
Abstract

To the Editor
The Composite International Diagnostic Interview (CIDI) is a standardized, structured diagnostic interview for the assessment of mental disorders. It was designed to be used by trained lay interviewers to conduct epidemiological surveys and there is also a computerized version (CIDI-Auto). However, the validity of CIDI diagnosis has been questioned, and some previous studies have shown an inadequate level of agreement with clinical diagnosis (Komiti et al., 2001).
In the present study, a file review of a consecutive sample of patients who attended a psychiatric outpatient clinic was conducted. The CADE clinic specializes in the diagnostic evaluation of outpatients referred by general practitioners and psychiatrists. Patients completed the CIDI-Auto, had a clinical interview with a psychiatrist or senior trainee psychiatrist, and diagnostic agreement was achieved by consensus in a clinical meeting with researchers and clinicians. Consensus with CIDI diagnoses was recorded (agree or disagree).
In total, there was sufficient data to include 52 patients from the 71 files examined. For these patients, 196 diagnoses were generated by CIDI (a mean of 3.8 diagnoses per patient) across seven categories of disorder (Table 1). Clinicians assigned a mean of 2.3 diagnoses per patient and disagreement with CIDI diagnoses was common. No mention was made of agreement or disagreement for 61 CIDI-generated diagnoses.
CIDI-generated diagnoses and rate of clinical disagreement
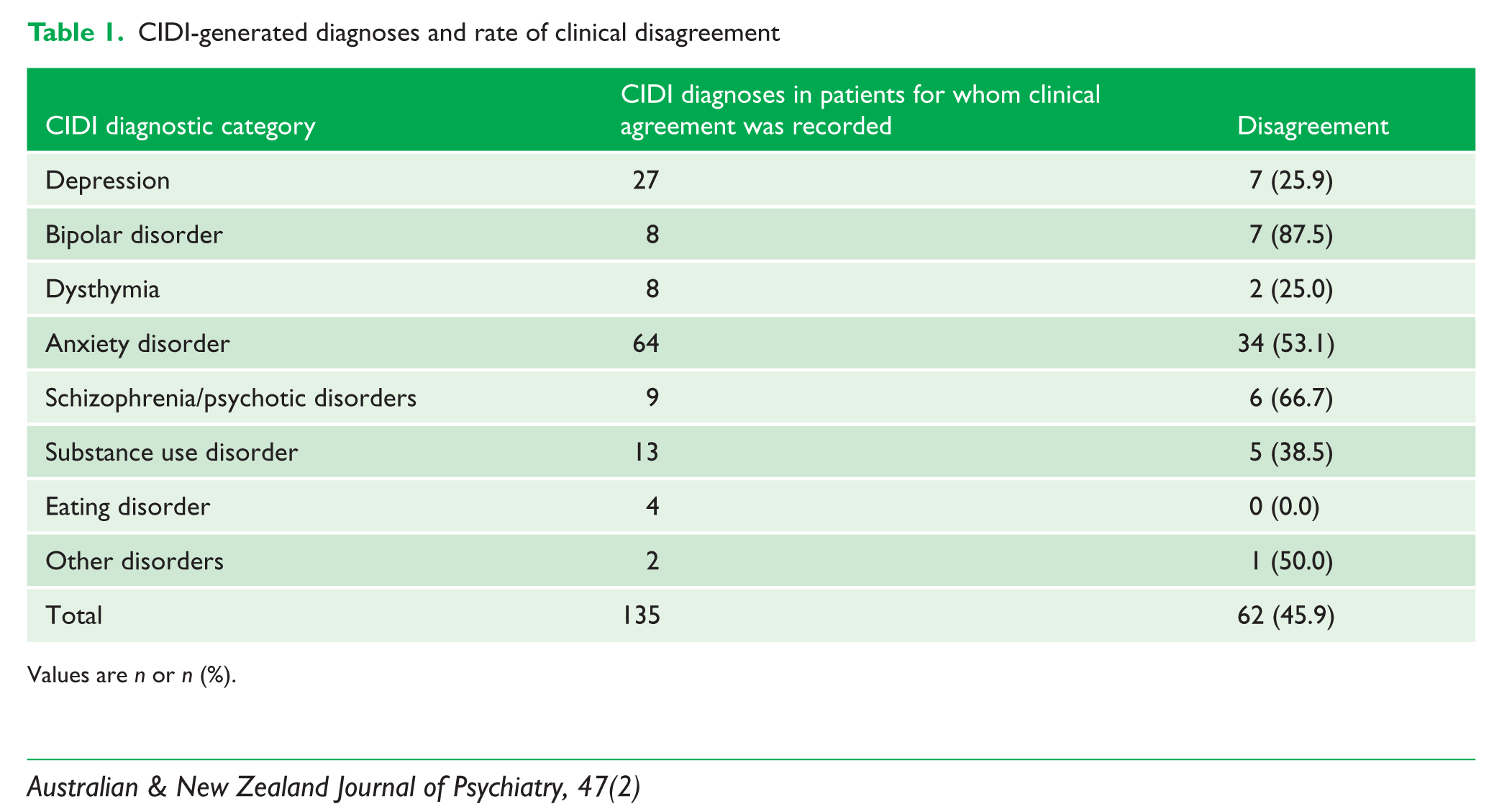
Values are n or n (%).
Possible causes for the poor level of agreement were considered. In the category with the highest level of disagreement, bipolar disorder, clinicians preferred a diagnosis of bipolar II disorder to the bipolar I disorder diagnosis assigned by the CIDI in four our of seven cases of disagreement, and in the other cases, clinicians rejected a diagnosis of bipolar disorder, instead assigning anxiety disorder diagnoses. Anxiety disorders represented a large category in which clinicians disagreed with the CIDI, particularly for panic disorder and agoraphobia. In most cases, clinicians determined that another disorder, such as social phobia, was the principal cause of the panic attacks, and they made fewer anxiety disorder diagnoses overall.
The CIDI only generates Axis I diagnoses, and in 15 of 52 cases (29%) a primary diagnosis of personality disorder (PD) was made by clinicians: that is, it was agreed by the clinical team that the patient’s presenting symptoms were primarily related to or a result of an underlying PD. Most often the CIDI generated an anxiety disorder diagnosis for patients with PD, and all four patients assigned a diagnosis of agoraphobia without panic were considered by clinicians to instead have a primary PD diagnosis. Post-traumatic stress disorder (PTSD) was also a common CIDI diagnosis in patients considered to have a primary PD. It is also possible that clinicians failed to diagnose a true comorbid anxiety disorder in patients with PD, for example, comorbid PTSD with borderline personality disorder.
The CIDI made fewer diagnoses of panic disorder and bipolar disorder in those with clinically diagnosed PD. The explanation for this is unclear, and further study is warranted.
Structured instruments such as the CIDI offer the possibility of standardizing routine clinical diagnosis and improving the detection rate for mental disorders (Zimmerman and Mattia, 1999). However, our examination shows that there may be significant disagreement with clinical diagnoses and suggests that clinical relevance and clinical judgments about key cognitive and motivational drivers that underlie symptoms are important considerations, consistent with research advocating that the gold standard of diagnosis may be the ‘LEAD’ standard: longitudinal, expert, all data (Spitzer, 1983).