
Abstract
Objective:
To analyse, and explain to Australasian psychiatrists, recent proposed changes to the terms of coercive treatment for mental illness in Tasmania and Victoria and to place the proposals in the context of a broader human rights framework that is likely to impact the future shape of mental health legislation more generally.
Methods:
The Australian law reform proposals are reviewed against the requirements of numerous human rights instruments, including the recently ratified United Nations Convention on the Rights of Persons with Disabilities. Ethical and legal arguments are made to support the proposed changes and to introduce others, taking into account academic commentary on mental health law and recent empirical work on the ability to usefully categorise patients by their likelihood of harm to self and others.
Results:
The Victorian and Tasmanian draft mental health bills propose a new basis for compulsory psychiatric treatment in Australasia. If they become law, coercive psychiatric treatment could only be applied to patients who lack decision-making capacity. The Tasmanian draft bill also sets a new benchmark for timely independent review of compulsory treatment. However both jurisdictions propose to retain an ‘additional harm’ test which must be satisfied before patients may be treated without consent. This differs from non-psychiatric cases, where if patients are unable to consent to medical treatment for themselves, they will be entitled to receive coercive treatment if it is in their best interests.
Conclusions:
The proposed changes under the Tasmanian and Victorian draft mental health bills will ensure that, in line with local and international human rights obligations, only patients who lack decision-making capacity may be coercively treated for mental illness. However the continuing ‘additional harm’ criteria may breach human rights obligations by imposing a discriminatory threshold for care on patients who are unable to consent to treatment for themselves. This could be avoided by replacing the ‘additional harm’ test with a ‘best interests’ test.
Introduction
Australian mental health law is on the verge of a major change. Western Australia, Tasmania, Victoria and the Australian Capital Territory are currently reviewing their Mental Health Acts, and in the last year, both the Victorian and Tasmanian governments have released draft Mental Health Bills for public comment (Mental Health Bill 2010 (Vic) (Exposure Draft); Mental Health Bill 2011 (Tas) (Exposure Draft)). These draft bills represent the first attempts at refashioning mental health laws under the influence of the recently ratified United Nations Convention on the Rights of Persons with Disabilities (CRPD) (United Nations, 2006). In Victoria and the Australian Capital Territory, the legislative reforms have also been moulded by local human rights legislation (Charter of Human Rights and Responsibilities Act 2006 (Vic); Human Rights Act 2004 (ACT)).
The Victorian and Tasmanian draft bills contain some important human rights based innovations. Current mental health legislation in every state and territory, and in New Zealand, allows coercive treatment of any person with a mental illness whom doctors think is likely to come to some harm themselves, or to harm others. These proposed laws, though, will only permit treatment without consent where patients lack capacity to make their own treatment decisions ((Mental Health Bill 2010 (Vic) (Exposure Draft) cls. 64, 70; Mental Health Bill 2011 (Tas) (Exposure Draft) cls. 42, 59). In addition, Tasmania has proposed a reduction in the current wait time for tribunal review of involuntary orders from 28 days to 4 days (Mental Health Bill 2011 (Tas) (Exposure Draft) cl. 51). Both these initiatives represent a significant improvement in rights protection for patients.
While these proposals have attracted a deal of attention among legal scholars, issues such as the introduction of capacity-based admission criteria, problems with ‘additional harm’ requirements, and reducing wait times for independent review of detention, will not be familiar to many psychiatrists. It is important, however, that psychiatrists be engaged in the process as the changes will profoundly affect both clinical practice and the administration of coercive treatment for mental illness. In the context of ANZJP’s longstanding and key role as a platform for discussion of mental health legislative reform (Doutney, 1986; Ellard, 1990; Gray et al., 2010; Kirby, 1983; McKenna et al., 2000; McLachlan and Mulder, 1999; O’Brien et al., 1995; Rosenman, 1994), this paper seeks to explain these reforms in the context of an increasingly focused and influential international movement towards greater protection of the civil rights of people with disabilities.
Tides of change
In recent years, there has been a significant shift in the legal and intellectual landscape in which Australia and New Zealand’s mental health laws are situated. In July 2008, the Australian government ratified the United Nations Convention on the Rights of Persons with Disabilities (CRPD) (United Nations, 2006). New Zealand ratified the Convention in September of the same year. The CPRD built on the set of conventions known as the International Bill of Human Rights – which includes the Universal Declaration of Human Rights (1948) (UDHR) and the International Covenant on Civil and Political Rights (1966) (ICCPR) – by introducing a set of measures specifically designed to bolster the rights of persons with disabilities, including people living with mental illness. The CPRD supersedes earlier non-binding guidelines set out in the United Nations Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care (United Nations, 1991).
In addition, Victoria, the Australian Capital Territory and New Zealand have enacted local human rights legislation (or charters) giving legal protection to the human rights set out in those documents (Charter of Human Rights and Responsibilities Act 2006 (Vic); Human Rights Act 2004 (ACT); New Zealand Bill of Rights Act 1990 (NZ)). The charters require local legislation to be interpreted in a way that is compatible with the prescribed rights (Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 32; Human Rights Act 2004 (ACT) s. 30; New Zealand Bill of Rights Act 1990 (NZ) s. 6), and that government policies comply with these human rights obligations (Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 38; Human Rights Act 2004 (ACT) s. 40B).
Critically for mental health law reform, the rights protected under international and local laws include the right to freedom from discrimination and equality before the law (United Nations, 1948: art. 7; United Nations, 1966: art. 26; United Nations, 2006: arts. 5, 12; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 8; New Zealand Bill of Rights Act 1990 (NZ) s. 19); protection from cruel, inhuman or degrading treatment (United Nations, 1948: art. 5; United Nations, 1966: art. 7; United Nations, 2006: art. 15; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 10; Human Rights Act 2004 (ACT) s. 10; New Zealand Bill of Rights Act 1990 (NZ) s. 19); freedom of movement (United Nations, 1948: art. 13; United Nations, 1966: arts. 9–12; United Nations, 2006: art. 14; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 12; New Zealand Bill of Rights Act 1990 (NZ) s. 18); freedom from arbitrary detention (United Nations, 1948: art. 9; United Nations, 1966: art. 9; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 21; New Zealand Bill of Rights Act 1990 (NZ) s. 22); humane treatment when deprived of liberty (United Nations, 1966: art. 10; United Nations, 2006: art. 14; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 22; New Zealand Bill of Rights Act 1990 (NZ) s. 23(5)); and a fair hearing by an impartial tribunal to decide rights recognised by law (United Nations, 1948: art. 10; United Nations, 1991: principle 17; Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 2; New Zealand Bill of Rights Act 1990 (NZ) s. 23(3)). The Victorian and Australian Capital Territory human rights charters also specifically provide that a person must not be subject to medical treatment without consent (Charter of Human Rights and Responsibilities Act 2006 (Vic) s. 10; Human Rights Act 2004 (ACT) s. 10), while the New Zealand Bill of Rights declares that ‘[e]veryone has the right to refuse to undergo any medical treatment’ (New Zealand Bill of Rights Act 1990 (NZ) s. 11).
In addition to these more general rights, the CRPD specifies that persons with disabilities are entitled to recognition of legal capacity on an equal basis with others, and access to support in exercising their legal capacity (United Nations, 2006: art. 12). The CRPD also calls for the modification and abolition of existing laws and practices that constitute discrimination against persons with disabilities (United Nations, 2006: art. 4(1)(b)).
International law requires that signatory states must conform to treaty requirements when making new laws and Australian courts have determined that existing local laws will be interpreted in a manner that is consistent with treaty obligations where there is any ambiguity as to their meaning (Minister of State for Immigration & Ethnic Affairs v Teoh [1995] HCA 20 at [26]; Cranwell, 2001). As the CRPD requires states to adopt strategies to ensure the full realisation of all human rights for people with disabilities, including people with mental illness, it is expected to have, and seems already to be having, a significant impact on the development of mental health laws in Australia.
In addition to these developments in human rights protection, there has been a burgeoning academic critique of legislative schemes in which the power to provide coercive psychiatric treatment is based on an assessment of the patient’s perceived risk of future harm (Langan, 2010; Large et al., 2008b, 2011a, 2011b, 2011d; Mossman, 2006, 2009; Ryan, 2009; Ryan et al., 2010a; Szmukler, 2003). The ‘future harm’ to be assessed is of two overlapping types. The first is the likelihood of patients coming to harm themselves either through active self-harm or through mental or physical deterioration. Judgements like these are required in Queensland, both Australian territories and (arguably) in Tasmania. The other type is the likelihood of the patient causing harm to others. Risk of harm to others is a criterion for involuntary treatment in all Australasian jurisdictions. However an increasing body of research has shown that in practice, it is impossible to usefully categorise patients into those who are at high or low risk of future harm (Large and Nielssen, 2011; Large et al., 2011b, 2011c, 2011d; Mossman, 2009; Singh et al., 2011;). Furthermore, in focusing on illusive factors such as ‘risk of harm’ rather than the severity of a person’s illness and the person’s ability to make treatment decisions for themselves, such schemes will arguably lead to denial of treatment for patients in genuine need and to forced detention and treatment of patients whose refusals should perhaps have been respected (Ryan, 2011b).
These arguments lend support to a radical reform approach in which decisions about coercive treatment require, first and foremost, a determination of whether or not a person with mental illness has capacity to make treatment decisions for themselves. A mentally ill person with capacity should then be permitted to refuse treatment in the same way as any other patient. Mentally ill people who do not have capacity could be treated according to a legislated best interests test without any other consideration of possible future harms (or indeed even current harms) aside from those that would form part of the calculations of that best interests test (Bartlett, 2003; Buchanan, 2002; Dawson and Szmukler, 2006; Richardson, 2002; Ryan, 2011a).
Against this background, the Victorian, Western Australian, Australian Capital Territory and Tasmanian governments have each established major reviews of their mental health legislation. New South Wales is set to begin such a review later this year. In Victoria and Tasmania, where the review process is most advanced, the preparatory phase has concluded and each state has released an Exposure Draft Mental Health Bill for public comment (Mental Health Bill 2010 (Vic) (Exposure Draft); Mental Health Bill 2011 (Tas) (Exposure Draft)). The Victorian draft bill was released in late 2010 and submissions received from the public are now being considered by the Victorian Department of Health. A final bill is expected to be released shortly, for introduction to parliament (State Government of Victoria, 2011). The Tasmanian draft bill was released in June 2011 and at the time of writing, submissions were still being received.
The following sections explore the proposals of the Victorian and Tasmanian draft legislation in relation to the criteria for coercive treatment. In particular, we examine the definition of patient capacity and its role in making compulsory orders, as well as the requirement that patients suffer harm additional to their mental illness before accessing treatment and the mechanisms for review of compulsory treatment orders.
Human rights and compulsory orders in the draft bills
Coercive treatment and capacity to consent
The right to self-determination is well recognised both under international law (United Nations, 1966: art. 1) and in the common law principle that a person is entitled to make autonomous decisions about medical treatment, provided they have the capacity to do so (Hunter and New England Area Health Service v A [2009] NSWSC 761 (‘Hunter’)). This right has been reinforced for people with mental illness by the provisions of the CPRD, which require that persons with disabilities must be able to exercise legal capacity on an equal basis with others (United Nations, 2006: art. 12.2).
A person will have the capacity to refuse medical treatment at common law if they are able to comprehend and retain information which is material to the decision (in particular, information about the consequences of the decision) and to use and weigh the information as part of the process of making the decision (Hunter [2009] NSWSC 761 at [25]). A competent person may refuse medical treatment even if that decision is ‘not sensible, rational or well considered’ (Hunter [2009] NSWSC 761 at [10]; Re T (Adult: Refusal of Treatment) [1992] EWCA Civ 18 (‘Re T’) at [39]) and even if refusal will likely lead to death or serious injury (Hunter [2009] NSWSC 761 at [11]; Re T [1992] EWCA Civ 18 at [54]). Equally, where a person is found to lack capacity it is generally accepted both ethically (Beauchamp and Childress, 2009) and legally (Hunter [2009] NSWSC 761 at [31–34]; Re T [1992] EWCA Civ 18 at [5]) that his or her refusal of treatment may be overridden as it will not be taken to reflect a genuine free choice. At common law, a person who lacks capacity may be treated by doctors in an emergency situation if to do so would be in the person’s best interests, notwithstanding any stated refusal of medical treatment (Hunter [2009] NSWSC 761 at [31–34]). Guardianship laws in all Australasian jurisdictions provide for consent to be given by a substitute decision maker where patients lack decision-making capacity (Guardianship Act 1987 (NSW); Guardianship and Administration Act 2000 (Qld); Guardianship and Administration Act 1993 (SA); Guardianship and Administration Act 1995 (Tas); Guardianship and Administration Act 1986 (Vic); Guardianship and Administration Act 1990 (WA); Guardianship and Management of Property Act 1991 (ACT); Adult Guardianship Act 1998 (NT); Protection of Personal and Property Rights Act 1988 (NZ)).
For patients with mental illness, however, the presence or absence of decision-making capacity has not been determinative of whether or not that person can be treated without consent. In Victoria, Queensland, the Northern Territory and Western Australia, a patient may be coercively treated if they lack capacity to consent to treatment themselves or if they have refused treatment (in Queensland and the Northern Territory the patient must have refused treatment unreasonably) (Mental Health Act 1986 (Vic) s. 8(1); Mental Health Act 2000 (Qld) s. 14(1)(f); Mental Health and Related Services Act 1998 (NT) s. 14; Mental Health Act 1996 (WA) s. 26). In New South Wales, South Australia, Tasmania and the Australian Capital Territory, and also in New Zealand, decision-making capacity is not a consideration at all.
Generally speaking, in all Australasian jurisdictions patients can be treated without consent if they have a mental illness (whether or not they lack capacity) and they are thought to be at risk of some type of harm to themselves or others. This has had the dual impact of denying some competent patients with mental illness a right to control their own treatment decisions, while at the same time denying persons who lack decision-making capacity access to treatment in their best interests, in circumstances where they do not meet the extra requirements of the relevant likelihood of harm or ‘additional harm’ test. This situation is arguably discriminatory and contrary to human rights obligations that demand that all persons are entitled to equal protection under the law.
New capacity criteria in Victoria and Tasmania
Both the Victorian and Tasmanian draft Bills have sought to address this issue by introducing a significant change to the rationale for coercive treatment, requiring that a person can only be treated non-consensually if they lack decision-making capacity to refuse treatment (Mental Health Bill 2010 (Vic) (Exposure Draft) cls. 64(d), 70(c), 71(c); Mental Health Bill 2011 (Tas) (Exposure Draft) cls. 42, 59(e)). This represents a seismic shift in previous approaches to involuntary treatment and comes even as the Tasmanian government recommended in 2007 that ‘when a person has a treatable mental illness and as a result of that mental illness the person is a danger to themselves or others, the State has a duty to intervene and provide treatment to that person, even though they may have made a competent and informed choice not to consent to treatment’ (Tasmanian Department of Health Human Services, 2007: p. 16 (emphasis added)). This change in position seems to reflect the gathering influence of the human rights movement in mental health as well as the influence of the CRPD.
Under the Tasmanian Mental Health Bill (Exposure Draft), a person lacks the requisite ‘mental capacity’ to make a treatment decision for themselves if, because of an impairment of or disturbance in the functioning of the mind or brain, he or she is unable to (cls. 8):
understand information relevant to the decision; or
retain information relevant to the decision; or
use or weigh information relevant to the decision; or
communicate the decision (whether by speech, gesture or other means).
Similarly, the Victorian Mental Health Bill (Exposure Draft) provides that a person can only be made subject to a compulsory order if, because of their mental illness, their ability to make decisions about the provision of treatment is significantly impaired (cls. 64(d), 70(c), 71(c)). This ‘significant impairment’ is defined as an inability to:
understand the information relevant to the decision; or
retain that information; or
use, weigh or appreciate that information as part of the process of making the decision; or
communicate the decision in a manner such that another person can understand what the decision is.
The criteria used in these proposed statutory tests broadly reflect the common law formulation for decision-making capacity. If applied correctly, these tests will normally be sensitive enough to identify even the more subtle effects that mental illness can have on decision-making ability. For example, a person with a major depression may have a factual understanding of what it meant to be admitted to hospital, however his or her ability to ‘use’ or ‘weigh’ that information may be compromised if he or she has a belief, rooted in their depression, that they are unworthy of treatment. In these circumstances, he or she could not competently refuse admission to hospital.
If these capacity provisions become law, Victoria and Tasmania would be two of only a handful of jurisdictions in the world, and the first in Australasia, to make consideration of a patient’s decision-making capacity a threshold criteria for compulsory treatment for mental illness (Ryan, 2011a). This represents a major step towards bringing treatment for people living with mental illness in line with the rules applying to medical treatment for people with conditions other than mental illness.
‘Additional harm’ and compulsory orders
The mental health acts of all Australasian jurisdictions currently demand that, before a person with a mental illness can be coercively detained and treated, an examining doctor must consider the possibility of a certain type of harm befalling the mentally ill person or another person. The types of harm to be assessed include current or potential harm to the patient themselves, and the potential harm that the patient poses to others.
With respect to harm to the person themselves, the requirements of the legislation differ in every jurisdiction (see Table 1).
Harm requirements for the making of inpatient orders in Australasian mental health legislation.
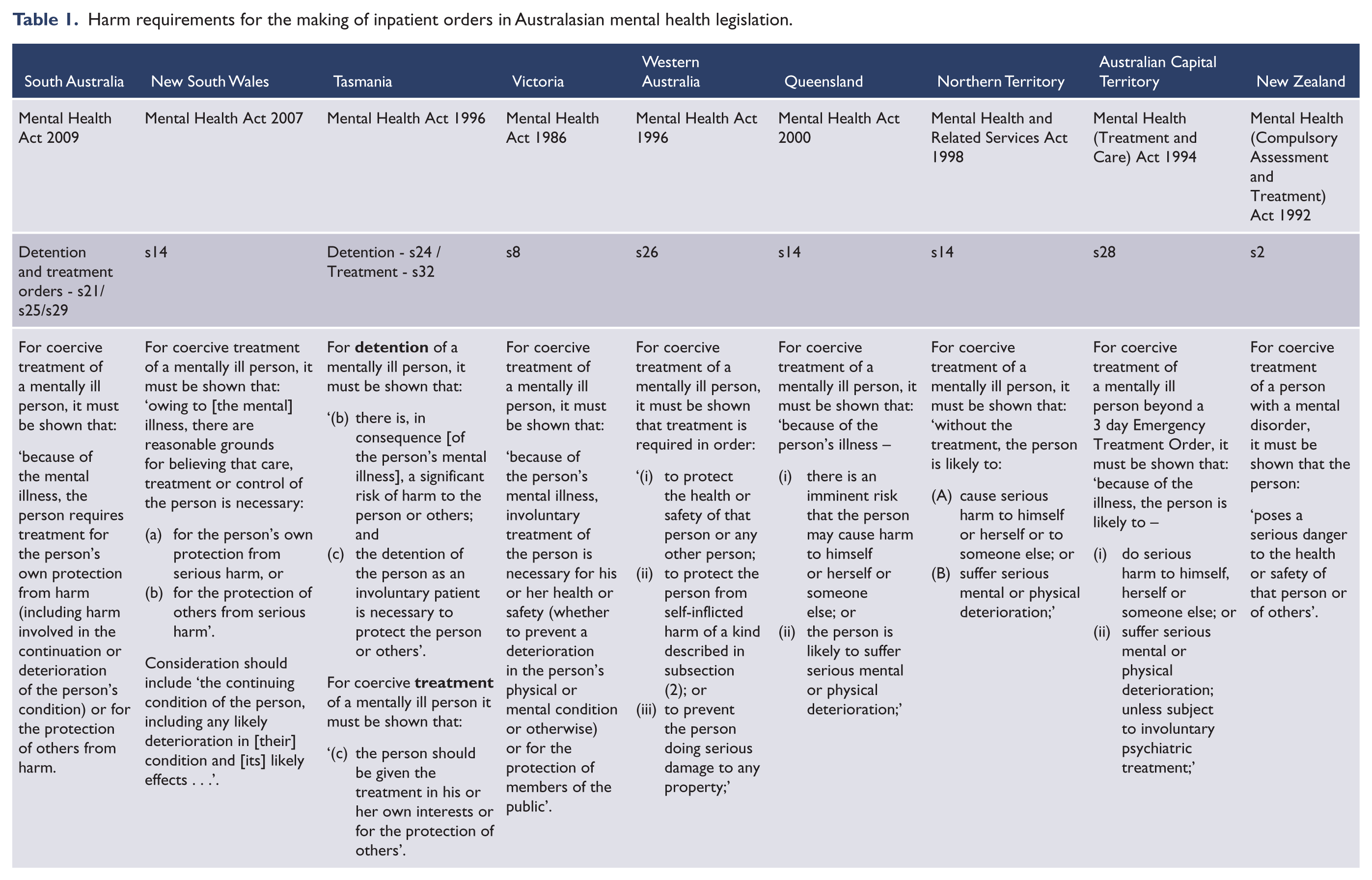
In New South Wales an examining doctor must believe that intervention is ‘necessary for the person’s own protection from serious harm’ (Mental Health Act 2007 (NSW) s. 14). Up until recently, it has not been clear what would constitute ‘serious harm’, and many NSW psychiatrists had taken the view that the Act required serious harm that was more than any harm caused merely by the symptoms of the mental illness. Applying this narrow interpretation, it would not have been sufficient for the person to be suffering serious harm as a result of abusive hallucinations, or distressing delusions, or severely depressed mood; something more would have been required, such as the possibility the patient might commit suicide, or physically deteriorate. However in the recent case of Re J the New South Wales Supreme Court noted that ‘section 14 would permit the continued involuntary detention of a person suffering from mental illness if that were necessary to protect the person from serious harm, being the harm associated with the illness itself’, though White J added that ‘it would be necessary to consider the extent to which the illness was a harm for the person and to assess its seriousness’ (Re J (no. 2) [2011] NSWSC 1224 (‘Re J’) at [101]).
While this statement from Re J is not strictly binding on future cases, it is likely that in New South Wales, if a patient is suffering a mental illness; that illness is causing serious harm; and there is no less restrictive way of protecting the person from that harm, involuntary detention will be permitted under the Mental Health Act 2007 in circumstances where the serious harm is the symptoms of the illness itself. For example crushing, unremitting depression is a serious harm in itself, even without additional concern about the possibility of future suicide, other self-harm or deterioration. The harm to be considered in New South Wales can include harm being experienced at the time of admission, or harm that may occur in the future if treatment is not given.
The South Australian Mental Health Act 2009 also clearly states that the harm to be considered includes ‘the harm involved in the continuation or deterioration of the person’s condition’ – so current harm-causing symptoms of mental illness will provide sufficient warrant for involuntary treatment in South Australia (ss. 10, 16, 21, 25, 29).
In the other jurisdictions however, it may not be possible to treat patients who are ‘only’ suffering harm experienced as the symptoms of the mental illness – even though those symptoms might be severe and debilitating. In these jurisdictions, the Mental Health Acts may require evidence of some ‘additional harm’ occurring, either at the time the patient is assessed or at some time in the future. This might include some additional impact on health and safety beyond that caused by the illness directly.
The Tasmanian Mental Health Act 1996 has a similar requirement to the New South Wales legislation, in that there must be ‘a significant risk of harm to the person’ for a person to be detained in hospital (s. 24). While the statement of the New South Wales Supreme Court in Re J suggests that this requirement might also be interpreted broadly, it would still be open to the Tasmanian courts to give a more narrow reading to the legislation, with the effect that additional harm to the harm caused by the symptoms of mental illness may be required. Also, and unlike New South Wales, the use of the word ‘risk’ suggests that the relevant harm is future harm, not harm being experienced at the time the patient is assessed.
The Victorian and Western Australian acts do not refer to ‘harm’ to the person, but rather, that treatment must be necessary to protect the person’s ‘health or safety’ (Mental Health Act 1986 (Vic) s. 8; Mental Health Act 1996 (WA) s. 26). Again, it is not clear what protection of ‘health or safety’ would include, though in Victoria at least, the second reading speeches for the legislation referred to protection from further deterioration or physical harm, suggesting that the intention of the legislators was that the current symptoms of the illness alone should not be sufficient warrant for involuntary detention (Roper, 1985). However as this has yet to be considered by the Victorian court a wider reading of the requirements is still possible (Ryan, 2011a). The law in New Zealand similarly requires the abnormal state of mind pose ‘a serious danger to the health or safety’ of the person (Mental Health (Compulsory Assessment and Treatment) Act 1992 (NZ) s. 2).
The situation is perhaps most concerning in the two Australian Territories and in Queensland. The law in the Australian Capital Territory and the Northern Territory requires that the examining doctor must believe that the person is likely to cause serious harm to themselves or suffer serious deterioration (Mental Health (Treatment and Care) Act 1994 (ACT) s. 28; Mental Health and Related Services Act 1998 (NT) s. 14). The Queensland Mental Health Act is the same, except that the envisaged harm-to-self need not be ‘serious’, though the risk must be ‘imminent’ (s. 14). In requiring that the harm must be caused by the patient, all three jurisdictions may require an estimation of risk of an act of self-harm by the patient, or evidence of risk of deterioration – and all require an assessment of likelihood of future harm.
With respect to harm-to-self then, the legislation in all Australasian jurisdictions (except South Australia and New South Wales) make it possible for clinicians to interpret provisions so as not to allow coercive treatment unless the affected person is deemed to be either currently suffering some harm or likely to come to some harm in the future, additional to the harm that is inherent in suffering from serious mental illness. If doctors do interpret the provisions this way and do not believe that the person is suffering some ‘additional harm’ or likely to come to some ‘additional harm’, then coercive treatment may only be given if they believe that the person is likely to harm another person.
The statutory requirements in terms of harm-to-others differ again in each jurisdiction (Table 1), but in all, clinicians are required to make some estimate of the likelihood of future harm to others. In New South Wales there must be ‘reasonable grounds for believing that care, treatment or control of the person is necessary . . . for the protection of others from serious harm’ (Mental Health Act 2007 (NSW) s. 14). The law in the Australian Capital Territory and the Northern Territory is similar (Mental Health (Treatment and Care) Act 1994 (ACT) s. 29; Mental Health and Related Services Act 1998 (NT) s. 14). In Tasmania and Queensland the ‘harm’ envisaged is not qualified by the word ‘serious’, however: in Tasmania, there must be a ‘significant risk’ of harm for a person to be detained; and in Queensland the risk must be ‘imminent’ (Mental Health Act 2000 (Qld) s. 14; Mental Health Act 1996 (Tas) s. 24). In Victoria, involuntary treatment must be necessary ‘for the protection of members of the public’, while in Western Australia it must be required to ‘protect the health or safety’ of any other person (Mental Health Act 1986 (Vic) s. 8; Mental Health Act 1996 (WA) s. 26). In New Zealand the abnormal state of mind must pose a ‘serious danger to the health or safety . . . of others’ (Mental Health (Compulsory Assessment and Treatment) Act 1992 (NZ) s. 2).
When mental health laws impose coercive treatment regardless of whether a person has capacity to refuse it, an ‘additional harm’ criterion might be seen to provide some justification for overriding that person’s autonomy. However when coercive treatment can only be imposed if a patient lacks capacity to refuse, as is required under the Victorian and Tasmanian draft bills, there is no need to justify a breach of autonomy, because the person’s refusal is not truly autonomous. In these circumstances, a substituted decision should be made on the patient’s best interests alone. Whether or not the patient is experiencing some ‘additional harm’ or causing harm to others is of no relevance beyond its consideration in a best interests calculation.
In any case, and perhaps more importantly, the increasing evidence that assessments of risk of future harm are of no practical utility and may even cause unnecessary harm by preventing access to treatment for patients who are unable to consent to treatment but for whom treatment would be in their best interests (Large et al., 2008a), only adds to an argument for the removal of criteria that ask clinicians to consider a likelihood of future harm.
In other words, despite the widespread use of ‘additional harm’ criteria in mental health legislation, if patient capacity is the threshold criterion for compulsory treatment, there is no benefit, and quite possibly discriminatory detriment in imposing these extra requirements for access to treatment.
The Victorian Exposure Draft Mental Health Bill clearly includes an ‘additional harm’ criterion for compulsory treatment, requiring clinicians to make estimates of future harm. Mirroring the troublesome provisions of the current Queensland and territory acts, the draft Victorian bill demands that compulsory orders can only be made in circumstances where, if the person is not detained for assessment (cl. 64(c)) or treated (cls. 70(d), 71(d)) there is either ‘an imminent and significant risk that the person may cause serious harm to himself or herself or to another person’ or ‘a significant risk that the person will suffer serious physical or mental deterioration’. This requirement means that patients who lack the capacity to consent to treatment that would return their physical and mental health may not be able to gain access to that treatment if they are not deemed to be at risk of serious self-harm, or serious deterioration. Under the common law, or the Victorian Guardianship and Administration Act 1986 (ss. 42E, 42H), if these patients were medically ill, they would be able to be given treatment which was in their best interests, regardless of whether or not they were thought at risk of ‘self-harm’, ‘harm to others’ or ‘serious deterioration’.
The Tasmanian Exposure Draft Mental Health Bill also requires consideration of the possibility of ‘additional harm’ to the patient, but in far broader terms than the Victorian proposal. When making an involuntary treatment order, the Tasmanian tribunal must be satisfied that (cl. 59):
without treatment, the mental illness will, or is likely to, seriously harm –
the patient’s health or safety; or
the safety of other persons.
It seems likely that the serious harm referred to here could include harm already being suffered at the time the judgement is made, though clinicians will still be trying to make some estimate of future risk to others. Moreover, and although the New South Wales Supreme Court decision in Re J would encourage a wider interpretation, it would remain unclear what serious harm to the patient’s health and safety actually means. It is not clear, for example, that this requirement would permit treatment to be provided to patients who lacked capacity to consent and who would simply be better off if their illness were treated.
It seems that the requirement that treatment must be necessary to prevent ‘serious harm to health’ may constitute a higher threshold for treatment than a ‘best interests’ test – which is currently the basis for treating non mentally-ill patients in Tasmania where they lack capacity and actively object to treatment (Guardianship and Administration Act 1995 (Tas) s. 43).
At the very least, a test focused on harm prevention precludes a more positive focus on the potential benefits of treatment – a balancing of the benefits and disbenefits of treatment. This balancing of all the relevant considerations is just the sort of exercise required in a ‘best interests’ test and would be a fairer and more straightforward approach to treatment decisions for mental illness. Continued reliance on ‘harm prevention’ tests, as opposed to a broader ‘best interests’ test, may have the effect of giving patients with mental illness who lack decision-making capacity more limited access to legitimately required treatment than those with physical illnesses. A differential approach to treatment based only on the type of illness a person has, which would operate to the detriment of patients with psychiatric illness, would seem unfairly discriminatory.
Review of detention
Under international law, all persons are entitled to a fair hearing by an impartial tribunal to decide rights recognised by law (United Nations, 1948: art. 10), including the right not to be detained without lawful excuse (United Nations, 1948: art. 9; United Nations, 1966: art. 9). The Victorian Civil and Administrative Appeals Tribunal recently confirmed that these rights would be engaged by a person seeking review of an involuntary treatment order (Kracke v Mental Health Review Board & Ors (General) [2009] VCAT 646). In addition, the United Nations Principles for the Protection of Persons with Mental Illness and the Improvement of Mental Health Care recommend that the initial review of a decision to admit or retain a person as an involuntary patient should take place ‘as soon as possible’ after the decision (United Nations, 1991: principle 17).
In light of these requirements, both the Victorian and Tasmanian governments have sought to reduce the time that patients wait for compulsory orders to be reviewed by an independent tribunal (State Government of Victoria, 2010: p. 8; Tasmanian Department of Health Human Services, 2007: p. 26; Mental Health Bill 2011 (Tas) (Exposure Draft) part 4). The current Victorian Mental Health Act enables a person who meets the relevant criteria to be detained for a period of 8 weeks before an independent review of the order (s. 30(1)). This is the longest period of detention for treatment without automatic independent review in any Australasian jurisdiction. Currently, in Tasmania, decisions made by a ‘person responsible’ under the Guardianship and Administration Act 1995 to consent to psychiatric treatment on behalf of patients who lack decision-making capacity are not reviewed at all, while involuntary treatment orders made under the Mental Health Act do not need to be reviewed for 28 days (Mental Health Act 1996 (Tas) s. 52).
The Victorian draft bill improves the current arrangements through the introduction of staged orders of fixed duration, however the opportunities for timely and thorough independent review are still unacceptably limited. With extensions of time permitted at various intervals during the staged order process, patients may be compulsorily detained for 6 weeks or longer (Callaghan and Ryan, 2011: pp. 20–22) on an Assessment Order, followed by an Inpatient Treatment Order (both of which are made by psychiatrists) without an independent review of their detention by the tribunal. Indeed, tribunal review is only required if an additional Extended Treatment Order is sought, beyond the initial 4–6 week detention period permitted on doctor-made orders. If an extended order is not sought, no independent review need happen at all. This is not a vast improvement on the current arrangements and falls well short of the standards for compulsory detention set in many other Australian jurisdictions. For example, the Australian Capital Territory only permits emergency detention for 3 days, after which further detention requires an order made by the Mental Health Tribunal (Mental Health (Treatment and Care) Act 1994 (ACT) part 4); in the Northern Territory a review must take place no later than 14 days after admission (Mental Health and Related Services Act 1998 (NT) s. 123); and New South Wales legislation requires review ‘as soon as practicable’ (Mental Health Act 2007 (NSW) s. 27(d)). It also falls well short of the measures proposed in Tasmania.
The Tasmanian review acknowledged that ‘a decision to treat someone without their consent or against their will is a fundamental breach of their right to bodily integrity’ (Tasmanian Department of Health Human Services, 2007: p. 25) and that more stringent safeguards were required to ensure that coercive treatment orders were properly made. The review committee specifically noted that by 28 days after admission (the time that tribunal review is currently required), approximately two-thirds of mental health orders made in Tasmania have been discharged, and that many people who are repeatedly subject to involuntary orders in Tasmania never have their order independently reviewed (Tasmanian Department of Health Human Services, 2007: p. 26). As a consequence, the Tasmanian draft bill provides that all involuntary orders (other than short-term assessment orders made by a medical practitioner) must be made by the tribunal, and applications for those orders must be heard ‘as soon as practicable’ after they are received (Mental Health Bill 2011 (Tas) (Exposure Draft) cl. 58(3)). A single member of the tribunal may make an interim treatment order within 4 days of the assessment order being made (cl. 57(1)), and a full three-member tribunal must hear the matter within 7 days of the expiry of assessment order (cl. 58(4)).
According to the Tasmanian review committee, ‘it is considered in the best interests of the person that independent consideration of the order should occur as soon as possible’ in line with the state’s human rights obligations (Tasmanian Department of Health Human Services, 2007: p. 26). This timely review represents a significant improvement in the protection of the civil rights of psychiatric patients in Tasmania and is likely to serve as a benchmark in other Australian jurisdictions where review is currently unacceptably delayed (Ryan and Callaghan, 2011; Ryan et al., 2010b).
Conclusion
The Victorian and Tasmanian mental health act reviews have broken new ground in achieving equal treatment of Australians with mental illness. If the proposed draft bills become law, capacity will become a fulcrum for coercive psychiatric treatment and people with mental illness in Victoria and Tasmania, who are competent to make their own treatment decisions, will not be able to be treated against their will. The Tasmanian proposal to reduce the wait time for review of treatment orders also furthers the rights protection of people with mental illness.
But for those patients who lack decision-making competence, and for whom treatment would be in their best interests, ‘additional harm’ requirements in both draft bills represent a major continuing difference in the threshold for access to mental health care, as compared with access to treatment for other medical conditions. These requirements deserve close scrutiny to ensure that people whose best interests would be served by treatment are not deprived of care because they fail to meet conditions that would not apply in other healthcare settings.
Even allowing for these concerns, the proposed changes in these two states represent the beginning of a new era of human rights prominence in Australasian mental health law. These changes, and those yet to come, will present some challenges to Australasian psychiatrists, who will now need to have capacity considerations at the front of their minds when making treatment decisions. Nonetheless the increased focus on human rights safeguards should be welcomed for the improved protection they will offer our most vulnerable patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.