
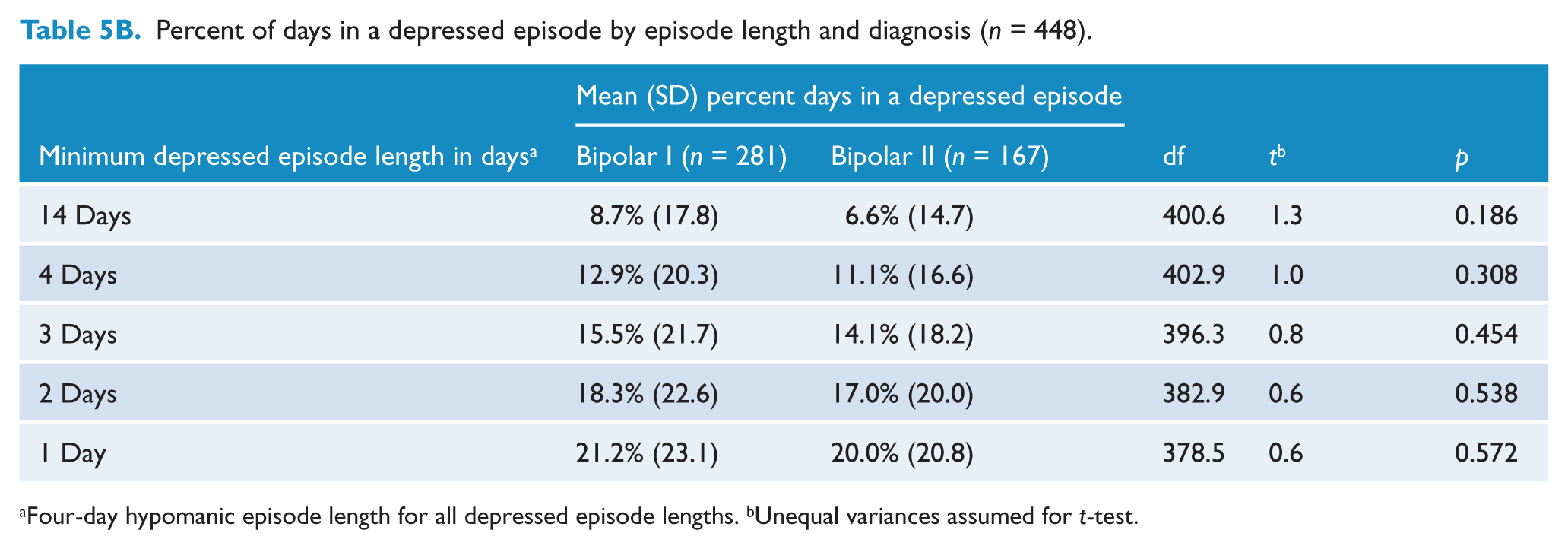
Four-day hypomanic episode length for all depressed episode lengths. bUnequal variances assumed for t-test.
Percent of depressed days not in a depressed episode-by-episode length and taking antidepressants (n = 448).
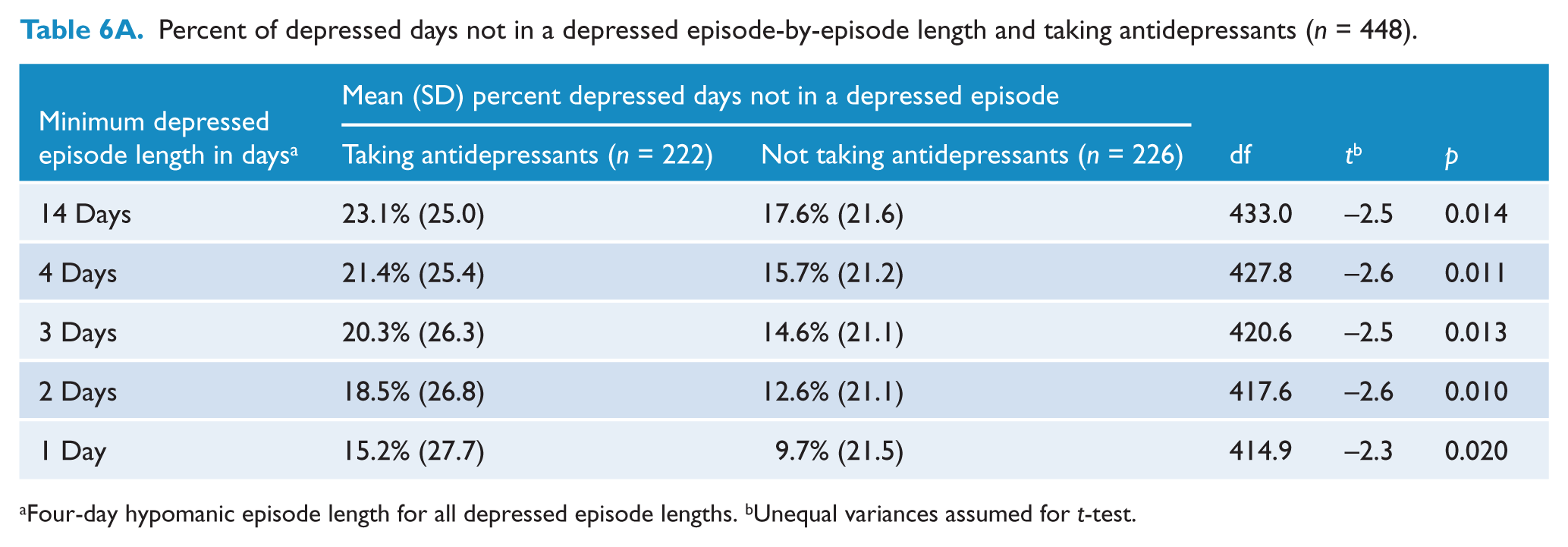
Four-day hypomanic episode length for all depressed episode lengths. bUnequal variances assumed for t-test.
Percent of severe depressed days not in a depressed episode-by-episode length and taking antidepressants (n = 448).
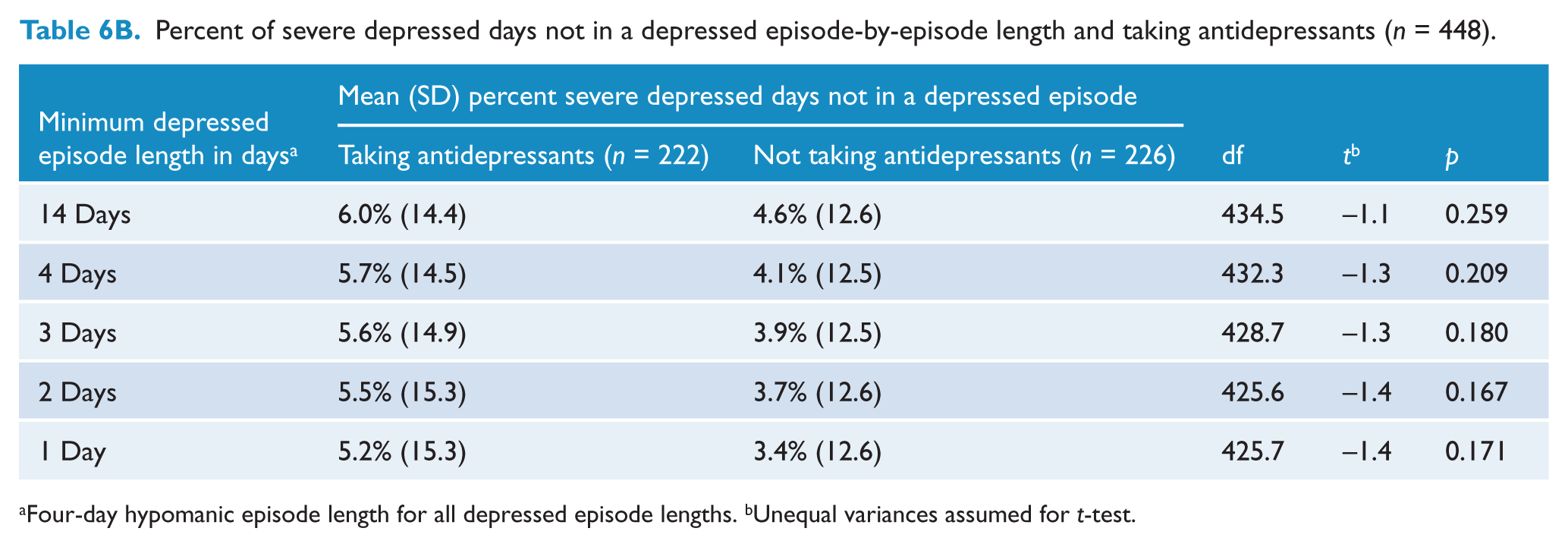
Four-day hypomanic episode length for all depressed episode lengths. bUnequal variances assumed for t-test.
When considering all days both within and outside of an episode, there was no significant difference between the mean percent of depressed days between patients with bipolar I and bipolar II disorders (22.0% versus 24.5%, p = 0.586). There was also no significant difference between the mean percent of days spent in a depressed episode of any length between patients with bipolar I and bipolar II disorders (Table 5B).
Discussion
Brief depressive episodes lasting between 1 and 4 days occurred frequently in this study of patients with bipolar disorder. In fact, 61% of all days of depression occurred outside of a depressed episode when using the 14-day DSM-IV length criterion. This high frequency of subsyndromal depression in bipolar disorder is consistent with prior research in which diverse methodologies were used to measure symptoms (Angst and Merikangas 1997; Bauer et al., 2010; Judd et al., 2002, 2003a). The occurrence of brief depressive episodes could not be used to differentiate between a diagnosis of bipolar I and bipolar II disorder, as with prior findings (Bauer et al., 2007; Kupka et al., 2007; Marangell et al., 2009).
Frequent brief depressive episodes are of concern for many reasons. Depressive symptoms, rather than manic symptoms, are the primary determinant of the quality of life in bipolar disorder (Bowie et al., 2010; Michalak et al., 2008; Vojta et al., 2001). Moreover, the functional burden due to subsyndromal depressive symptoms is similar to that from an episode of depression (Judd et al., 2005; Marangell et al., 2009). Subsyndromal depressive symptoms are equally impairing in both bipolar I and bipolar II disorder (Judd et al., 2005), and are a predictor of both disability (Bowie et al., 2010; Judd et al., 2005; Simon et al., 2007) and reduced quality of life (Michalak et al., 2008). Furthermore, the total time spent symptomatic may be a better predictor of psychosocial functioning than the total number of episodes, suggesting a cumulative effect from all prior symptoms whether within or outside of an episode (Bauer et al., 2001, Bauer et al., 2010; Gitlin et al., 1995; Goldberg and Harrow, 2004). Subsyndromal depressive symptoms are also associated with an increased risk of relapse (Perlis et al., 2006). In a prior analysis of daily patient mood ratings using the DSM-IV criteria, significantly increased irregularity in mood occurred in the 60 days prior to an episode (Bauer et al., 2011).
In agreement with prior research, most of the depressive symptoms in the current study were mild in intensity (Judd et al., 2002, 2003a; Paykel et al., 2006). The proportion of days within an episode with moderate to severe symptoms was about ⅓ for episodes that met the DSM-IV criteria. The proportion remained about ⅓ within a 4-day episode, decreasing to about ¼ for a single-day length. This pattern of symptom intensity was similar regardless of diagnosis of bipolar I or II, or if patients were taking or not taking antidepressants. Symptom intensity during brief depressive episodes is important since even modest increases in the severity of depression are associated with a significant increase in functional impairment and disability (Simon et al., 2007). Patient perception of severity of depressive symptoms is also associated with suicidal behaviour in patients with bipolar disorder (Oquendo et al., 2004). Furthermore, the co-occurrence of brief recurrent depression increases the risk for suicidal behaviour in patients with unipolar depression (Altamura et al., 2011; Pezawas et al., 2005).
About 50% of the patients in this study were taking antidepressants, similar to prior reports of patients with bipolar disorder in the USA and Europe (Baldessarini et al., 2007, 2008; Morselli et al., 2003). As in other observational studies, patients taking antidepressants experienced depressive symptoms more frequently than those not taking antidepressants (Bauer et al., 2007; Post et al., 2003). In this study, patients taking antidepressants spent about 4% more days within an episode of depression and 6% more days with depressive symptoms outside of an episode, regardless of episode length. The association between increased subsyndromal depressive symptoms and taking antidepressants in this observational study does not imply causality. Although one possible hypothesis is that antidepressant use may contribute to the increase in subsyndromal symptoms, a reverse causality argument would suggest that increased vulnerability to depression leads to an increased use of antidepressants. Furthermore, many confounding factors beyond the scope of this study may contribute to both depressive symptoms and antidepressant use, such as substance abuse or anxiety disorders, general medical health, or economic status. The treatment of bipolar depression with antidepressants remains controversial (Fava, 2003; Gijsman et al., 2004; Goldberg and Ghaemi, 2005; Licht et al., 2008). However, given the widespread use of antidepressants, including 11% of Americans over the age of 12 years in a national sample of 14,000 (Pratt et al., 2011), there is a need for controlled trials of the impact of antidepressants on subsyndromal depressive symptoms in affective disorders.
One strength of the present study is that the results are consistent with our earlier findings, using a sample that is about double in size (Bauer et al., 2007). Another strength is that daily mood ratings were obtained prospectively from a relatively large number of patients using validated software. There are also several limitations. While an observational study reflects the heterogeneity of patients in clinical practice, patients varied in severity, phase of the disorder, symptoms experienced, and in medications taken. We can only assume, but cannot confirm, that the patients taking antidepressants were more depressed when they began taking antidepressants and have since improved. There were fewer patients with bipolar II than bipolar I disorder in the study, fewer males than females, and only outpatients were included. Other limitations include the use of self-reported mood ratings and the requirement for computer access. Although self-reporting may affect the variable being monitored, recent research did not find significant evidence of measurement reactivity with daily ratings, including depression (Hufford et al., 2002; Lenderking et al., 2008; Simpson et al., 2005). A longer data collection period from each patient would be preferable. This study did not address the frequency of brief depressive symptoms in individuals with bipolar disorder who were not taking medication. Finally, there were no control groups, so this study cannot compare the frequency or severity of brief depression with conditions other than bipolar disorder. Future research on brief depression in those without psychopathology and with other psychiatric disorders is needed.
In conclusion, most patients with bipolar disorder experience brief depressive symptoms lasting between 1 and 4 days, regardless of a diagnosis of bipolar I or bipolar II disorder. Symptoms of moderate to severe intensity occur on ¼ to ⅓ of days in these brief depressive episodes. Patients taking antidepressants experience brief depressive symptoms more frequently. Controlled trials to explore the impact of antidepressants on subsyndromal depressive symptoms are indicated.
Footnotes
Funding
This project was funded entirely by local university funds.
Declaration of interest
The ChronoRecord Association is a 501(c)(3) nonprofit organization that aims to increase understanding of mood disorders (![]() ). None of the authors receive financial compensation from the Association. Tasha Glenn and Peter C Whybrow share a US patent for ChronoRecord software. Michael Bauer, Paul Grof and Peter C Whybrow are on the Medical Advisory Board.
). None of the authors receive financial compensation from the Association. Tasha Glenn and Peter C Whybrow share a US patent for ChronoRecord software. Michael Bauer, Paul Grof and Peter C Whybrow are on the Medical Advisory Board.