
Abstract
Objective:
This paper examines public attitudes towards the acceptability of using prescription drugs to treat depression and attention deficit hyperactivity disorder (ADHD), and whether attitudes are influenced by familiarity with the use of pharmacological treatments for these disorders.
Method:
Participants were 1265 members of the general public aged 18–101 years (50% female) participating in the Queensland Social Survey (QSS), an omnibus state-wide survey of households in the state of Queensland. The survey was administered through a CATI (computer-assisted telephone interviewing) system.
Results:
Most members of the public thought that the drug treatment of depression was acceptable (55%) but attitudes were much less positive towards the use of drugs to treat ADHD (35.6% acceptable). Regression analyses showed that respondents who knew someone who had received pharmacological treatment for depression were more likely to find it acceptable. However, participants were divided about the acceptability of drug treatment for ADHD regardless of whether they knew someone who had received drug treatment for ADHD or not. Participants with a higher level of education were more likely to find drug treatment for depression and ADHD acceptable. Participants who did not know anyone who had received drug treatment were less likely to have a definite opinion on whether it was acceptable or unacceptable.
Conclusions:
Attitudes towards the acceptability of the use of prescription drugs are more positive for depression than for ADHD. This may broadly reflect ongoing controversies in the public sphere about the potential over-diagnosis of ADHD or overmedication of children with ADHD. Members of the public who do not know anyone with depression or ADHD may need particular information from prescribers in the event that they (or their child) are diagnosed.
Introduction
Attitudes towards the use of psychotropic medications for common mental disorders are an important aspect of ‘mental health literacy’ – that is, public knowledge and beliefs about mental disorders which aid their recognition, management or prevention (Jorm et al., 1997; Jorm, 2000). Attitudes towards commonly prescribed psychotropic medications (e.g. anti-depressants such as SSRIs; psychostimulants such as methylphenidate) may influence people’s willingness to start using these drugs, to continue using them, and to support their use by family and friends. These attitudes reflect broader cultural beliefs about the causes of mental illness and those who are affected by these disorders.
In Australia, the use of pharmacological treatments for mental disorders has increased over the last decade. In the 5 years to 2007, the use of prescription anti-depressants increased by 41% (Hollingworth et al., 2010). Between 2002 and 2009 the number of stimulants that were dispensed (typically to treat attention deficit hyperactivity disorder – ADHD) increased by 87% (Hollingworth et al., 2011). Public attitudes towards the use of psychotropic drugs have often been less positive than those of health care professionals, thereby posing a potential challenge to the use of these cost-effective and evidence-based treatments (Jorm et al., 2005). This paper explores the attitudes of members of the general public in Australia towards the acceptability of using prescription drugs to treat two common mental disorders, depression and ADHD, that are often treated with pharmaceutical drugs.
Surveys of the US public show an increase in the endorsement of medications for the treatment of several mental illnesses, but attitudes towards the use of prescription drugs are not uniform across disorders (Pescosolido et al., 2010). This is probably for a number of reasons, such as variations in the perceived risk/benefit profile of the drug; in the perceived effectiveness of non-pharmacological treatments; in beliefs about the aetiology of the disorder; and in the extent to which the condition is seen as a ‘brain disease’ rather than as the result of lifestyle, behavioural choices, and ‘character’ (Pescosolido et al., 2010). US surveys have not tended to explore attitudes towards the overall acceptability of using prescription drugs to treat depression and ADHD. Acceptability may be a good reflection of how members of the public weigh up the risks and benefits of pharmacological treatment and their views about the aetiology of the disorder.
In Australia, public views about the use of anti-depressants have become more positive since the 1990s, although some scepticism about their use is evident. A 1995 national survey of Australian adults found that only 29% thought medications would be helpful in treating depression but this increased in the two subsequent decades to almost 48% in 2003–2004 and to 59% in 2011 (Jorm et al., 2006; Reavley and Jorm, 2011). Despite these increases, more members of the public rated counselling, self-help, relaxation and close friends/family as helpful, and approximately 20% said anti-depressants were actually harmful (down from 42% in 1995 and 27% in 2003–2004) (Reavley and Jorm, 2011, 2012). A 2002 survey of 900 community members across Australia found that 65% thought anti-depressants were helpful in treating depression, but nonetheless only 2% said that pharmacological therapy would be their first choice of treatment (Highet et al., 2002).
There is comparatively little recent work on the attitudes of members of the Australian public towards the use of psychostimulants in the treatment of ADHD. Most surveys have focused on the attitudes of health professionals, school personnel and the parents of children with ADHD. A 2002 US survey of the general public found that two-thirds had heard of ADHD and, among them, 78% thought it was a genuine disorder (McLeod et al., 2007). However, as with depression, participants preferred non-pharmacological interventions over medication. An earlier study of over 1000 members of the US public found that less than a third would medicate a child with ADHD (McLeod et al., 2004). In a survey of over 600 Australian parents, 77% said they believed ADHD is a genuine disorder but around two-thirds also believed it was over-diagnosed and thought that too many children with ADHD were treated with medication (Gilmore, 2010).
The influence of familiarity on attitudes towards pharmacological treatment
A recent survey found that most Australian parents knew someone with ADHD either through colleagues or friends (40%), or in their own family (28%), but almost a third of parents had no contact with someone with ADHD (Gilmore, 2010). Those with some contact were more likely to think that too many children are medicated for ADHD. The influence of such contact on attitudes towards the use of medication is not always clear in studies in other countries. Some surveys have found that parents with a child with ADHD favour behavioural rather than pharmaceutical treatments (Corkum et al., 1999) but others have found that parents of children with ADHD rated stimulant treatment more positively than parents of non-ADHD children (Stroh et al., 2008).
Australian surveys have found that more people report personal familiarity with depression than ADHD, with most indicating that either they or a family member have experienced depression (Highet et al., 2002). Familiarity with depression may have a more positive effect on attitudes towards the use of medications since Jorm et al. (2005) found that those who viewed anti-depressants as harmful were less likely to know someone with the disorder. Similar results have been found in other countries (e.g. Dahlberg et al., 2008).
In this study we explored the general public’s attitudes towards the acceptability of using prescription drugs to treat depression and ADHD. This approach allowed us to take a broader perspective than would be possible by separately measuring attitudes towards specific aspects of prescription drug use such as ‘helpfulness’ or ‘harmfulness’, or ‘preferred first choice of therapy’. The first aim of this study was to explore whether the public viewed pharmacological treatments for depression and ADHD as acceptable, and to what extent attitudes were similar for the two disorders. We also asked about participants’ familiarity with people who have been treated for these two conditions using prescription drugs (e.g. have you or anyone you know personally been treated for depression/ADHD with prescription drugs?). The second aim was to explore how ‘familiarity’ was related to attitudes on the acceptability of pharmacological treatment for depression and ADHD.
Method
Sample
The sample comprised 1265 participants: 633 males and 632 females (aged 18+ years; range 18–101; mean = 53.7). Younger people were under-sampled when compared with the Australian Bureau of Statistics (ABS) census data for the Queensland population. Those aged under 35 years comprised 13.9% of the sample (vs 30.6% ABS), those aged 35–54 years comprised 35.1% (vs 38% ABS), and those aged 55+ years comprised 50.3% (vs 31.4% ABS). The sample varied in the number of years of education: 1–10 (24.3%), 11–12 (22.5%), 13–14 (10.9%), and 15+ (41.2%).
The survey instrument: The Queensland Social Survey
Data collection was during July and August 2011 through the Queensland Social Survey (QSS), which is an omnibus style state-wide survey of households in the state of Queensland, Australia. The QSS is administered through a CATI (computer-assisted telephone interviewing) system at Central Queensland University. It includes questions from multiple research bodies and other organizations on a wide range of topics. Among the questions participants were asked, we included two on the extent to which they agreed with the following statements:
Q1. It is acceptable for prescription drugs, such as Prozac, to be used in the treatment of depression. Q2. It is acceptable for prescription drugs, such as Ritalin, to be used in the treatment of ADHD (attention deficit hyperactivity disorder).
Participants were asked to respond using the following response categories: (1) strongly agree; (2) agree; (3) slightly agree; (4) neither agree nor disagree; (5) slightly disagree; (6) disagree; (7) strongly disagree; (8) don’t know. In Australia, Prozac and Ritalin are widely prescribed for the treatment of depression and ADHD, respectively, and are commonly mentioned in the media discourse about these conditions; we mentioned them by name to aid participant understanding.
Next, we asked participants about their familiarity with persons who have been treated for depression or ADHD with prescription drugs:
Q3. Have you, or someone you know personally, ever been treated for depression with prescription drugs? Q4. Have you, or someone you know personally, ever been treated for ADHD with prescription drugs?
Participants were asked to answer according to the following format: (1) yes – I have; (2) yes – someone I know personally has; (3) yes – both myself and someone I know personally; (4) no; (5) don’t know.
Procedure
The target population for the telephone interview consisted of persons 18 years of age or older who, at the time of the survey, were living in a dwelling unit in Queensland and could be contacted by direct-dialled, land-based telephone service. The response rate was 31.9%. The sample was drawn from a telephone database by using a computer program to select a random sample of phone numbers. Within the household, one eligible person was selected as the respondent for the interview. The respondent within each household was selected on the basis of gender using the following selection guidelines to ensure an equal yet random selection of male and female participants:
The dwelling unit must be the person’s usual place of residence and he/she must be 18 years of age or older;
Each household was randomly pre-selected as either a male or female household;
If there was more than one male/female in the household then the male/female that had the most recent birthday was selected;
If there was no-one of the pre-selected gender residing in the house then the house was designated not qualified.
Analysis
Participant responses to Q1 and Q2 were coded into four categories (Agree; Disagree; Neutral; Don’t know). Responses to Q3 and Q4 were coded into three groups (Not familiar; Yes – other (i.e. I personally know someone who has been treated with prescription drugs for that disorder); Yes – me (i.e. I have been treated with prescription drugs for that disorder)). Descriptive analyses gave overall rates of agreement with the acceptability of using prescription drugs to treat depression and ADHD, and overall rates of familiarity with drug treatment for depression and ADHD.
We conducted two logistic regression analyses (one for depression and one for ADHD) to predict agreement with the acceptability of using prescription drugs to treat the disorder. In these models, participants who responded ‘Don’t know’ or ‘Neutral’ were excluded. The dependent variable was ‘Agreement with the acceptability of using prescription drugs’ coded as disagree = 0; agree = 1. The predictor variables were: familiarity with the relevant disorder (not familiar = 0 (ref); yes – other = 1; yes – me = 2); gender (male = 0 (ref); female = 1); years of education (1–10 years = 0 (ref); 11–12 years = 1; 13–14 years = 2; 15 years+ = 3); and age (entered as a continuous variable).
Using the same method, we conducted two logistic regression analyses (one for depression and one for ADHD) to predict actually having an opinion about the acceptability of using prescription drugs to treat the relevant disorder, as opposed to answering ‘Don’t know’ / ‘Neutral’. In these models, participants answering ‘Neutral’ and ‘Don’t know’ were combined, and compared to participants who agreed or disagreed (i.e. they expressed a firm opinion pro or con). The dependent variable was ‘Having an opinion’, coded as no opinion = 0; opinion = 1. The predictor variables were the same as above.
Results
A majority of participants said that it was acceptable to use prescription drugs to treat depression (55.5%); only 15.1% expressed outright disagreement. By contrast, attitudes towards the use of prescription drugs to treat ADHD were much less positive, with about the same proportion saying it was acceptable (35.6%) as unacceptable (35.7%) (Figure 1). For both depression and ADHD, almost one in five participants answered ‘Don’t know’ (19.8% for depression and 19.5% for ADHD) and a smaller proportion indicated that their opinion was neutral (i.e. that they neither agreed nor disagreed).
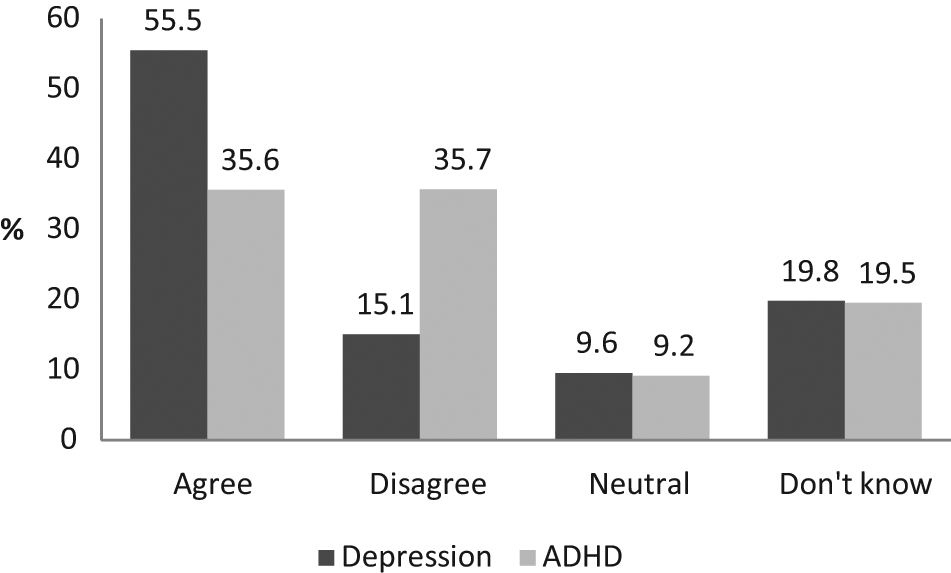
Responses to the statement ‘It is acceptable for prescription drugs to be used in the treatment of depression and ADHD’.
There were some interesting patterns of association between positive and negative attitudes towards using drugs to treat the two disorders. The great majority (80%) of those who thought drug treatment was acceptable for ADHD also thought that drug treatment was acceptable for depression and 70.1% of participants who disagreed with drug treatment for depression also disagreed with treating ADHD with drugs. But support for drug treatment of depression did not necessarily translate into support for drug treatment of ADHD. Indeed, only 51.1% of those who agreed with drug treatment for depression thought that drug treatment for ADHD was acceptable.
Depression
Familiarity
Almost two-thirds of all participants were familiar with someone treated for depression (65.4%) in that they had either been treated for depression with prescription drugs (20.2%) or personally knew someone who had (45.2%). The remainder (34.5 %) did not know anyone who had been treated for depression with prescription drugs (26.1% of all female participants, and 46% of all males).
Table 1 shows that participants in the ‘Not familiar’ group (39.1%) had a lower rate of agreement with the use of prescription drugs to treat depression, compared to those who knew someone who had been treated (62.4%), or those who had been treated themselves (68%). More participants in the ‘Not familiar’ group also answered ‘Don’t know’ (31.8%) compared to participants who either knew someone who had been treated with drugs for depression or who had been treated themselves.
Agreement with the statement ‘It is acceptable for prescription drugs to be used in the treatment of depression’ according to familiarity with treatment for depression with prescription drugs.
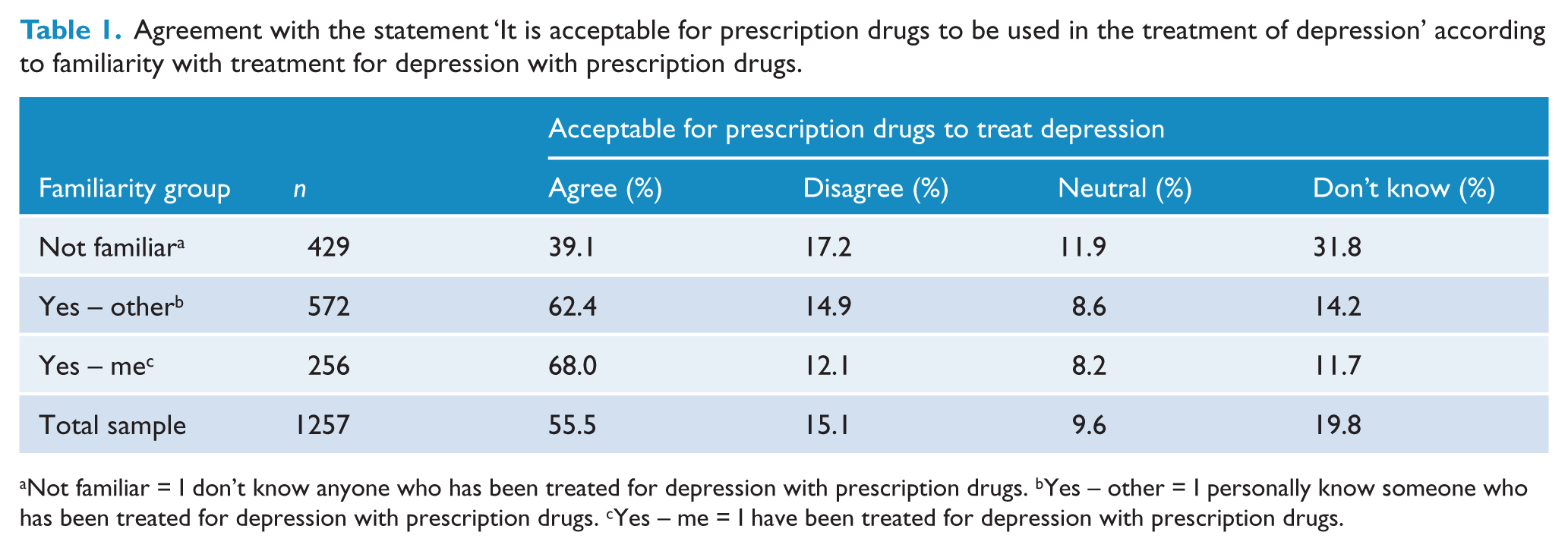
Not familiar = I don’t know anyone who has been treated for depression with prescription drugs. bYes – other = I personally know someone who has been treated for depression with prescription drugs. cYes – me = I have been treated for depression with prescription drugs.
Predicting positive attitudes towards the acceptability of drug treatment for depression
A logistic regression analysis was used to assess the impact of a number of factors on the likelihood that participants would agree with the acceptability of using prescription drugs to treat depression. The full model was able to distinguish between respondents who expressed outright agreement, and those who expressed outright disagreement, with the use of drugs to treat depression (χ2 (7, n = 886) = 40.185, p < 0.001). Table 2a shows that familiarity and education were significant predictors while age and gender were not. Compared to those with no familiarity, participants who had been treated for depression with prescription drugs were 2.6 times more likely to agree that drug treatment for depression was acceptable. Those who personally knew someone who had been treated with drugs for depression were 1.7 times more likely to agree with drug treatment than those with no familiarity. A higher level of education also predicted agreement with the acceptability of drug treatment for depression. Compared to those with 1–10 years of education, participants with 15 or more years of education were 2.2 times more likely to agree that drug treatment for depression is acceptable (participants with 11–12 years of education were 1.75 times more likely to agree, and participants with 13–14 years of education were 1.9 times more likely to agree). Age and gender were not significant predictors of attitudes.
‘It is acceptable for prescription drugs to be used in the treatment of depression’: (a) predictors of agreement with the statement; (b) predictors of having an opinion (vs ‘Don’t know’ / ‘Neutral’).
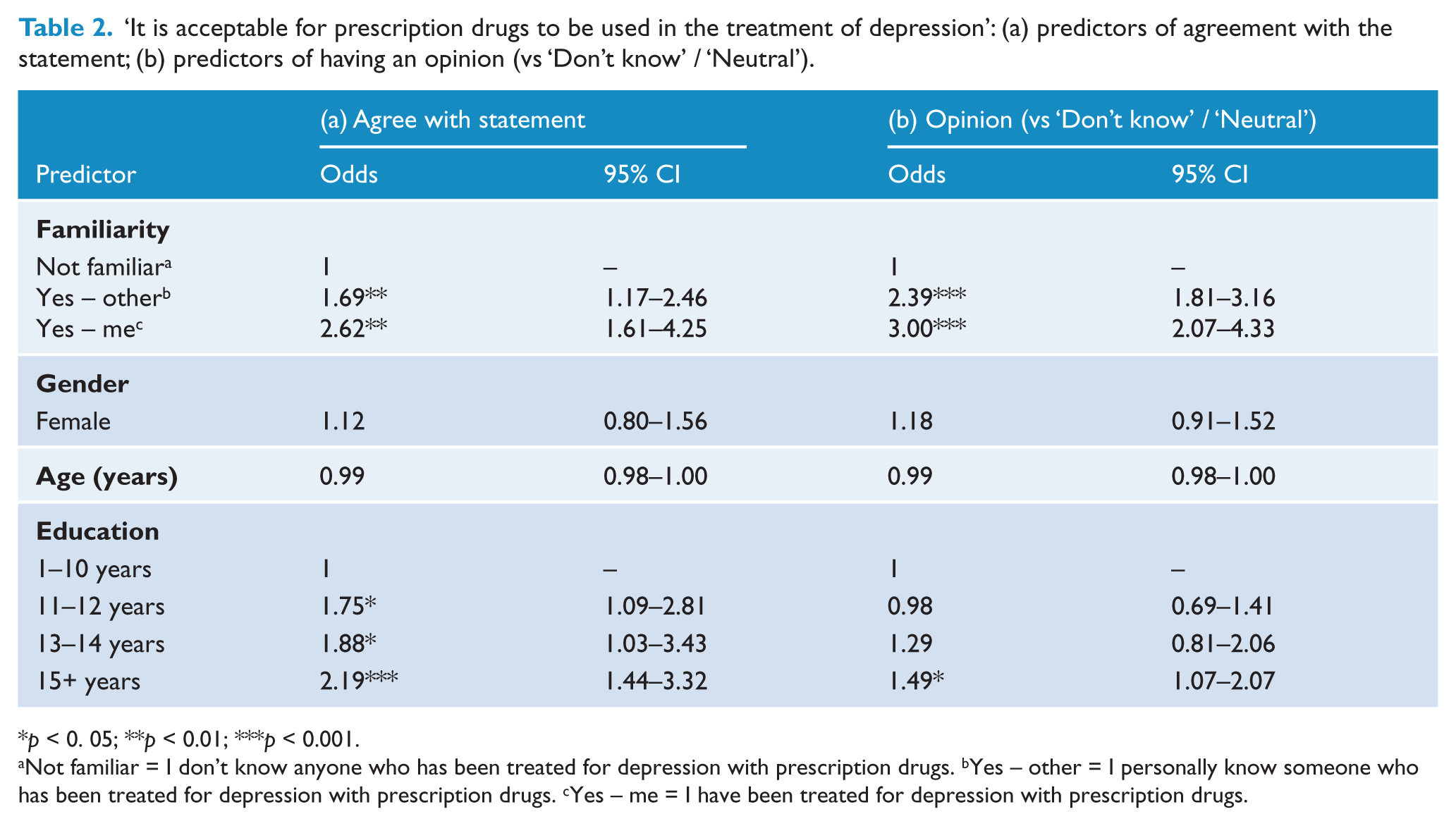
p < 0. 05; **p < 0.01; ***p < 0.001.
Not familiar = I don’t know anyone who has been treated for depression with prescription drugs. bYes – other = I personally know someone who has been treated for depression with prescription drugs. cYes – me = I have been treated for depression with prescription drugs.
Predicting positive or negative opinion versus no opinion towards the acceptability of using drugs to treat depression
Since a substantial minority of participants offered no opinion (i.e. they answered ‘Don’t know’ or ‘Neutral’) on the acceptability of using prescription drugs to treat depression, we used a logistic regression analysis to identify the characteristics of participants that predicted whether they would offer an opinion on the issue. The full model was statistically significant (χ2 (7, n = 1251) = 83.38, p < 0.001). Table 2b shows that familiarity was a significant predictor – participants who had been treated for depression with prescription drugs were three times more likely to express a firm opinion about the acceptability of drug treatment and those who personally knew someone who had been treated were 2.4 times more likely. Participants with 15 or more years of education were also significantly more likely to express an opinion than answer ‘Don’t know’ or remain neutral, than participants with 1–10 years of education. Age and gender were not significant predictors.
ADHD
Familiarity
In contrast with depression, most (68.9%) participants did not know anyone who had been treated for ADHD using prescription drugs (‘Not familiar’); 28.7% knew someone who had been treated; only 2.5% had been treated themselves. Table 3 shows that, as with depression, a much higher proportion of people in the ‘Not familiar’ group answered ‘Don’t know’ (25.1%) compared to the two ‘Familiar’ groups. Those in the ‘Not familiar’ group had the lowest rate of agreement with the acceptability of drug treatment for ADHD, although the ratio of agree-to-disagree responses was similar to those who personally knew someone who has undergone drug treatment for ADHD.
Agreement with the statement ‘It is acceptable for prescription drugs to be used in the treatment of ADHD’ according to familiarity with treatment for ADHD with prescription drugs.
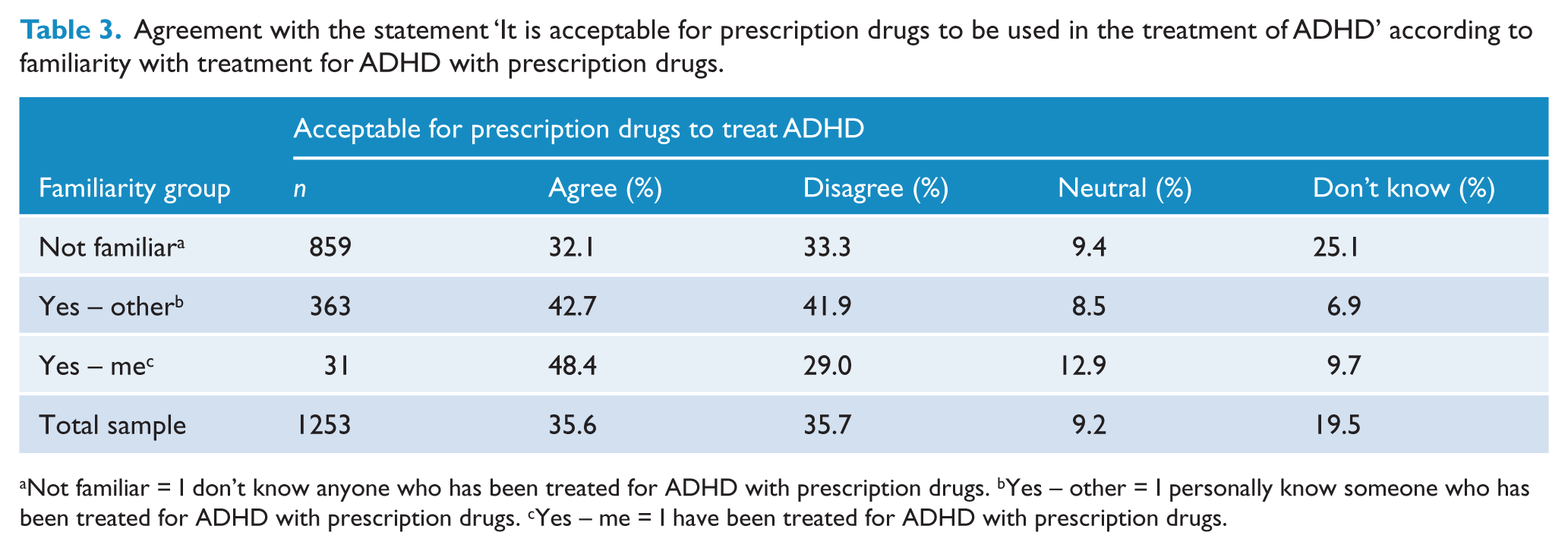
Not familiar = I don’t know anyone who has been treated for ADHD with prescription drugs. bYes – other = I personally know someone who has been treated for ADHD with prescription drugs. cYes – me = I have been treated for ADHD with prescription drugs.
Predicting positive attitudes towards the acceptability of drug treatment for ADHD
For ADHD, the full regression model was also statistically significant and able to distinguish between respondents who expressed outright agreement, and those who disagreed, with the use of drugs to treat ADHD (χ2 (7, n = 896) = 17.201, p < 0.05). Table 4a shows that only education was a significant predictor; familiarity, age and gender were not. Participants with 11–12, 13–14 and 15+ years of education were all more likely to agree that drug treatment for ADHD is acceptable than those with 1–10 years of education.
‘It is acceptable for prescription drugs to be used in the treatment of ADHD’: (a) predictors of agreement with the statement; (b) predictors of having an opinion (vs ‘Don’t know’ / ‘Neutral’).
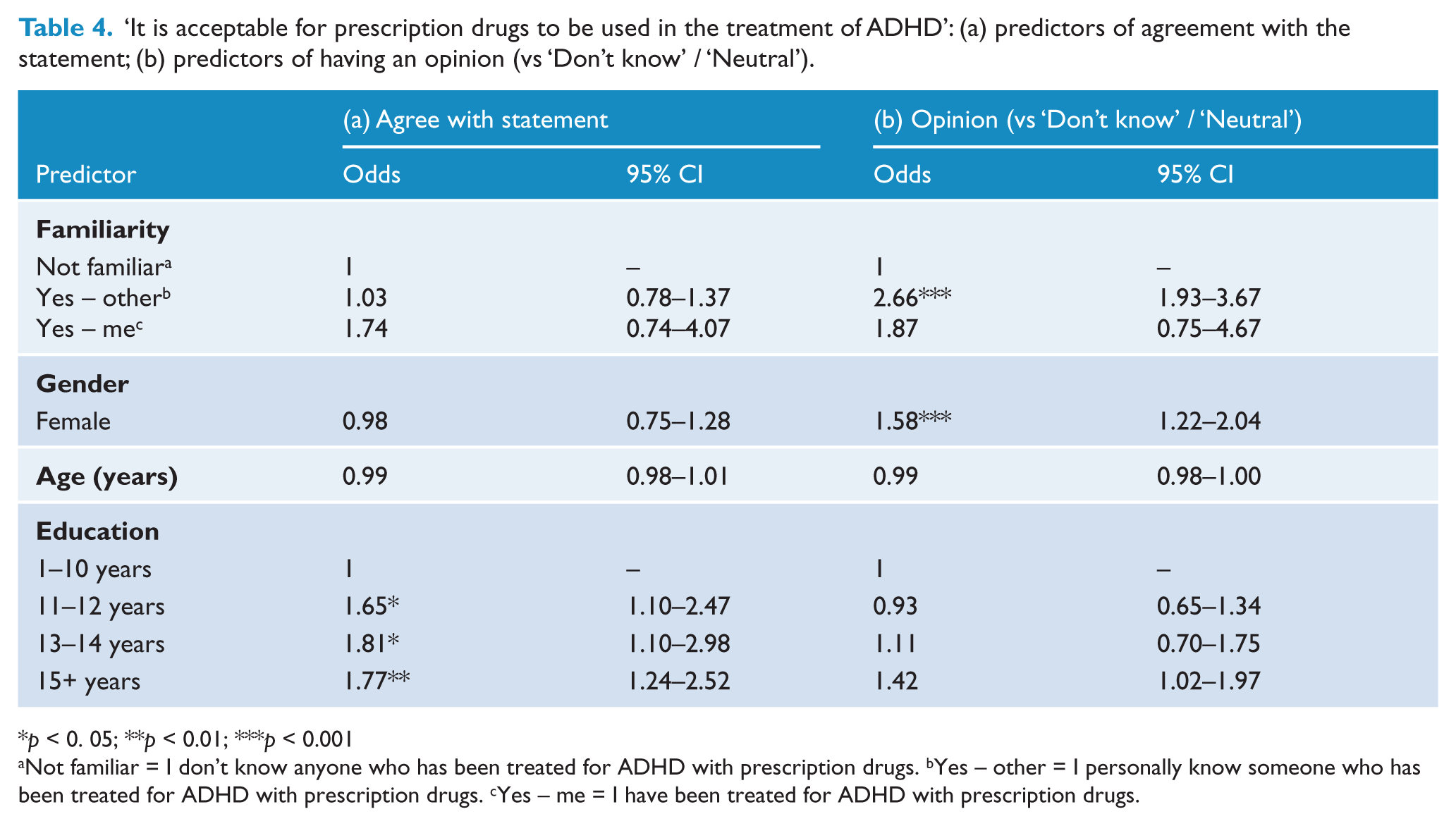
p < 0. 05; **p < 0.01; ***p < 0.001
Not familiar = I don’t know anyone who has been treated for ADHD with prescription drugs. bYes – other = I personally know someone who has been treated for ADHD with prescription drugs. cYes – me = I have been treated for ADHD with prescription drugs.
Predicting positive or negative opinion versus no opinion towards the acceptability of drug treatment for ADHD
The full regression model was statistically significant (χ2 (7, n = 1251) = 72.518, p < 0.001) and, as with depression, Table 4b shows that gender was the only significant predictor – women were 1.5 times more likely to have an opinion than men. Age and education were not significant predictors of having an opinion about the acceptability of drug treatment for ADHD. Familiarity was a statistically significant predictor in this model. Those who personally knew someone who had undergone drug treatment for ADHD were 2.6 times more likely to have an opinion about the acceptability of drug treatment for ADHD compared to those in the ‘Not familiar’ group. Participants who had undergone drug treatment for ADHD were not significantly more likely to have an opinion about its acceptability compared to those in the ‘Not familiar’ group.
Discussion
Our survey found that most members of the public viewed drug treatment for depression as acceptable, while only a minority did not. Previous surveys of public attitudes have found that support for the use of anti-depressants has increased over time (Reavley and Jorm, 2011), and that people who view anti-depressants as harmful were less likely to know someone with the disorder (Jorm et al., 2005; Reavley and Jorm, 2012). In our survey, participants who had either been treated for depression with prescription drugs or knew someone who had, were more likely to think drug treatment for depression is acceptable. People who were not familiar were also, perhaps appropriately, much more likely to reserve judgement and indicate that they did not know whether it is acceptable or not.
Public attitudes were much less positive towards the use of drugs to treat ADHD – the proportion of participants in favour was almost equal to that who found it unacceptable. This may broadly reflect ongoing controversies in the public sphere about the potential over-diagnosis or overmedication of children with ADHD. Surveys with parents and educators have sometimes shown conflicting attitudes towards the use of stimulants in the treatment of ADHD. While some surveys indicate that parents of children with ADHD are more likely to favour behavioural treatment, other studies have found that they view stimulants more positively (Corkum et al., 1999; McLeod et al., 2007; Stroh et al., 2008). This has made it difficult to ascertain whether objections to drug treatment for ADHD stem from those with personal experience with such treatments, or from those who are relatively unfamiliar with the disorder. Our results indicate that members of the general public are divided about the acceptability of drug treatment for ADHD, regardless of whether they have had personal contact with someone with ADHD or not. As with depression, we found that a large proportion of people with no personal contact with ADHD said that they did not know whether it was acceptable. Women were more likely than men to have a firm opinion about the acceptability of drug treatment, but were just as divided in their opinion as men.
There are several strengths and limitations of this study. The sample size is large enough to make useful comparisons across relevant attitudinal and demographic categories, and the sample comprised a reasonably broad cross-section of the community. The ‘acceptability’ measure adds a useful contribution to the literature about public attitudes towards prescription drug treatment beyond measures of helpfulness or harmfulness. Furthermore, the survey compared public attitudes between two disorders and assessed personal familiarity, supporting previous evidence on the importance of personal experience in forming attitudes towards drug treatment of mental health problems. However, the representativeness of the sample was limited by the over-sampling of older participants from Queensland only, and the relatively low participation rate (31.9%). Gaining adequate participation from younger respondents when conducting CATI surveys using only randomly generated landline telephone samples has become more difficult as increasing numbers of young people use only mobile (cell) telephones, although US mobile/cell samples have been found to have a lower response rate (Hu et al., 2011). Some studies have shown that the exclusion of mobile phone-only households does not significantly influence survey results (Pennay and Bishop, 2009). However, other studies have found that ‘landline’ and ‘mobile/cell’ samples differ in ways that may affect survey results (e.g. age; prevalence of health-related behaviours such as alcohol consumption or smoking) (Hu et al., 2011; Newman, 2011).
Our survey results may be useful for practitioners and policy makers. At a broad level, it is important to understand how public attitudes towards pharmacological treatments for mental disorders align with those of prescribers. Negative attitudes towards drug treatment of ADHD may reduce a patient’s willingness to undergo or maintain drug treatment. Attitudes towards drug treatment are unlikely to be consistent across disorders. They are likely influenced by participants’ previous anecdotal experiences with drug treatment, including whether or not they know anyone who has undergone such treatment, as much as by media coverage.
In our survey, the high proportion of ‘Don’t know’ responses among people without any personal contact with depression or ADHD may indicate that people’s attitudes towards the acceptability of drug treatment of these disorders are largely guided by personal or vicarious experiences. For ADHD and depression, people who answered ‘Don’t know’ were less likely to know someone who had undergone drug treatment for the condition (and less likely to have received drug treatment themselves). It may be that many people who indicated ‘Don’t know’ felt that it was precisely because they lacked any personal contact with someone with ADHD or depression, that they were unable to make an informed judgement about whether drug treatment of those conditions was acceptable. Depression and ADHD are among the most common mental conditions in Australia, but members of the public who do not know anyone with the disorder may need particular information in the event that they (or their child) are diagnosed. Asking recently diagnosed patients whether they personally know anyone with the disorder (or know anyone who has undergone drug treatment for the disorder) may be a quick way for doctors to raise the questions of prior knowledge of and attitudes towards drug treatment.
Our results suggest the need for in-depth qualitative studies of public attitudes to better understand the reasons for beliefs about the acceptability of drug treatment for depression and ADHD. This would help to elucidate the commonly held beliefs underlying attitudes towards drug treatment and the factors that shape attitudes, particularly the influence of familiarity and anecdotal experiences with both disorders. For both depression and ADHD this would be useful in exploring the reasons people had for expressing outright disagreement with drug treatment. Our results indicate that the use of prescription anti-depressants is acceptable to most; however, we did not ask participants how different forms of treatment compared in terms of their acceptability. A number of studies have found that behavioural treatments or self-help for depression are often preferred to medication (Jorm et al., 2006; Reavley and Jorm, 2011), although one recent study found that people who viewed anti-depressants as harmful were also likely to have less positive views about other forms of treatment (Reavley and Jorm, 2012). Less is known about attitudes towards the preferred methods of treatment for ADHD. Qualitative studies could build on this knowledge by exploring why drug treatment may be viewed as unacceptable or not the preferred method of treatment.
Footnotes
Funding
This work was supported by an NHMRC Australia Fellowship awarded to WH, and an NHMRC Training Fellowship awarded to BP.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.