
Abstract
Keywords
Introduction
Major depression ranked as the fourth leading contributor to the global burden of disability in 2000 and is projected to become the second cause of disease burden by the year 2020 (Murray and Lopez, 1996). It has been conventionally accepted that it takes about 1 month for antidepressants to fully unfold their action (Quitkin et al., 1984a, b). More recently, this view has been challenged by those who believe that an earlier onset of antidepressants (i.e., before 2 weeks) is highly prevalent and can be highly predictive of later outcomes (Henkel et al., 2009; Szegedi et al., 2009; van Calker et al., 2009). Given that depressive symptoms are likely to be most severe during the early stages of the disorder, when patients seek treatment, it is critically important to relieve these depressive symptoms as soon as possible (Uchida et al., 2010).
Repetitive transcranial magnetic stimulation (rTMS) has been introduced as a promising new treatment option for major depression and has demonstrated beneficial effects (Fregni et al., 2006; George et al., 2000, 2010; Grunhaus et al., 2003; Lisanby et al., 2009; Uchida et al., 2010; Fitzgerald, 2011). Various studies have examined the accelerating or augmenting antidepressant effects of rTMS (Rossini et al., 2005; Rumi et al., 2005; Garcia-Toro et al., 2006; Anderson et al., 2007; Bortolomasi et al., 2007; Brunoni and Fregni, 2010); however, not all of these studies have been positive. A multicentre clinical trial conducted by Herwig et al. (2007) found no accelerating effects of 10-Hz rTMS combined with mirtazapine or venlafaxine. Moreover, most of these studies analysed the accelerating or augmenting effects of rTMS in patients with treatment-resistant depression, while fewer studies have investigated the effectiveness of rTMS in non-drug-resistant major depression patients, specifically those who have started on new antidepressant medication at earlier stages. The safety and efficacy of a treatment plan that includes an accelerated or augmented antidepressant response in combination with rTMS therapy in first-episode depressed patients is unknown.
The primary objective of this study was to determine if a treatment strategy composed of 2-week rTMS treatments in combination with antidepressant medication in first-episode young depressive patients would result in a greater number of patients exhibiting signs of early improvement (as determined by a reduction in their 17-item Hamilton depression rating scale (HAMD-17; Hamilton, 1960) score of ≥20% within the first 2 weeks of treatment) and response (as determined by a reduction in HAMD-17 score of ≥50%). The secondary objective of this study was to determine the effect of rTMS treatment in combination with medication (citalopram) on HAMD-17 and Montgomery–Asberg depression rating scale (MADRS) rating scores compared to sham-stimulated patients.
It is important to note that the criteria of a 20% score reduction has been chosen as an early indicator of improvement because it can be reliably measured in clinical trials and is a highly sensitive predictor of a later stable response or stable remission of depression (Henkel et al., 2009; Szegedi et al., 2009). However, a change of 20% is not a sensible target score for therapeutic intervention and should not be understood as such.
Participants and methods
Study participants
Patients diagnosed with major depression were recruited from the first affiliated hospital of Zhejiang Medical University. Inclusion criteria used in this study for patient selection were: (1) patients were between 18–45 years old; (2) males and females; (3) patients with a DSM-IV clinical criteria for major depressive episode; (4) patients who demonstrated a HAMD-17 score >18; and (5) patients who are experiencing their first depressive episode. Patients were excluded if they fell into any of the following categories: (1) were left-handed; (2) demonstrated psychotic symptoms; (3) exhibited a severe and unstable physical illness; (4) had a history of head injury or seizure disorder; (5) were diagnosed with bipolar disorder; (6) had metal implants; and (7) were pregnant.
This study was approved by the medical ethics committee in the first affiliated hospital of Zhejiang Medical University in April of 2007 (Ethical Research Review 2007, No. 1), and was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). All patients provided their written and informed consent. Patients were randomly assigned to either the sham or active stimulation group and received rTMS treatment on 10 consecutive workdays (Monday to Friday, for a period of 2 weeks).
The rTMS sessions were performed with 20 mg citalopram daily for the first 2 weeks. During the following 2 weeks, the patients continued with citalopram treatment in the absence of stimulation. Patients were administered 40 mg citalopram daily if the reduction of their HAMD-17 scores were below 50% within the first 2 weeks of treatment. No other antidepressant or concomitant antipsychotic medication was given to the patients. In addition, the rater in this study was blind to the rTMS and sham-stimulation conditions.
Clinical assessment
The severity of depression was assessed using HAMD-17 and MADRS at 0 (baseline), 1, 2, and 4 weeks.
The HAMD-17 was used as the primary outcome of measure and the MADRS as a secondary outcome of measure. Similar to previous reports, we grouped our patients accordingly: (1) early improvers, patients having an HAMD-17 score reduction of ≥20% below baseline within the first 2 weeks of treatment; (2) treatment responders, patients having an HAMD-17 score reduction of ≥50% below baseline; and (3) symptom remitters, patients having an HAMD-17 score reduction of ≤7 points below baseline (Szegedi et al., 2009).
Neuropsychological assessment
Neuropsychological tests were administered to assess executive function at baseline and 2 weeks after treatment. As the dorsolateral prefrontal cortex (DLPFC) was the target stimulation area, three different tasks assessing frontal executive functions were used.
Wisconsin Card Sorting Test (WCST, modified version; Nelson, 1976)
Subjects were asked to sort 48 cards on the basis of three possible categories (colour, number, and shape). After six consecutive correct responses, subjects were asked to change the sorting principle to another category. The test ended when subjects completed all six categories correctly or used all 48 cards. The total trials, correct trials, total number of errors, perseverative errors, random errors, and categories were recorded.
Trail-Making Tests (TMT; Reitan, 1958)
In part A, the subjects were required to quickly draw lines to connect consecutively numbered circles. In part B, the subjects were asked to alternately combine numbers with different colours in ascending order. The task completion was measured in seconds.
Stroop Color–Word Test (SCWT; Stroop, 1992)
In part 1, the subjects were asked to read out three written colours printed in black ink as fast as possible. Then, in part 2, the subjects were instructed to name the colour as fast as possible. Finally, in part 3, the subjects were required to name the ink colour of a colour word as fast as possible. The colour word was not the same as the ink colour. The performance for each condition was calculated by the processing time per item in seconds. The reaction time difference in part 3 relative to part 2 is called the ‘interference’ effect.
Stimulation parameters
A Magstim rapid stimulator with a figure-8 coil (Magstim, Sheffield, UK) was used for treatment. Each patient underwent five weekly sessions that lasted for 2 weeks. Each session included 800 stimuli/day delivered in 20 trains of 10-Hz rTMS at 90% of the motor-evoked potential threshold. Each train lasted 4 s with a 56-s inter-train pause. Before each session, the resting MT was defined as the lowest intensity able to induce a visible muscle contraction in five of 10 trials, an involuntary movement of the right abductor pollicis brevis muscle (thumb). In each treatment session, stimulations were delivered to the left DLPFC, which is defined as the site 5.5 cm anterior in a mid-sagittal plane from the site for MT determination. For the sham group, subjects received the same number of stimuli, with parameters identical to those in the active group, but the coil was turned 90°, with only 1 wing in contact with the edge on the left DLPFC, which produces the same sound (Rossini et al., 2005). The TMS treatments were assigned by a random number list. The patients were naive to rTMS prior to the study and were not familiar with the differences between sham and active rTMS regarding acoustic and tactile aspects.
Statistics
Intent-to-treat analysis was performed and last observation carry forward was used for missing values. Data were analysed for normal distribution (Kolmogorov–Smirnov test). Independent sample t-tests were used to investigate the differences between the groups for demographic and baseline clinical variables for normal distribution data. The Mann–Whitney U-test is often viewed as the nonparametric equivalent of the Student’s t-test if the data is not of normal distribution. Changes in HAMD-17, MADRS scores, and neuropsychological assessments over time were analysed with repeated-measures analysis of variance (ANOVA). Post-hoc comparisons were performed with the paired t-test adjusted for multiple comparisons by the Bonferroni method. The differences between the active and sham rTMS groups in changes from baseline, at 1, 2, and 4 weeks, were analysed with linear contrasts for the time multiplied by the rTMS interaction. Pearson χ2 tests were used to investigate the differences between groups in the rates of early improvers, responders, and remitters at 2- and 4-week time points. Pearson correlations were used for correlation analysis. All statistical tests were two-tailed and a p-value <0.05 was considered to be significant. Statistical analyses were performed using SPSS Version 11.0.
Results
Demographics
The study had a total of 60 patients, and only 56 subjects had completed all treatments (Figure 1). Two patients in the active rTMS group chose to stop the study because of pain at the site of stimulation, and two other patients treated under the sham condition were unable to tolerate the sound of the stimulation and dropped out of the study. In the active rTMS group, three patients reported mild cephalgia that lasted for a few hours and three patients complained of fatigue. There were no seizures (a possible adverse effect of rTMS) during the course of the stimulation. Patients in the sham rTMS group did not report any symptoms related to cephalgia or fatigue and there were no patients who experienced mania during the study.
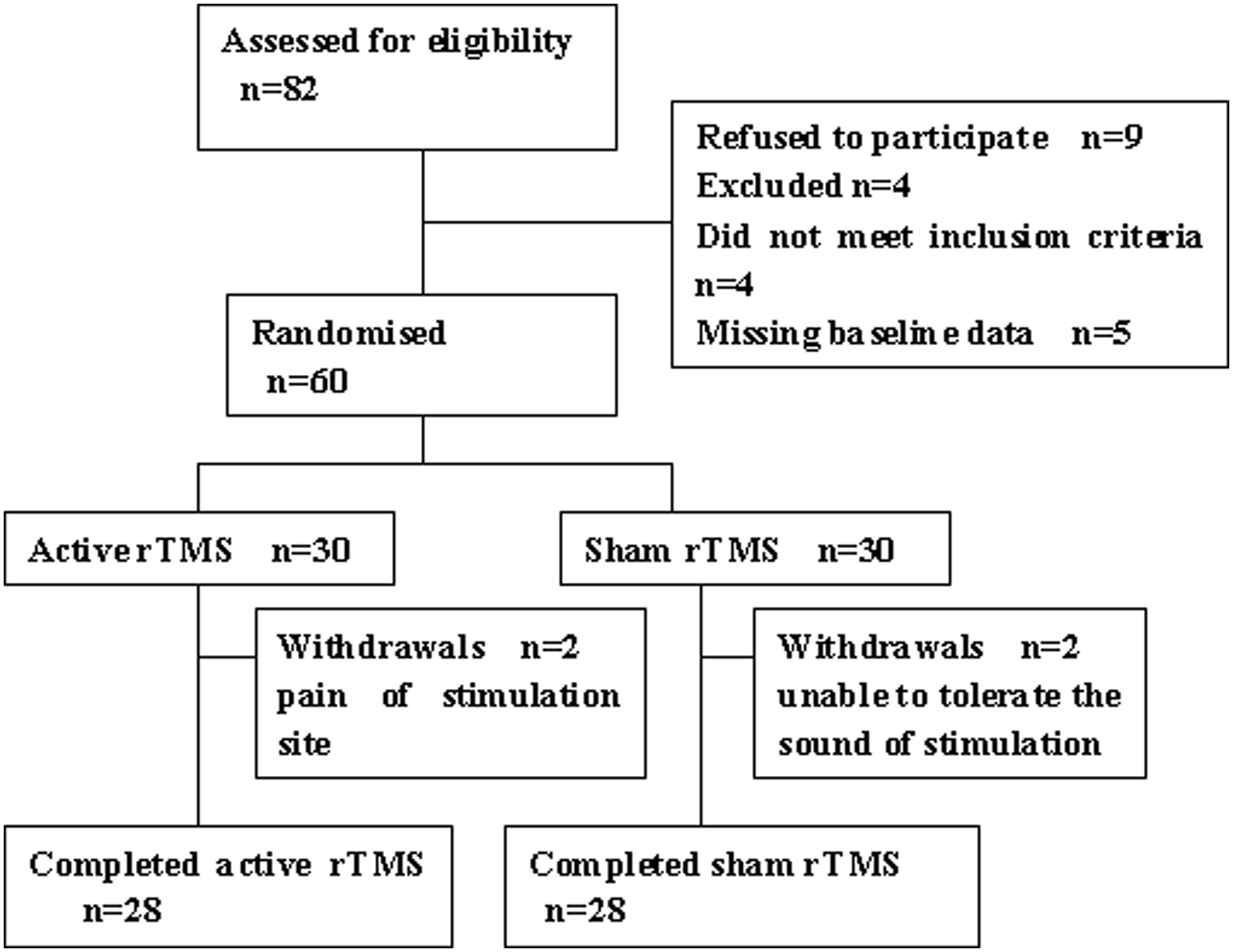
Consort flow chart
Seventeen patients in the active group and twenty patients in the sham group were administered 40 mg citalopram daily at the end of the second week because the reduction in their HAMD-17 scores was less than 50% compared to baseline. The two groups did not differ in terms of age, gender, education, marital status, the duration of the current episode, age at onset, or the dosage of medication. Relevant demographic and clinical characteristics of the two treatment groups are shown in Table 1.
Demographic and clinical characteristics of patients
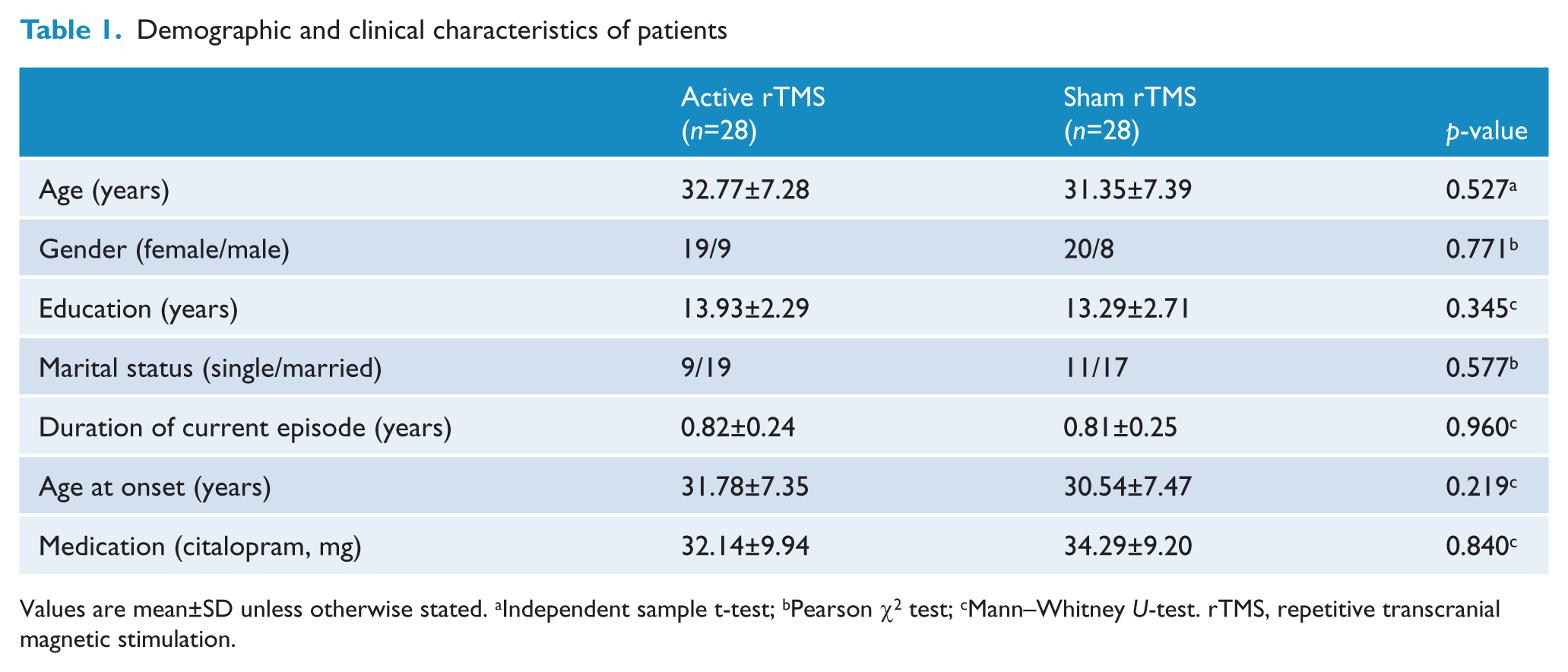
Values are mean±SD unless otherwise stated. aIndependent sample t-test; bPearson χ2 test; cMann–Whitney U-test. rTMS, repetitive transcranial magnetic stimulation.
Primary and secondary efficacy outcome
The ratio of early improvers (who demonstrated a 20% reduction of HAMD-17 scores) was significantly higher in the active than the sham rTMS group (57% vs. 29%, χ2=4.667, p=0.031) within the first 2 weeks of treatment. There were no significant differences observed in responder rates (a 50% reduction of HAMD-17 scores) between the two treatment groups (39% vs. 29%, χ2=0.319, p=0.572) and at 2- and 4 weeks (46% vs. 36%, χ2=0.295, p=0.586). Remission of depression, which was evaluated at the end of the study, was found in 11 patients in the active group and in seven patients in the sham group. No difference was observed between the two groups regarding the ratio of remission (39% vs. 29%, χ2=0.319, p=0.572).
The active rTMS group demonstrated a HAMD-17 score reduction over time compared to the sham rTMS group, as shown in Figure 2. The main effect of each time point (active rTMS: F=575.24, p=0.000; sham rTMS: F=374.02, p=0.000) showed that depression scores significantly declined after treatment in both groups using repeated-measures ANOVA (Table 2). The time×group interaction does not indicate a difference at the end of the first week, but rather a difference in symptom change over time (F=23.586, p=0.000). Post-hoc comparison of HAMD-17 scores was performed. We observed no difference at the 1-week time point (t=2.851, p=0.097), but a significant difference was found at the 2-week time point (at the end of rTMS; t=13.444, p=0.001) that remained significant until the fourth week of treatment (t=46.915, p=0.000).
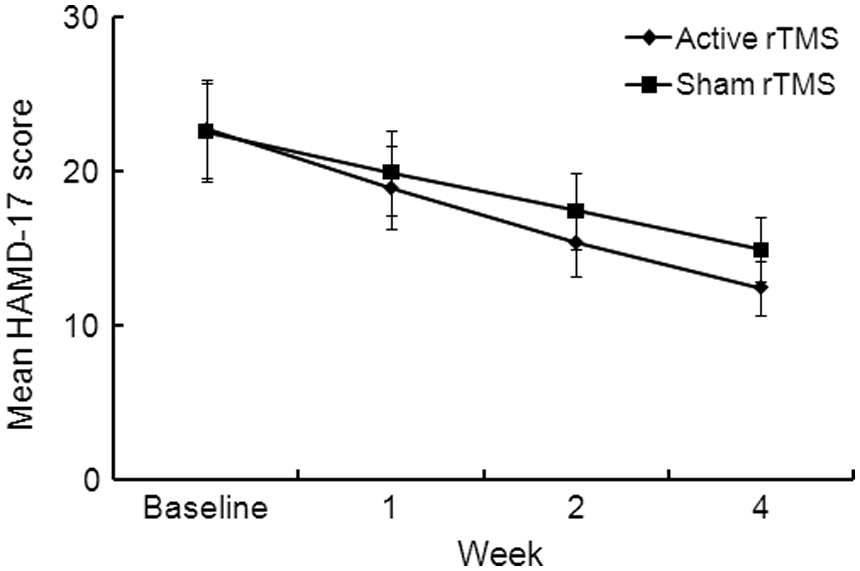
Reduction in 17-item Hamilton depression rating scale (HAMD-17) total score over time in active repetitive transcranial magnetic stimulation (rTMS) vs. sham rTMS groups
The effects of time and group variables on total score on Hamilton depression rating scale – 17 items
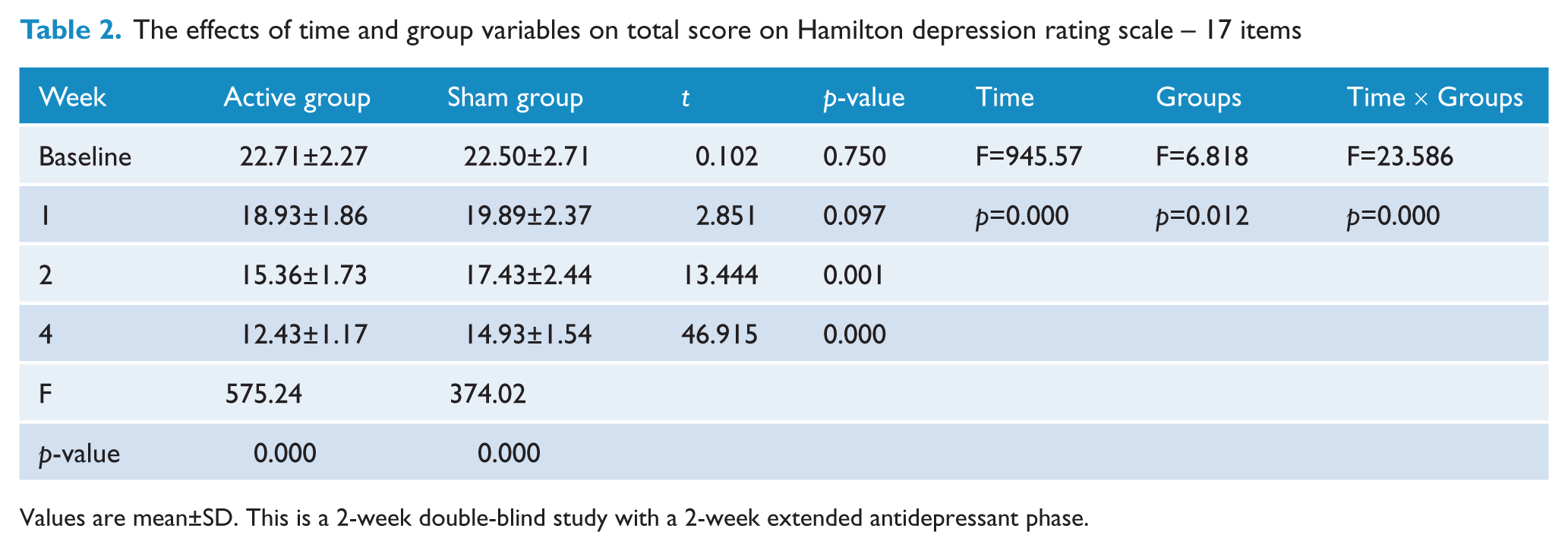
Values are mean±SD. This is a 2-week double-blind study with a 2-week extended antidepressant phase.
Consistently with the HAMD-17 score results, the MADRS scores improved over time (active rTMS: F=736.72, p=0.000; sham rTMS: F=259.34, p=0.000; Figure 3). Based on a post-hoc comparison of MADRS scores (Table 3), there was a significant difference between the two groups, with a lower MADRS score in the active rTMS group compared with the sham rTMS group after 2 weeks (23.82 vs. 28.32, t=30.123, p=0.000) and 4 weeks (18.39 vs. 23.21, t=39.996, p=0.000). Thus, no significant differences in HAMD-17 or MADRS scores were found between the two groups at baseline or after 1 week of treatment.
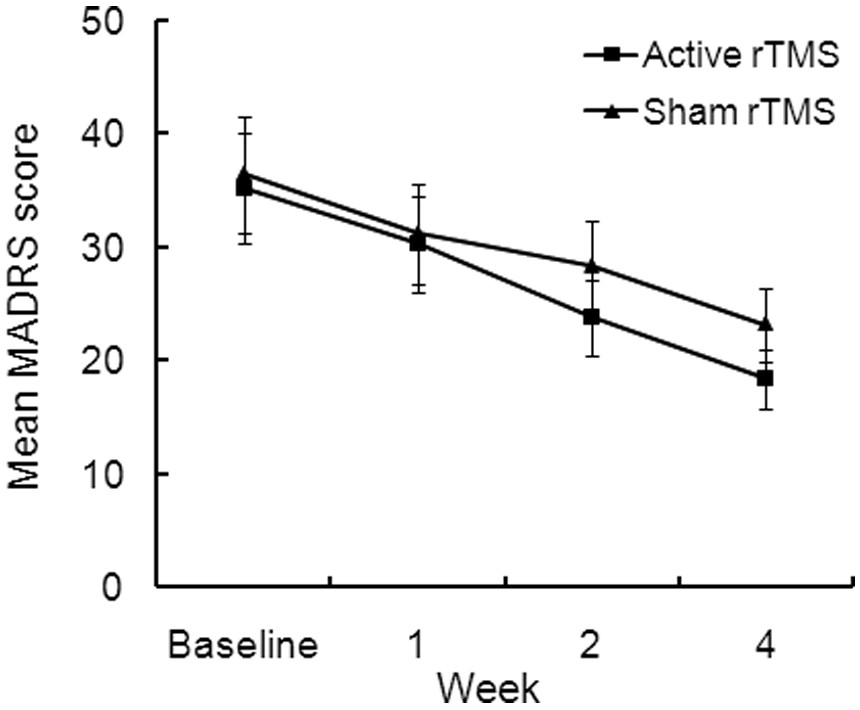
Reduction in Montgomery–Asberg depression rating scale(MADRS) total scores over time in active repetitive transcranial magnetic stimulation (rTMS) vs. sham rTMS groups
The effects of time and group variables on total score on Montgomery and Asberg depression rating scale
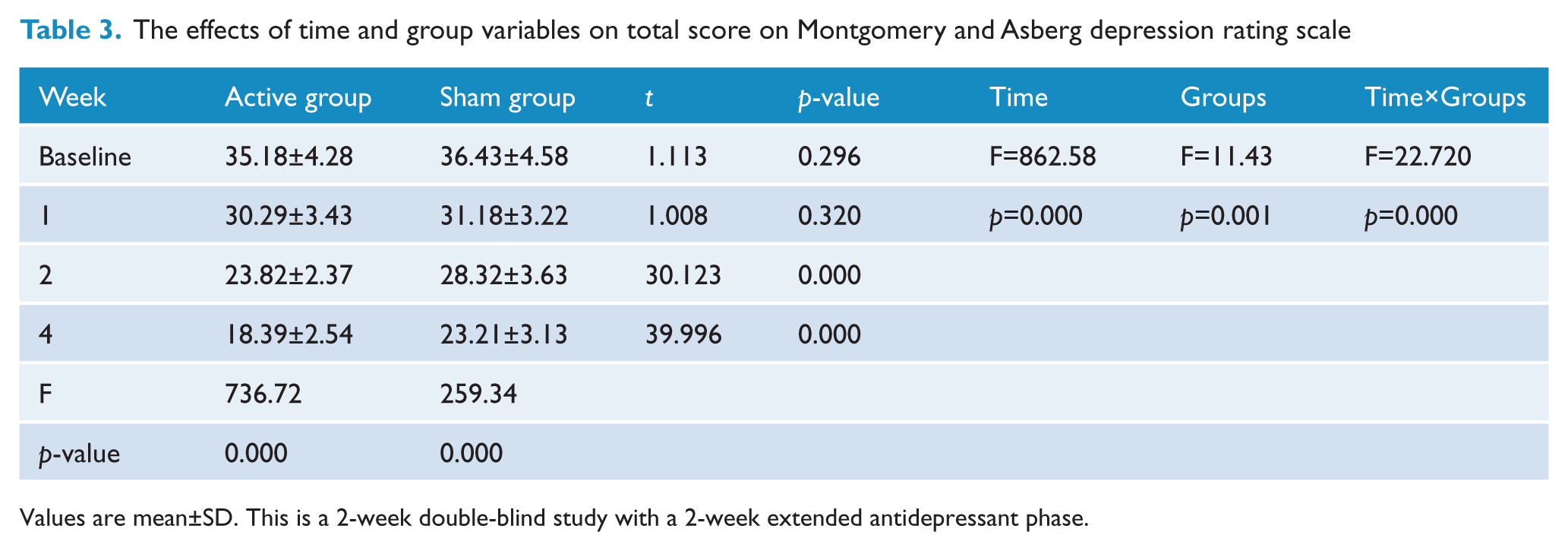
Values are mean±SD. This is a 2-week double-blind study with a 2-week extended antidepressant phase.
Neuropsychological assessments
Baseline neuropsychological ratings did not differ between the active and sham-stimulation groups (WSCT, TMT, and SCWT; independent sample t-tests). The neuropsychological test score results from this study are summarized in Table 4.
Neuropsychological rating of patients
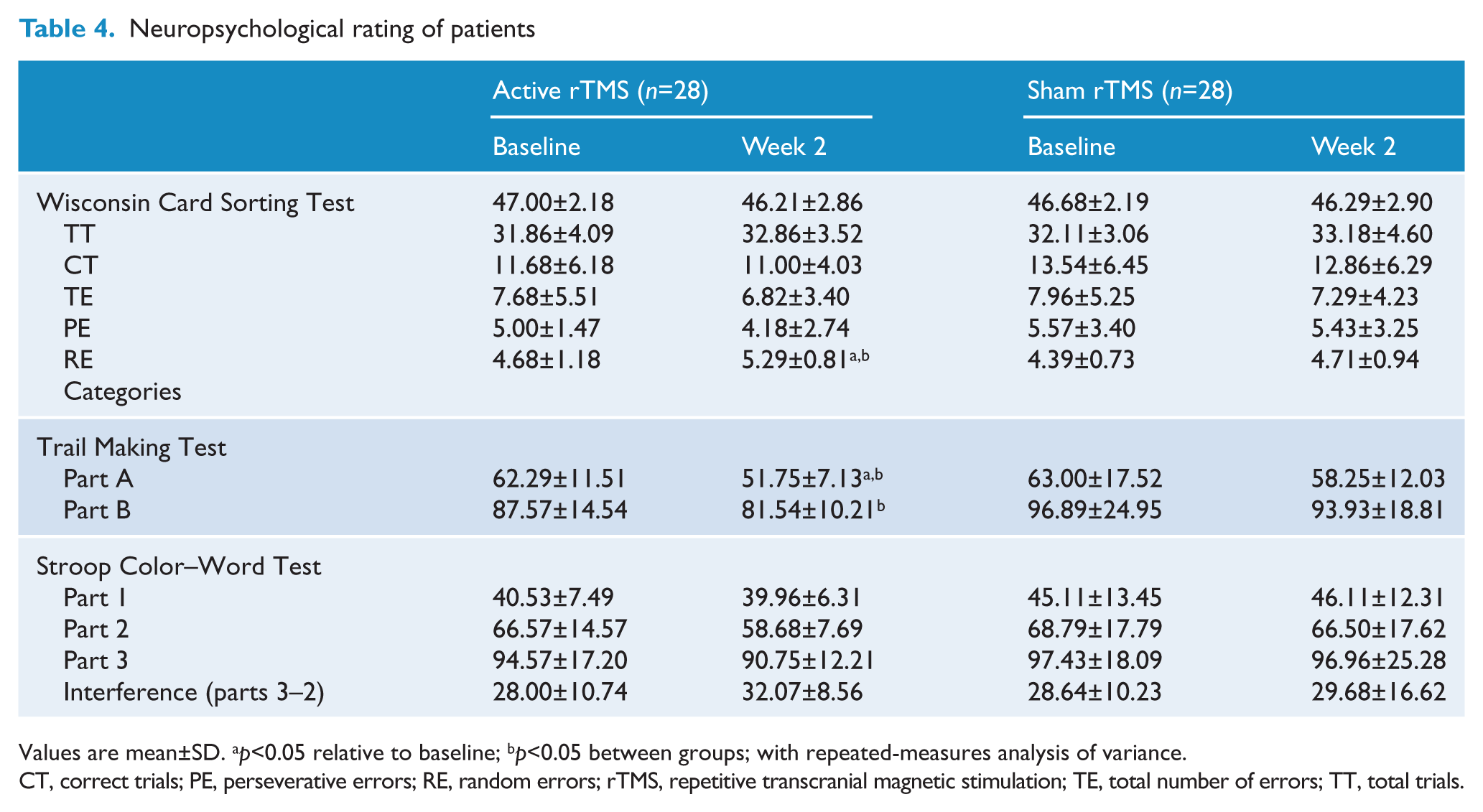
Values are mean±SD. ap<0.05 relative to baseline; bp<0.05 between groups; with repeated-measures analysis of variance.
CT, correct trials; PE, perseverative errors; RE, random errors; rTMS, repetitive transcranial magnetic stimulation; TE, total number of errors; TT, total trials.
In the WSCT task, the perseverative errors and total errors did not change during the study and did not differ between the two groups. However, we found that the depressed patients in the active rTMS group completed more categories compared to the sham group (F=4.11, p=0.048) and performed significantly better compared to their baseline scores (F=4.99, p=0.03), as revealed by repeated-measures ANOVA.
In the TMT, the depressed patients in the active rTMS group completed part A of the examination faster compared to either baseline (F=16.95, p=0.007) or the sham group (F=5.30, p=0.025) at week 2. Performance on part B of the TMT did not differ between the two groups at baseline, but a difference was found at week 2 (F=7.55, p=0.008).
Performance on the SCWT did not differ during the study.
Correlation analysis
Correlation analyses were performed to check for an association between executive function measures and clinical or demographic variables. There was no correlation found between the clinical ratings of symptom severity and the cognitive scores of depressed patients in both groups. We also found that the number of years of education of depressive patients was negatively correlated with the processing time for SCWT part 3 (word-colour page; r=−0.259, p<0.05).
The correlation coefficients of scores of the frontal executive tests were calculated for the two groups combined. The number of completed categories in the WSCT was negatively correlated with the completion time found in part A (r=−0.31, p<0.05) and part B of the TMT (r=−0.34, p<0.05).
Discussion
We used the DLPFC as our target of stimulation according to previous studies. This localization is based on the historical observation of depression-related hypometabolism of the prefrontal cortex. As reviewed by Loo and Mitchell (2005), it has been suggested that rTMS may be less effective in psychotic depression (Grunhaus et al., 2003), elderly subjects (Fregni et al., 2006), and those with depressive episodes of longer duration (Holtzheimer et al., 2004). Based on the previous studies, we chose to assess the effects of left DLPFC rTMS in young patients with first-episode major depressive disorder in the absence of psychotic symptoms. We observed significant antidepressive effects after left frontal high-frequency rTMS. This finding is consistent with previous reports (George et al., 2000, 2010).
In previous studies, rTMS has been studied as an adjunctive treatment for drug-resistant patients. One key aspect of the present study is that we assessed the effectiveness of rTMS started simultaneously with antidepressant medications in first-episode, untreated major depressive patients in the early treatment stage. The use of rTMS as an additional strategy in conjunction with antidepressant medication resulted in a greater number of early improvers after the 2-week stimulation treatment, but we found no significant difference in the number of responders and remissions at the end of the fourth week. The active rTMS group showed a significantly faster reduction in both the HAMD-17 and MADRS scores compared with the sham group at weeks 2 and 4. This finding is in agreement with other previously controlled studies (Rossini et al., 2005; Rumi et al., 2005), but is inconsistent with Herwig et al. (2007). Unfortunately, it is very difficult to compare our study with other studies because of the differences in stimulation parameters, patient populations, and study designs. It has been suggested that less medication resistance, younger age, and shorter illness duration would be associated with the superior antidepressant efficacy of rTMS (Brunoni and Fregni, 2010).
In this study, no serious adverse effects were reported in any group, except for the pain at the stimulation site reported by two patients, mild cephalgia reported by three patients, and fatigue noted by three patients in the active rTMS group.
Although rTMS seems to be a new tool for treating depression, reports on the executive performance of rTMS treatment in depressed patients during early treatment stages are very limited. Our results indicated that the patients did not deteriorate in executive performance during the study, and even improved in categories on the WCST and completed the TMT faster in the active group. Some studies have also shown significant improvements in response speed, procedural learning, verbal and visuospatial memory, and verbal fluency in cognitive examinations (Martis et al., 2003; Fabre et al., 2004; Hausmann et al., 2004; Schulze-Rauschenbach et al., 2005).
There were some limitations found in this study: (1) the patients were treated with antidepressants, which may have affected executive functioning; consequently, drug-free patients should be investigated in future studies to determine whether prefrontal cortex rTMS has the potential to modulate frontal lobe activity during executive function. (2) we didn’t calculate the sensitivity (early improvers who became stable responders or stable remitters/the total stable responders or stable remitters) or the specificity (early non-improvers who did not become stable responders or stable remitters/the number of patients who did not become stable responders or stable remitters) because of the small sample sizes and short observation periods; (3) the 2-week period of rTMS appeared rather short and the intensity and number of pulses chosen were relatively conservative, because (a) we did not know what kind of rTMS parameters would be beneficial for Chinese people at the start of our study and (b)we studied first-episode, untreated young major depressive patients who were starting on new antidepressant medication; (4) 90° angling was used as sham rTMS for depression; this condition might deliver a slight magnetic field and evoke negligible physiological effects, but compared with real rTMS condition, it does not elicit a comparable sensation on the patient’s scalp and this may have created different expectations about its therapeutic effects (Rossini et al., 2005).
Given the substantial delay in the symptomatic improvement observed with antidepressants, another potential benefit of rTMS is that it accelerates the rapidity of the antidepressant response in first-episode depression. In addition, rTMS as a therapy has some advantages, such as a very low rate of serious adverse effects and lack of drug interaction issues (Brunoni and Fregni, 2010).
Conclusion
These results indicated that rTMS accelerated the rapidity of the antidepressant response in young patients with first-episode major depressive disorder despite the use of a low dose and short duration treatment. Treatment of rTMS was safe from adverse events and effects on executive function. Our results call for further rTMS studies using larger sample sizes, high intensity of stimuli, and longer duration to draw more definitive conclusions.
Footnotes
Acknowledgements
We thank Dr Mikhail Pletnikov from the Department of Psychiatry and Behavioral Sciences, Johns Hopkins School of Medicine, for his helpful comments on this paper and help with English grammar, Shu-Lan Li for help with the stimulations, and Yi Shen for his statistical advice throughout the entire project.
Funding
This research was supported by the Department of Health Foundation of Zhejiang Province (grants 2006B027 and 2007B065), the Department of Traditional Chinese Medicine Science Foundation of Zhejiang Province (grant 2009CA062), and the Education Bureau of Zhejiang Province (grant Y201019141).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.