
Abstract
Introduction
Around 25–55% of people with schizophrenia of over 2 years’ duration are partially or not at all responsive to antipsychotic medication (Pantelis and Lambert, 2003). For people with treatment-resistant schizophrenia and schizo-affective disorder, clozapine, which was the first of the atypical or second generation antipsychotics, is advocated as the ‘treatment of choice’ by the Royal Australian and New Zealand College of Psychiatrists (2005). Clozapine acts on multiple neurotransmitter pathways including dopamine, serotonin, adrenergic and muscarinic systems, enabling it to treat positive (e.g. hallucinations and delusions) and negative (e.g. lack of interest and motivation) psychotic symptoms (Ashby and Wang, 1996). Between 30 and 60% of patients whose symptoms do not respond to first-choice antipsychotic medication, show improvement on clozapine (Kane et al., 1988; Lieberman et al., 1994). With limited striatal dopamine actions, this clinical efficacy is associated with a low risk of extrapyramidal side effects (e.g. tremor, muscle stiffness) (Kane et al., 1988).
Despite clear clinical benefits with clozapine, there are significant safety concerns regarding its use (Berk et al., 2007; Fitzsimons et al., 2005; Iqbal et al., 2003). Clozapine can cause potentially life-threatening side effects, due in particular to haematological and cardiac effects. Agranulocytosis and neutropenia (reductions in white blood cells levels) occur in about 0.18–0.80% of people taking clozapine (Alvir and Lieberman, 1994; Stübner et al., 2004), with myocarditis and cardiomyopathy occurring in 0.015–0.188% (Merrill et al., 2005). Other potential complications include weight gain and an increased seizure risk (Castle et al., 2006; Fitzsimons et al., 2005).
Consequently, in Australia, the Therapeutic Goods Administration (TGA) has implemented compulsory haematological and cardiac monitoring standards to minimize the risk of clozapine side effects. Clozapine is classified as a ‘highly specialized drug’ and can only be prescribed by psychiatrists specifically registered to do so. General practitioners (GPs) can prescribe clozapine after initiation by a psychiatrist, but cannot alter the dose. Therefore, a person taking clozapine generally gets their prescription from a psychiatrist, obtains it from a pharmacy registered to dispense this medication, and has frequent blood tests (initially weekly, then monthly depending on the results) and careful physical monitoring (Castle et al., 2006).
Clozapine treatment is usually initiated during a hospital admission for optimal medical monitoring. Once stabilized on clozapine, patients are discharged to a public community mental health service (CMHS), under the care of a psychiatrist and case manager. In the community, care occurs via three pathways:
The patient continues being managed in a public CMHS;
The patient becomes engaged in a GP shared- care arrangement with their clozapine treatment monitored by a GP while seeing their CMHS case manager less frequently, and retains a consultant psychiatrist at the CMHS who they see six-monthly or sooner if required;
The patient is discharged from the CMHS to receive sole treatment from a private psychiatrist.
While there is extensive research documenting the efficacy and side-effects of clozapine, and published treatment and monitoring guidelines, (Castle et al., 2006; Collins et al., 1992; Kane et al., 2003; Ronaldson et al., 2011) there has been little research into systemic models for supporting people taking clozapine. Due to the compulsory monitoring requirements, treating people taking clozapine can be costly and labour intensive (Rosenheck et al., 2003; Sernyak et al., 2001). This may result in patients taking clozapine being retained within the public mental health service beyond their rehabilitation needs due to the complexity of their medical management. Moving patients taking clozapine from CMHS into less intensive models of care (e.g. private psychiatrist or GP shared care) will reduce treatment costs and burden for the public mental health service, while freeing up spaces to accept new patients. This is particularly important as clozapine prescription has increased by 78% in Australia over the last 10 years (Malalagama et al., 2011). For the patients taking clozapine, being managed in a less intensive and restrictive manner may provide more normality, flexibility, improved quality of life, greater satisfaction, and reduced stigma.
With the current lack of research into the factors contributing to the success of this transitioning, this paper aims to explore the perceived transition barriers and criteria used by staff to identify patients that are suitable for transition from the public to private/GP shared-care setting.
Method
Sample
A total of 215 staff involved in the care of people taking clozapine were invited to participate in the study. This included 60 staff from the Alfred CMHS based in Melbourne, Australia, 120 local private psychiatrists registered to prescribe clozapine, and 35 local GPs involved in the Bayside Health clozapine GP shared-care programme. This project was approved by the Alfred Research and Ethics Committee.
Measures
Clozapine transition questionnaire (CTQ)
Key stakeholders involved in the treatment of patients taking clozapine in the Alfred CMHS were interviewed individually and in focus groups by author SF using both closed- and open-ended questions about the experience of transitioning patients taking clozapine, the perceived barriers, and the criteria used to select suitable patients (e.g. clozapine coordinator; clozapine assistants; psychiatrists; psychiatric nurses; pharmacists; psychologists; researchers). Authors SF and AW interviewed representatives from the private psychiatry sector (e.g. clozapine coordinator in a private psychiatric hospital; nurse manager of a private psychiatric service; private psychiatrists). Author AW met with GPs engaged in the Bayside Health clozapine GP shared-care programme to obtain their perspective. Information from the Bayside Health clozapine protocols and clinical guidelines supplemented the data collected. Thematic analysis was applied to the transcripts and information obtained from the various staff interviews to determine the items of the CTQ. Once the CTQ was developed, it was piloted in a small sample of clinicians and researchers from the Alfred for ease of completion, comprehension, and content. Appropriate format changes were made based on the feedback from the staff who piloted the CTQ.
The CTQ is divided into 3 sections. Section 1 identifies 14 barriers (see Table 1), and asked staff to rate the impact of each barrier on the transitioning process (1 = no impact, 2 = some impact, 3 = significant impact, 4 = impact so significant that it prevents the process). Staff could list additional barriers. Section 2 consists of general questions about the experience of transitioning patients taking clozapine from the public to private/GP shared-care setting. Section 3 lists 12 criteria (see Table 2) used to determine if a patient taking clozapine is ready to transition and asked staff to rank the level of importance of each (1 = not important, 2 = somewhat important, 3 = very important). Staff could list additional criteria.
Mean (SD) ratings of barriers to transitioning patients taking clozapine from public to private/GP shared-care settings
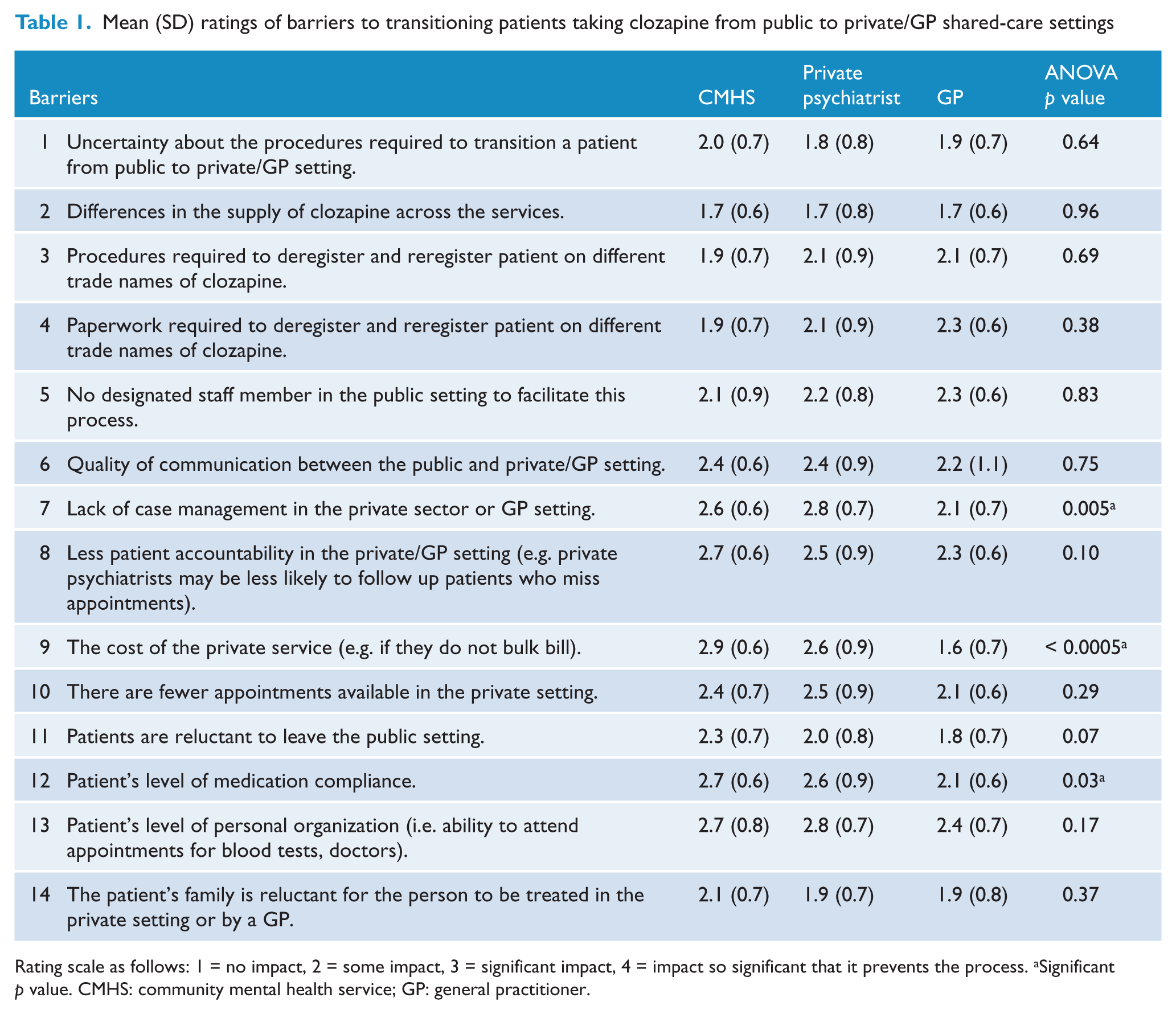
Rating scale as follows: 1 = no impact, 2 = some impact, 3 = significant impact, 4 = impact so significant that it prevents the process. aSignificant p value. CMHS: community mental health service; GP: general practitioner.
Mean (SD) ratings of criteria used to determine if a patient taking clozapine is suitable for transitioning from the public to the private/GP shared-care setting.
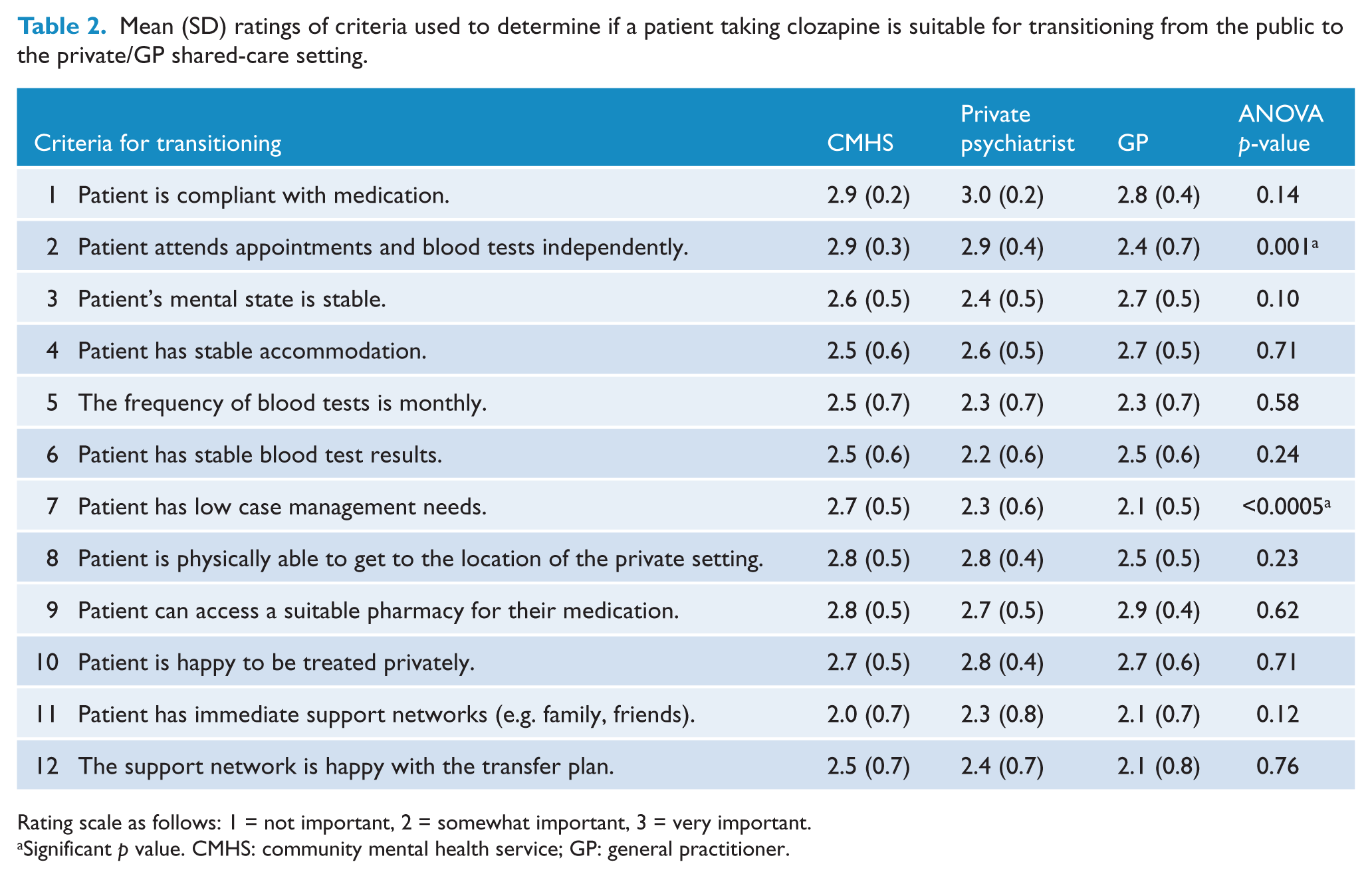
Rating scale as follows: 1 = not important, 2 = somewhat important, 3 = very important.
Significant p value. CMHS: community mental health service; GP: general practitioner.
Procedure
The CTQ and an introductory letter were provided by the clozapine coordinator to staff of the Alfred CMHS at usual team meetings, and mailed to private psychiatrists and GPs. The introductory letter encouraged all clinicians to complete the CTQ even if they had not been directly involved in the process of transitioning a patient taking clozapine. Participants were given a reply paid envelope to return the completed questionnaire, and the CTQ was anonymously completed.
Statistical analysis
General descriptive statistics were calculated. Work area group differences in the ratings of the transitioning barriers and criteria were explored using one-way analysis of variance (ANOVA), with Scheffé’s post hoc comparisons used to identify pairwise differences between work areas.
Results
Sample characteristics and participant experience in transitioning clozapine patients
Of the 215 questionnaires sent out 42 were returned via post marked ‘return to sender’. A total of 80 completed CTQs were returned (overall response rate = 46.2%) with 34 from the Alfred CMHS (56.7%); 29 from private psychiatrists (37.2%) and 17 from GPs (48.6%), with overall no significant differences in the response rates from the three clinician groups, χ2(2, n = 173) = 5.28, p =0.07. Equal numbers of men and women completed the questionnaire (see Table 3) and most participants were doctors (70.3%). Most participants (64.6%) had been involved in transitioning a patient between public and private/GP shared care, and of these around half said it was a ‘worthwhile treatment option’, ‘it went really smoothly’ and the ‘patient was satisfied’.
Participants’ demographics and experience regarding the transitioning of patients taking clozapine from public to private/GP shared-care settings
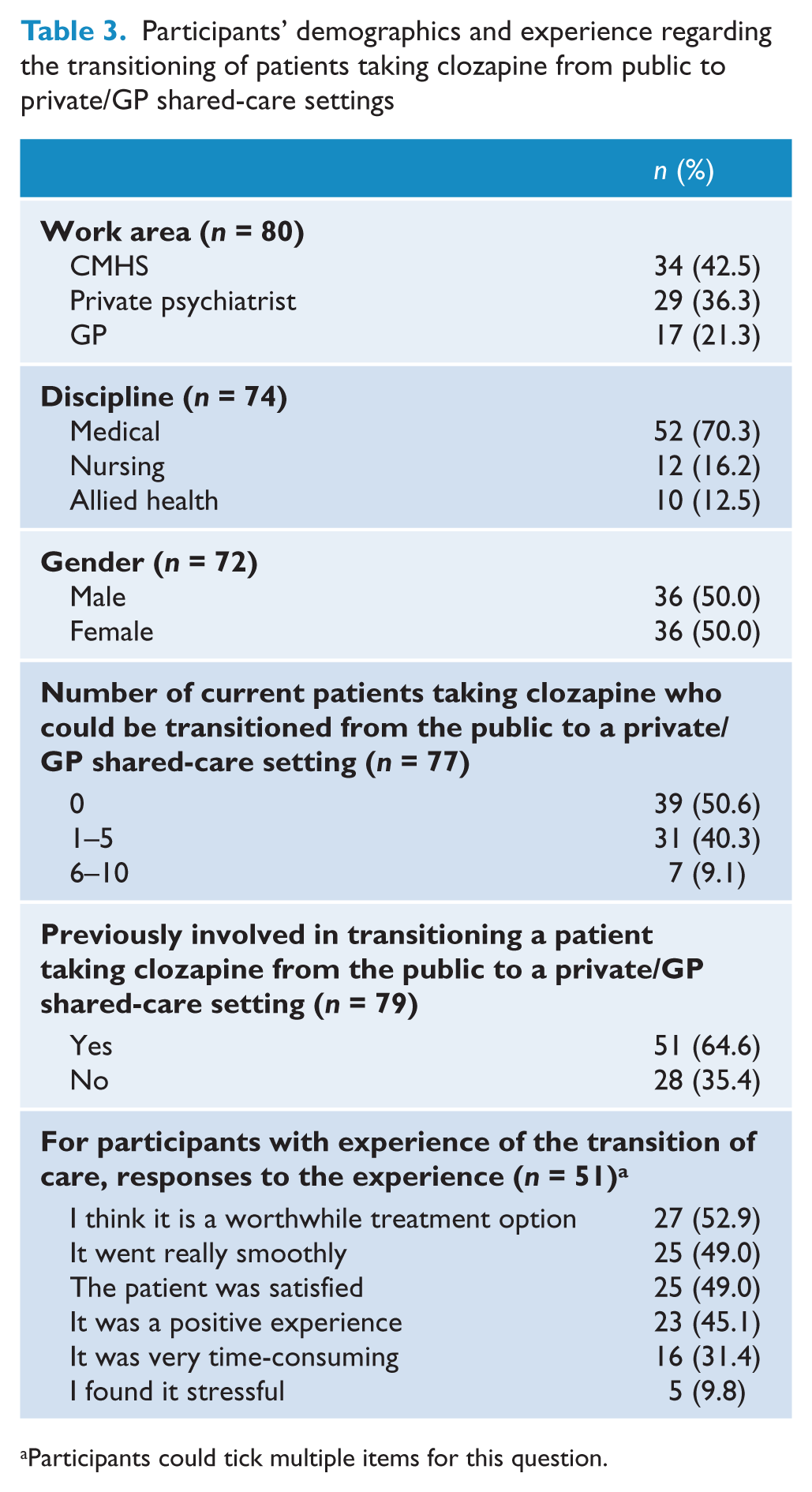
Participants could tick multiple items for this question.
Barriers to transitioning
Of the 14 barriers on the CTQ, the five most significant in order were:
Patient having a low level of personal organizational skills;
Patient having ongoing case management needs;
Less patient accountability in the private/GP setting;
The cost of the private service;
Patient’s level of medical compliance.
Generally, participants rated the impact of most barriers similarly. However, the three groups differed significantly for cost, patient medication compliance, and ongoing case management needs (see Table 1). Specifically, GPs rated the cost of the private service as significantly less of a barrier to transitioning than CMHS staff (Scheffé’s test, p < 0.0005) and private psychiatrists (Scheffé’s test, p = 0.001). GPs also rated ongoing case management needs significantly less of a barrier than CMHS staff (Scheffé’s test, p = 0.03) and private psychiatrists (Scheffé’s test, p = 0.006), and ongoing medical treatment compliance was significantly less of a barrier for GPs than CMHS staff (Scheffé’s test, p = 0.04).
The following additional barriers were provided by participants (number of respondents in parentheses):
The process of transitioning a patient is too time-consuming (4);
There is a lack of information available about the transition process (2);
There is a lack of support from the GP/private psychiatry sector (2);
There is a lack of support from the public CMHS – this includes access to mental health services for review and the public service being unwilling to take back patients if issues arise (6);
Amount of paperwork that needs to be completed (2);
Being able to establish a therapeutic relationship with the patient (3);
Patient not having health insurance (1);
Side-effects of clozapine (1);
Obtaining approval for scripts and blood tests for patients to go on holidays (1).
Criteria for transitioning
Of the 12 criteria (see Table 2), participants rated the five most important in order as:
Compliant with medication;
Attends appointments and blood tests independently;
Can access a suitable pharmacy for their medication;
Is happy to be treated privately;
Is physically able to get to the private service.
Primarily ratings were consistent across the groups, however, staff from the CMHS (Scheffé’s test, p = 0.001) and the private psychiatrists (Scheffé’s test, p = 0.005) thought it was significantly more important that the patient is able to independently attend appointments and blood tests than did GPs. CMHS staff rated that it is significantly more important that a patient has low case management needs before they are transitioned than did the private psychiatrists (Scheffé’s test, p = 0.013) or GPs (Scheffé’s test, p < 0.0005).
The following additional transitioning criteria were listed (number of respondents in parentheses):
Support from the public system is available if the patient deteriorates (2);
There is no substance abuse (1);
The patient can afford the change to treatment (1).
Discussion
This study explored staff perceptions of the barriers and criteria for transitioning patients taking clozapine from public to private/GP shared psychiatric care, to help inform the management of this often complex population. Staff from a public CMHS, private psychiatrists, and GPs rated the following as the most significant transition barriers:
Patient having a low level of personal organizational skills;
Patient having ongoing case management needs;
Less patient accountability in the private/GP setting;
Cost of the private service;
Patient’s level of medical compliance.
The most important criteria for effectively transitioning patients were:
Compliant with medication;
Attends appointments and blood tests independently;
Can access a suitable pharmacy for their medication;
Is happy to be treated privately;
Is physically able to get to the private service.
Ranked criteria in the present study support those suggested by Castle et al. (2006) who proposed that patients suitable for a GP shared-care arrangement are psychiatrically stable, compliant with medication and blood testing regimes, have stable accommodation, and are readily contactable. For the optimization and success of a clozapine transitioning programme, addressing these barriers and preparing patients to meet the criteria is critical to successfully transition patients taking clozapine into less intensive mental health care.
The experience of Alfred psychiatry has been that having a clozapine coordinator on staff has significantly contributed to addressing these barriers. They assist with registration and completion of paperwork (a time-consuming component of care), and play a significant role in identifying, preparing, monitoring, and supporting suitable patients taking clozapine able to transition from the public to private/GP shared-care setting. Clozapine coordinators also act as contacts for patients for a designated period once they have transitioned (e.g. 12 months).
In practice, clozapine coordinators also become the first contact for GPs/private psychiatrists. A relationship is established that enables a rapid consultation response supported by a shared understanding of the patient, and can facilitate improved re-entry into the public CMHS if the patient deteriorates. Six respondents expressed on the CTQ that a lack of support from the CMHS following discharge could complicate provision of care if issues arose. Previous research has shown that approximately 52% of patients undergoing a planned discharge from case management re-present to the mental health service within 12 months (Backus et al., 2008). In the event of transitioned patients experiencing deterioration, a clozapine coordinator that was known to the patient and GP or private psychiatrist and following clinical guidelines that outlined pathways to re-entry, can improve re-engagement with public CMHS care.
In this study, GPs were significantly less likely than staff from the CMHS and private psychiatrists to think that cost and ongoing case management needs were barriers that impacted on the transition process. Perhaps GPs are accustomed to working with some of the more diversely complex patients on a regular basis. GPs are well placed to participate in a shared-care programme for patients taking clozapine, providing they receive adequate education and support, and are able to bulk bill such patients.
Private psychiatrists can also successfully manage suitable patients taking clozapine, but probably need greater incentive to do so. Due to the nature and structure of their practice, private psychiatrists may require greater support from, and access to, the public CMHS. It would be ideal for a private psychiatrist managing patients taking clozapine to work within a service that employs a clozapine coordinator or practice nurse to continue addressing many of the identified logistical barriers (e.g. reminders to attend blood tests, appointments, and support in locating and accessing an appropriate pharmacy). It is also important that private psychiatrists who manage patients taking clozapine are able to bulk bill.
Clozapine coordinators can also play a key role in working alongside fellow CMHS staff to identify, prepare, and initiate the transition of public patients under their care into private/GP shared-care arrangements. Historically, patients taking clozapine require long-term CMHS case management. With the clozapine coordinator able to facilitate the registration process for transitioning, and provide additional consultation and monitoring of the patient beyond the transition occurring, this may encourage public CMHS staff to use this as an opportunity to step patients down into a less intensive level of care.
Clinicians that had been involved in transitioning patients taking clozapine reported both positive and negative aspects to the experience. Refining the process of transitioning, for example, using information from this study to address the most significant barriers and refine the criteria for transitioning, will serve to improve the practice, and consequently the experience of staff involved. Staff need to be adequately trained, supervised, and supported during the process of transitioning patients taking clozapine, again something that a dedicated clozapine coordinator can provide.
This paper describes one study from a larger project. There are two other parts underway that together will provide a comprehensive evaluation of the entire clozapine transitioning model of care. One is a comprehensive audit of 90 patient files (30 transitioned to private psychiatrists, 30 transitioned to GP shared care, and 30 remaining with the public CMHS) for the 12-month period before and the 12-month period after transitioning. This will provide detailed information about the type of patient that is selected for transitioning and what actually happens once they are transitioned. The other study is exploring the patient perspectives of being involved in transitioning, to ensure that the experiences of patients directly affected can contribute to reviewing the effectiveness of the transitioning model.
There are some limitations to the present study. The response rate of below 50% provided a smaller sample than was anticipated. The results represent the views of staff in a certain geographical area, which has a clozapine coordinator and established GP shared-care programme. These views may not accurately represent those of staff working in other services, so a replication of this study in other regions may provide an indication of study generalizability. A final limitation was that the perspective of patients actually involved in the transitioning process was not taken into consideration. It is expected that the qualitative data obtained from patients in the other parts of the larger project will address this limitation.
In conclusion, while numerous barriers and criteria need to be considered and addressed prior to changing a clozapine patient’s model of care, transitioning patients from the public to private/GP shared-care setting is a viable and worthwhile treatment approach. The experience of staff involved in the transition programme has been positive, with benefits for staff and patients. This has highlighted a real possibility for expanding shared-care arrangements for complex psychiatric patients to build bridges between primary and psychiatric clinicians to enhance patient care.
Footnotes
Acknowledgements
We would like to thank the participants involved in this study and the services they work within.
Funding
This work was supported by a grant from HOSPIRA Australia.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.