
Abstract
Objective
The process of detecting people at high risk of schizophrenia from a community sample is a major challenge for prevention of psychotic disorders. The aim of this paper is to describe early detection procedures that can be implemented in primary care settings.
Methods
A selected literature review is supplemented by experiences and data obtained during the Buckingham Integrated Mental Health Care Project.
Results
General medical practitioners have been favoured as the agents most likely to prove helpful in detecting the key risk factors that predict the onset of schizophrenic disorders, as well as in recognising the earliest signs and symptoms of these conditions. However, the practical problems of screening for multiple and subtle risk factors in general practice are substantial, and general practitioners (GPs) often have difficulty recognising the earliest signs of a psychotic episode. A range of strategies to assist GPs detect early signs of psychosis in their patients are considered.
Conclusions
It is feasible to implement primary care setting early detection procedures for people at risk of schizophrenia. Implementation is aided by the use of a brief screening questionnaire, training sessions and case supervision; and increased collaboration with mental health services and other community agencies.
The process of detecting people at high risk of schizophrenia from a community sample is a major challenge for prevention of psychotic disorders. Schools and general medical practice are among the agencies that could provide effective screening. Almost all people living in a community are examined by these agencies over prolonged periods of high incidence to these disorders. Whereas schools and colleges of higher education observe cognitive and psychosocial development and dysfunction in young people, they have a limited ability to screen adults. Thus, general medical practitioners have been favoured as the agents most likely to prove helpful in detecting the key risk factors that predict the onset of schizophrenic disorders, as well as in recognising the earliest signs and symptoms of these conditions. My experience of several years of working as a general practitioner (GP), as well as, more recently, developing specialist mental health services in close partnership with GPs, may enable me to provide some useful practical comments [1].
First, two key issues are whether the average GP has the capacity to detect high-risk cases without the sophisticated assessments used in specialised psychiatric practice [2]. Second, whether GPs are capable of recognising consistently the early signs of psychosis.
Detection of persons with high risk of developing schizophrenic disorders
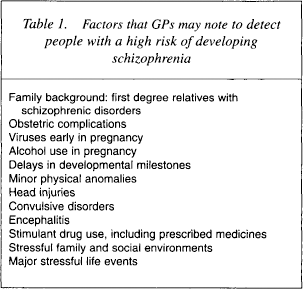
Table 1 lists some of the factors that have been considered potential indicators of a high risk of developing a psychotic disorder [3]. It is possible that if we were able to detect combinations of these factors in people attending general medical practices, we may be able to devise strategies to reduce this risk, or at least to monitor closely such people in order to detect the earliest signs of the onset of psychoses.
Factors that GPs may note to detect people with a high risk of developing schizophrenia
But how realistic is it to expect GPs to be able to collaborate in this risk assessment? First, let us examine some of the points that GPs might consider when they are faced with a psychiatrist asking them the following question: ‘Can you help us screen your patients to detect those people who might have a high risk of developing a schizophrenic disorder?’
Usually, GPs will have information about the family background of most of their patients but it may not always be well recorded in their records. A GP who has treated a family for several years will have gathered considerable information about the genetics of that family as well as the cultural and social environment that may contribute to the way in which any genetic vulnerability presents (i.e. both the genotype and phenotype). Birth records and developmental milestones may be recorded as well as details of accidents resulting in head injuries and concussion. Prenatal viral infections are more likely to be recorded in the mother's records. Neuroviral infections of the patient such as meningitis and encephalitis, as well as high fevers and convulsions, are noted. Minor physical abnormalities and neurological soft signs may be detected and recognised by astute GPs, but may be more evident to schoolteachers.
Other environmental risk factors may be less well recognised. Alcohol and drug abuse is not easy to screen as a GP. Stress factors may also be something that many GPs are aware of in their patients, but not usually recorded in the case notes.
A further difficulty faced by GPs is that many major mental illnesses present initially with physical rather than psychological symptoms. This is not only true of depressive and anxiety states, but also many cases of psychosis present with physical discomfort that may lead a person to go and seek help from their GP for that symptom, often contributing to a delayed diagnosis.
As a consequence, although there is a substantial store of knowledge about potential risk factors for schizophrenic disorders within the ambit of general practice, this is seldom well systematised and recorded in a clear manner that could readily aid the early detection of persons at risk for psychosis. For this reason the practical problems of screening for multiple and subtle risk factors in general practice are substantial. Despite the difficulty in formalising recognition of risk factors, it is possible that effective primary health-care practice, including improved prevention and treatment of infectious diseases, particularly the neuroviruses, as well as enhanced obstetric procedures may already be contributing to the reduced incidence of psychotic disorders reported in several countries with well-developed general practice services [4–8].
Recognition of the early signs of psychosis
General practitioners have difficulty recognising clearly the earliest signs of a psychotic episode. However, patients or their family members often seek advice from their GPs at this stage. Patients, family members and friends and GPs all usually realise that ‘something is not quite right’ with the person's psychological and social functioning. In my experience, efforts to formalise this process of detection with the use of simple checklists of prodromal signs and symptoms has met with limited success. Attempts to introduce more detailed early signs questionnaires [9,10] have been considered unfeasible. Nevertheless, most GPs find it useful to have a list of the main signs and symptoms readily at hand to alert them that ‘something is not quite right’ and to seek further consultation about that case without delay.
Screening for the characteristic symptoms of florid psychosis is not difficult for most GPs [11]. However, they do not always recognise the onset of deficit symptoms and psychosocial deterioration of patients with a more gradual onset. These may be mistaken as symptoms of anxiety and depression, or adolescent crises. We have devised a screening questionnaire, the 10 Question Screening (10QS), with questions which we suggest that GPs use as a brief mental status exam for patients they suspect of having symptoms of any major mental disorder (Table 2) [12]. Examples of these questions include:
Ten question screening – 10QS
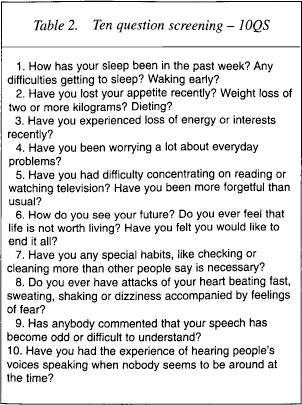
Sleep problems. These are among the best early signs of many serious mental disorders. Primary insomnia is very rare. However, persistently disturbed sleep is usually a symptom of a mental disorder, including schizophrenia and bipolar disorder, as well as depression and anxiety. So, if a busy GP can only ask one question to screen for major mental disorders, a check on the person's sleep patterns would detect most cases.
Appetite loss. This is usually a sign of depression, but a large proportion of cases of psychosis present with symptoms similar to depression – loss of energy, loss of interest and motivation, excessive worrying about everyday problems or concentration and attention difficulties.
Thoughts of suicide. These are important whatever the underlying disturbances, and it is important that GPs can learn to ask the sorts of questions that help bring out clear responses about this issue.
Specific psychotic signs and symptoms. The 10QS includes other questions that concern specific symptoms of psychosis. Most of these are included in early signs questionnaires. Unusual speech is often something that family members or teachers will comment on, but may be too subtle for a GP to detect in an interview. And of course the experience of hearing voices is a key symptom of established early psychosis.
With the aid of a brief screening questionnaire, such as the 10QS [12], it is feasible to train GPs to screen for established early symptoms of episodes of mental disorders. These methods may lead to more cases receiving effective treatment earlier in the course of the disorder, reductions in suicide, and a lower rate of inappropriate referrals to specialist psychiatric clinics. In our experience it has been more helpful to assist GPs to detect all forms of major disorders, including anxiety and depressive syndromes, not merely to restrict our focus on early detection of the relatively rare presentations of psychotic disorders.
Strategies to improve collaboration between primary care and specialist mental health services
There are several models of collaboration between the Specialist Mental Health Services and the Primary Care Services (Table 3) [1]. One is the District Nursing Model where mental health nurses work in general practice. This model has been used extensively in the United Kingdom. Another model is the relocated Outpatient Clinic approach. The traditional Outpatient Clinic located in a hospital or Community Mental Health Centre is relocated to one or more general practices, preferably health centres where several GPs are located. This increases the accessibility and reduces the potential for stigma. These clinics are not restricted to psychiatrists. Psychologists and social workers may also base their clinical work in general practice. All of these relocated clinics, as well as the associated mental health nurses, tend to be staffed by individual specialists who often lack effective backup consultation and support from a multidisciplinary team.
Models of collaboration
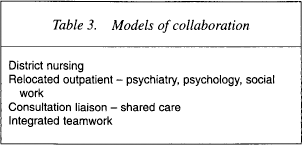
Another approach is the ‘shared care’ model that is very similar to consultation–liaison services in hospitals. The level of sharing can vary considerably. It can involve the consultant visiting and giving an opinion on cases that are presented by the GPs. The psychotherapeutic approach of Michael Balint has often been used in this way [13]. Alternatively, it can involve joint decision making following individual consultations with the patient.
The final approach is one that we developed in the program established in the United Kingdom in Buckingham in the early 1980s, which we called ‘Integrated Mental Health Care’. We took an entire comprehensive mental health team and located them all in the general practices in the area. The functions of mental health outpatient, day patient and most inpatient services were conducted in full collaboration with the GPs and their primary care teams. Administrative and clinical personnel were shared, as well as premises and records. This approach enabled detection of high-risk cases, early recognition of symptoms and signs of major mental disorders, and continued bilateral training and development of primary and specialist teamwork in a mutually satisfying way [1].
In order to collaborate effectively with primary care services, we need to choose the model that will fit best with local resources and limitations. In the absence of research on this issue, there is no evidence to suggest that one method is better than another. However, daily contact between GPs with mental health specialists who are competent at assessing high risk factors as well as recognising early cases appears to be essential for successful prevention.
Training general practitioners in detection of high-risk factors and early cases
Table 4 summarises some strategies that have been used to train GPs. In our experience formal training in lectures, seminars and workshops is not useful. This conclusion was validated by a survey we conducted with GPs in Buckingham who, without exception, endorsed an informal approach where they can discuss difficult cases and present their own ideas and experiences with experts without fear of appearing ignorant of the niceties of diagnostic formulations and technical jargon. This approach seems similar to that used successfully by pharmaceutical companies.
Training GPs to detect high-risk factors and early cases
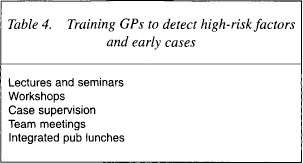
In the Buckingham Project, this informal case supervision was not done only by psychiatrists, but more usually by the key workers of the cases, who included nurse specialists, social workers, occupational therapists or psychologists. Specialist supervision on pharmacological or neuropsychiatric problems usually involved the team psychiatrist. In the same manner, a complex problem with housing or finances would generally involve discussion with the team social worker. This supervision was undertaken on an ‘as needed’ basis, and averaged 20 minutes weekly. In addition, we encouraged each GP to attend the team meetings that were held weekly in their practice offices at the end of their morning consulting. However, attendance was poor as they seldom finished consultation within the allotted time or they would have to manage an emergency or serious problem. So, even with the best intentions, it was difficult for them to regularly attend these team meetings/When they did, the experience was usually mutually rewarding.
We discovered that some of the best training opportunities were even more informal. For example, a group of GPs would organise lunch with pharmaceutical representatives every Friday for video presentations and a discussion about new pharmacotherapy. Another group met on Monday evenings at a local pub. In both these situations interesting discussions about problem cases occurred.
Given these considerations, efforts to train GPs with formal lectures and workshops seem to be of limited benefit. A more creative approach may work better. The need for a relaxed nonthreatening environment, where learning can be a mutual and a rewarding experience is strongly advocated.
Liaison with other community agencies
The provision of services in a community-based manner provides opportunities for informal liaison not only with general medical practitioners, but also with other community agencies (Table 5). Foremost among these are the schools. Schoolteachers are often very stressed and consult frequently with primary care services. They appeared highly receptive to consultations about their personal mental health problems and appeared eager to apply similar stress management strategies with their pupils. In this manner liaison with the schools and university developed in a simple and effective way.
Other community agencies that may assist in early detection
In addition to discussions with teachers about students who appeared to be suffering prodromes of mental disorders, we began to develop an education program for the schools [14]. This program consists of education about mental disorders that is targeted to age-specific issues throughout each of the 5 years of the UK high school curriculum. For example, in early adolescence we deal with eating problems and anxiety, while at a later stage psychotic and suicidal problems are targeted. In addition, students learn practical interpersonal communication and problem solving skills that they can apply to their personal goals and problems both in the classroom and in their relationships. Pilot applications have been very promising and have suggested that they may contribute to early intervention and possible prevention of serious mental health problems such as suicide and untreated psychosis. However, controlled trials are essential before we can advocate wider use of this approach.
Another important group to educate is the police and justice system. They generally have very little, if any, training in such matters as mental health. It may be helpful for them to have some understanding about early psychosis as well as how to manage someone who might be a high suicide risk. Training in the use of the 10QS was useful together with close collaboration and liaison on a case-by-case basis. Liaison with lawyers who deal with major family crises, abuse problems and marriage break-ups can also be very helpful in a community-based approach to stress management and detection of early cases of major disorders.
Collaboration with the social services is usually taken for granted but often is rather difficult because of the different models we follow. For example, we found that social service workers often loathe to ask somebody about psychotic experiences or suicide plans because they had been taught to be nondirective and to wait empathically until the person divulged such information. Despite training in sensitive yet structured psychiatric interviewing methods, most social service colleagues remained reluctant to use such direct questioning.
Another area where prevention and early intervention may prove effective is the antenatal program. Education about mental disorders at this critical time in family life may have a considerable and lifelong impact. This is in addition to the benefits of improved antenatal care on the reduction of birth injuries that may contribute to a reduced vulnerability to psychotic disorders. We developed a program in collaboration with obstetric nurses to educate pregnant women and their partners about mental disorders and stress management. This was conducted in conjunction with antenatal classes in all of the general practices and proved very popular. Postnatal psychosis and depression appeared to be detected early and managed with minimal difficulty. Once again, controlled studies are needed to validate our observations.
Consultation with cultural groups is another very important issue for the prevention and early intervention of mental disorders. The early signs, problems and risk factors might be quite different within culturally diverse groups (e.g. Aboriginals and Maori/Pacific Islanders). It is important to understand cultural phenomena and the way in which people express their stress problems and mental disorders and seek help. Ideas that may sound like delusions or hallucinations to a European, may be expressions of anxiety, depression or stress in other cultures. We have found that working closely with the person's family helps clarify many of these issues.
Conclusion
Prevention of mental disorders necessitates close collaboration with a variety of community agencies. In addition to liaison with primary health care teams, consultation and education with schools and universities, police and lawyers, antenatal programs and cultural groups is advocated. The methods used need to be mutually rewarding, effective and efficient. Successful pilot work has been conducted, but controlled studies are urgently needed before widespread application of these approaches can be advocated.