
Abstract
Objective
To provide a historic context for developing a framework for preventive mental health research in Australia.
Method
A literature review was undertaken and references were selected for their relevance to describing the contributions of Australian researchers and clinicians to an epidemiological approach to mental health disorders, particularly schizophrenia.
Results
Australian researchers and clinicians have made major innovative contributions to preventive mental health research.
Conclusions
Australian mental health services, in collaboration with academic departments, are in a highly favourable position to expand preventive research activities into schizophrenia.
There has been substantial interest in and commitment to prevention in psychiatry over recent decades. The first wave of the community mental health movement, exemplified in the work of Gerald Caplan, situated prevention as an important component of what could be achieved by community psychiatry. Caplan's classic volume, Principles of Preventive Psychiatry, published in 1964, focused on the opportunities for positive outcomes of life and developmental crises, which were seen by Caplan as times of disruption, stress and adaptation [1]. Crisis intervention was the centrepiece of prevention. Prevention was described as: (i) primary (prevention of onset or incidence of new cases); (ii) secondary (prevention of prolonged illness, i.e. decreasing prevalence); and (iii) tertiary (prevention of associated disabilities). The crisis intervention focus arose from work such as that of Eric Lindeman with intervention for acutely bereaved people following the Coconut Grove nightclub fire.
Caplan's theoretical constructs were attractive and offered opportunity for relatively brief and focused programs that might lessen the extent and suffering of mental disorders. It was also a ‘normalistic’ model in that its focus was positive and not orientated to a specific disorder. Prevention was seen to occur through lessening risk of poor crisis resolution, which was theorised to create general psychiatric vulnerabilities. In fact, this model was not unlike the earlier mental hygiene movement, which proposed parenting and child management as potentially creating the mentally healthy child – although it must be acknowledged that there was little focus on specific childhood psychiatric disorders per se.
This first wave of prevention in mental health lacked an empirical basis when Caplan published his work. Research studies to test this model were first carried out in systematic ways by Australian researchers, led initially by Maddison and Walker through their studies of the crisis of conjugal bereavement [2]. Testing of preventive intervention for those at high risk of poor resolution through identified risk factors, such as lack of social support, established the capacity of such interventions to significantly decrease the risk of general psychological morbidity [3]. This fitted clearly with the Caplan model of targetting only those at high risk of adverse outcomes, with expectancies of healthy or even improved adaptation in the remainder. Research studies with the crises of accidental injury [4] and injury and illness [5] provided further evidence of the effectiveness of such techniques in reducing psychiatric symptomatology in high-risk groups. This work was theoretically and methodologically relatively simple, and did not take into account either the epidemiology of specific disorders nor the capacity to prevent them, although there are some trends of decreased depressive symptomatology.
There was a refocusing of community mental health and mental health services generally in the ensuing years. Chiefly it would appear because the very broad promise of the initial movement had not been met and the needs of those with more severe, frequently psychotic illnesses were pushed to the forefront with deinstitutionalisation.
Nevertheless, research studies continued to develop further in this field through special research initiatives in the United States (e.g. early 1980s with targetted prevention funding). Within Australia there was further development of epidemiological studies, which were increasingly seen as a critical basis for planning prevention programs in the general health field, and could potentially have been so in the psychiatric field. There were, however, substantial barriers and a profound belief that prevention was pointless in mental health, because, for instance, the cause of the onset of schizophrenia was not known. Conceptualisation and marshalling of available evidence did little to further commitment, except in a few Australian centres [6].
The growing importance of psychiatric epidemiology, as well as the rapid expansion of research in psychiatry, including studies of aetiology. and course and treatment of disorders, was complemented by an accumulating body of work relevant to prevention. Again, this was generic in nature. However, this was also in keeping with a developing recognition of the multifactorial aetiology of most psychiatric disorders, and the generic nature of many risk factors, as was also the case of physical illnesses (e.g. obesity, physical inactivity, smoking, excess alcohol intake).
A number of reviews advocating prevention in mental health appeared from 1989 onwards and have been significant in the development of present policies and programs in this field. They include the Australian National Health and Medical Research Council (NHMRC) report Scope for Prevention in Mental Health [7]; the United Kingdom report Prevention in Psychiatry [8]; and the highly influential Institute of Medicine report Reducing Risks for Mental Disorders [9]. Numerous other volumes, research studies, reviews, journals and conferences have taken place and further drive this field [10–12].
A further critical development that has given momentum to the need for prevention in mental health is the publication of The Global Burden of Disease report by Murray and Lopez in 1996 [13]. This highlighted for the first time the extent of disability associated with mental disorders, and the health impact in terms of the new measure DALYS (disability-adjusted life-years lost through illness). Five of the ‘top ten’ causes of disability were identified as mental illnesses, including substance use disorders. This burden was growing with projections that unipolar depression alone would be the second leading cause of such burden by the year 2020. Australian studies examining the Australian burden of disease will be discussed later, but support this very high health impact of mental disorders [14]. These findings have made it clear that treating disorders is not enough and prevention must also occur; it is both feasible and effective, although the political will to commit to it is more difficult, as Eisenberg has outlined [15].
In the context of the Australian National Mental Health Policy, prevention and promotion were identified as a core element in 1993, but not included as specific programs in the First National Mental Health Plan where reform focused on orientation of services to the community and to general hospitals. The Second National Mental Health Plan (1998–2003) recognised both the global burden of disease, and the growing evidence-base for prevention; one of its three key platforms is that of health promotion, prevention and early intervention.
Substantial and ongoing Australian research has contributed to the evidence-base of prevention and is also contributing to programs being set in place across Australia, principally in the area of Child and Adolescent Mental Health. These studies are exemplified by those for the prevention of conduct disorder [16]; for the prevention of anxiety disorders [17]; and for the prevention of depression [18]. Many other Australian programs are also in place.
Building on these and international findings, the Mental Health Promotion and Prevention National Action Plan (1998) was drawn up and set in place by the Commonwealth, under the National Mental Health Strategy, in partnership with the National Public Health Partnership and with Australia-wide consultation [19]. This plan deals with priority target groups across the lifespan, priority population groups, and key strategic priority groups. It sets priority mental health targets; identifies the rationale and evidence-base for prevention for each of the above groups; suggests research questions; and proposes national strategies. Communities of interest, settings for intervention, and linked initiatives are described. Process outcomes and longer-term outcomes are identified. This plan has been the basis for National developments, such as scoping studies of perinatal mental health and prevention; and children of parents with mental illness and prevention. In addition, it has formed a basis for states and territories to take forward their activities for promotion and prevention under the Second National Mental Health Plan. This plan is currently being updated to include early intervention; that is, Promotion, Prevention and Early Intervention in Mental Health, and a monograph with supporting evidence and conceptualisation will also shortly be released.
The conceptual basis for prevention in the National Mental Health Policy, and the Promotion and Prevention Action Plan and now Early Intervention Action Plan rests on the Mrazek and Haggerty model of a spectrum of interventions as developed in Fig. 1 [9].
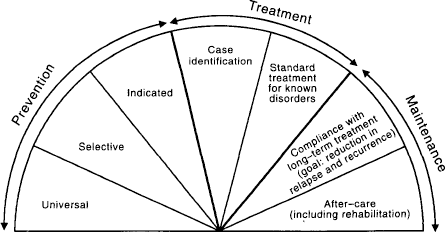
The mental health intervention spectrum for mental disorders.
Furthermore, Mrazek and Haggerty have identified the core sciences that will contribute to the understanding necessary for prevention, neuroscience, genetics, epidemiology and developmental psychopathology. Prevention in mental health does not, however, have to await the full elucidation of these as they contribute to specific conditions – and it does not do so in the physical health field.
This model for prevention is situated in a population health approach to mental health [20]. This melding of prevention into a population mental health framework alongside clinical or personal health services provides the capacity to identify, or the basis of epidemiology and related sciences, how the disease burden may best be impacted upon; that is, what are the ‘best buys’ to achieve decreased incidence, prevalence and disability associated with disorder, using the best available evidence of effective interventions? As described by Offord and coworkers, interventions across the full spectrum are likely to be needed to impact on disease burden [21], although some may hold greater opportunity for benefit than others (e.g. preventive interventions for conduct disorder).
Indicators have also been developed to monitor and evaluate program effectiveness both for individual programs and more broadly [22]. There is still the issue of how the research findings of preventive intervention (there are now over 1000 controlled trials) translate into effective program delivery. This involves, as Hosman and Engels have ably researched and described, keeping fidelity to principles in terms of what is effective, while ensuring relevance, feasibility and adaptability to local settings [23]. Ensuring the information systems to measure and monitor outcomes, to evaluate program effectiveness is critical, as is the cycle of research and evaluation.
Implications for schizophrenia
There has been a long-term interest in what might be done to ‘prevent’ schizophrenia, although little in the way of findings in terms of effective interventions. This is partly due to pervasive negative views about outcomes and a growing recognition of the multifactorial and, as yet, not clearly defined, factors that might contribute to onset and course of this illness. As noted by McGorry and Singh, barriers include: (i) views such as that of schizophrenia as an immutable and disabling brain disorder; (ii) the failure to recognise and address the burden of schizophrenia in a public health framework; (iii) pessimistic attitudes about the disease and its outcomes; and (iv) marginalisation of those affected [24]. They considered, then, that ‘harnessing existing knowledge now around the preventive paradigm would be a worthwhile and achievable objective’ (p. 491).
Potential for prevention with the schizophrenia syndrome will now be considered broadly, both in terms of the current understandings in the core science domains, and in terms of the evidence-base of effective interventions across the spectrum and the lifespan. This review will be illustrative rather than comprehensive.
Epidemiology and schizophrenia
Prevalence rates of psychosis more generally, and schizophrenia in particular, have now been established in a wide range of international studies with an estimated annual incidence between 0.1 and 0.5%. The lifetime risk of schizophrenia is generally considered to be 1%, with onset usually in the later adolescent to early adult years for men and later (5 years or so) for women. It has a long prodromal period and the duration of untreated psychosis (DUP) may be long, often more than 2 years, contributing to poorer outcomes [25]. Regardless of whether the lifetime risk is 1% or slightly higher, as some studies suggest [26], there are critical issues impacting on such a relatively rare condition by any population-based approach; for instance, a universal intervention program. Such an intervention would be difficult to target but, in addition, the potential to impact on such relatively low prevalence would make it difficult to demonstrate successful prevention in statistical terms.
When epidemiological studies examine risk factors, relative risk (RR) and population attributable risk (PAR) are key concepts to determine the potential for an intervention to produce benefit. In a Danish population study, Mortensen et al. confirmed that a family history of a parent or sibling with schizophrenia conveyed the greatest risk (RR = 9.31 for a mother with schizophrenia, 7.20 for a father with schizophrenia, 6.99 for a sibling with schizophrenia) [27]. Urbanisation of place of birth conferred higher risk than rural (2.40 for being born in Copenhagen compared to rural) and month of birth (February to March R.R = 1.1). When these are examined in terms of the population, however, the PAR changes the potential for impact of an intervention. It is 5.5% for a family history of schizophrenia; 34.6% for an urban place of birth; and 10.5% for season of birth (winter months). It is noted this latter season of birth is variously depicted as potentially due to viral infections in the winter months.
Thus to impact, one would need to address place of birth, but of course this is not possible – unless one provided advice on this to those already vulnerable. Nor is it likely that one can significantly influence season of birth. Thus, universal programs built on the epidemiology of schizophrenia are not only difficult to theorise but likely to be impossible to enact. Added to these findings are social determinants such as adverse socioeconomic status.
Nevertheless, as highlighted through the study of genetic epidemiology in twin cohorts [26], while 83% of the variance in liability to schizophrenia is accounted for by additive genetic factors, 17% may be caused by environmental factors that were not shared. This might include, for instance, obstetrics complications. What is highlighted by these epidemiological findings, then, is that environmental factors that are open to influence play some role in the aetiology of schizophrenia and therefore offer some opportunity for prevention. But to demonstrate the effectiveness of any such intervention it may be necessary to target those at heightened risk.
Genetics
As indicated earlier it is clear from a range of studies that genetics play a significant part in the vulnerability to schizophrenia. But the heightened risk in offspring does not mean that most people with schizophrenia have a relative with the disorder. In fact the majority of people who develop the illness do not have a relative with the condition. Risk is said to be increased, overall, ten-fold but, nevertheless, the model that appears to hold most evidence in terms of current research findings is that of varying levels of genetic vulnerability, coupled with environmental and psychosocial stressors [28]. This is often called the diathesis-stress model. This has been drawn together in neurodevelopment theories of schizophrenia, reflecting the interaction of these vulnerabilities and stressors [29]. Recently, however, this model has been challenged [30] and considered as being inadequate in terms of explanatory processes because of the number of other variables increasingly understood.
Thus, interventions utilising an understanding of genetic or familial vulnerability are theoretically possible. However, the genes responsible have not yet been identified, with the current consensus being that multiple genes are responsible [31,32]. Intervention may include genetic counselling, with all the inherent ethical issues, and specific programs for those likely to be more genetically vulnerable with respect to protective regimens to deal with environmental or psychosocial stressors. Of course such stressors need to be further clarified, but these have been reported to include perinatal complications [33] and influenza, or other viral exposure of the fetus during the winter months, or adversity such as famine. Protecting the fetus is inherently positive with potential benefits for other more prevalent and also disabling disorders, and preventing birth complications is also a generically positive intervention. Both should be mounted, but whether these can impact on the incidence and prevalence of schizophrenia in those vulnerable would be extremely difficult to establish. Such types of interventions, however, might be seen as selective prevention programs directed towards populations at higher risk, within the population as a whole.
Neurosciences
There has been a great focus on and extensive research attempting to establish the neuroscience of schizophrenia. Findings have included enlarged ventricular size; decreased cortical size; and unusual cortical laterality with dysfunction localising to the left hemisphere [34]. Anatomical abnormalities may be reflected in changes demonstrated in functional studies such as magnetic resonance imaging and positron emission tomography. These abnormalities may correlate with positive symptoms with, for instance, temporal lobe dysfunction related to abnormal phospholipid metabolism [35]. Disorganised speech has been found to be associated with abnormalities in regions of the brain dealing with speech. And negative and cognitive symptoms are commonly associated with prefrontal lobe dysfunction [36]. However, these findings vary, with some studies showing similar deficits in subjects without schizophrenia [30]. As noted in the Surgeon General's Report, such brain mapping is complex and variable (p. 277) and recent work suggests that dysfunctions are more likely to be in circuitry than in one or two localised areas of the brain [37,38].
The neurochemistry of schizophrenia is also of great relevance with excessive levels of dopamine being implicated, although it is not clear whether this is a primary causal or a secondary factor. Indeed, there are suggestions of greater complexity in the dysregulation of dopamine and other neurotransmittor systems, and variations in dopamine receptors [39] or serotonin systems [40]. New models of such pathopsychology of schizophrenia, which indicate the need to clarify directions and significance of any such findings in terms of the aetiology of the disorder, have been suggested.
With respect to opportunities for prevention building on neuroscience, these are, to date, limited both in terms of inadequate theoretical and scientific basis, or contributions to aetiology and potential for influence. These findings are at the present time most relevant for prevention in the stress-diathesis model or, with respect to impact on the course of the illness, through early and effective treatment and relapse prevention.
Developmental psychopathology
The development of schizophrenia over time has been the subject of a number of high-risk cohort studies, which attempt to provide an understanding of disorder evolution, the modifying factors, and how these could potentially be influenced by preventive interventions.
Stressors are principally hypothesised as operating on this developmental pathway, and being amenable to intervention at points of influence, taken particularly in a neurodevelopmental context. Such stressors include biological, environmental, psychological and social factors.
Exposure of the fetus to adverse environmental influence (e.g poor maternal nutrition, such as in the Dutch War famine [41], or mid-trimester maternal influenza during the winter months [42]) are suggested stressors, although these findings are also debated. Similarly, with respect to perinatal complications, these may be causative of neurodevelopmental problems or even the result of these. How these environmental stressors may impact to increase neurodevelopmental vulnerabilities to schizophrenia, either during the intrauterine period or subsequently, remains to be established.
Cohort studies of schizophrenia with high-risk offspring of schizophrenic parents have been carried out by a number of workers, and findings from these studies were reviewed by Asarnow in 1988 and highlight neurodevelopmental impairments and higher rates of maladjustment in such children [43]. Cognitive functioning was found to be impaired in some studies, but difficulties were diffuse and rarely those that would indicate a specific vulnerability to schizophrenia.
Interactions of such vulnerability with negative and disrupted family environments also contribute to poorer outcomes as do social variables such as poverty/adversity. Asarnow concluded that some high-risk children showed evidence of neurointegrative problems and impairments of social interaction [43]. Deficits in attention, information processing and neuromotor functioning could be more specific risk factors for schizophrenia, although many are also present in children at risk of other disorders. Family influences, such as environments of high levels of expressed emotion, might also contribute. Mednick and Schulsinger attempted a longitudinal prevention study with a population of vulnerable children on the island of Mauritius using specialised school settings and interventions [44]. However, this proved methodologically difficult and did not lead to relevant outcomes because the choice of risk factors (e.g. arousability) was not supported by later research. Also, ethical issues arise with the risk of the self-fulfilling prophecy in such studies. Such approaches would need to be better substantiated and tested, but may possibly provide evidence of developmental pathways to disorders and thus the potential to influence these for prevention.
A further neurodevelopmental vulnerability hypothesis may relate to findings for the potential influence of toxic substances, such as cannabis, and the precipitation of schizophrenic illness in adolescents/young adults. Andréasson and coworkers report that the vulnerability of a cohort of Swedish army recruits to schizophrenia was associated with the use of cannabis [45]. Causal directions and the strength of such findings have been currently debated but certainly such findings could provide opportunities for selective prevention programs. Targeting young people with education aimed at decreasing risk through decreasing marijuana use, particularly for populations where there is any family history of the illness, could decrease this potential contribution to the onset of schizophrenia.
These and other developmental psychopathology findings offer a number of opportunities for prevention. For instance, hypotheses about shyness or similarly sensitive withdrawing behaviours in children, possibly relating to later psychopathology, could mean it would be useful to provide interventions for children to assist their interpersonal skills and to deal with their social difficulties/sensitivities. Ample research exists about effective social skills training and social problem-solving training, and suggests that generic benefits for the mental health of the child may result. These benefits may decrease general vulnerability to mental ill health, including internalising anxiety/depression syndromes. They may benefit children at risk of schizophrenia if such withdrawing behaviours are established as being indicative of vulnerability. However, demonstrating such benefits may be extremely difficult because of the potential size of any effects, and the actual contribution to risk of this ‘shyness’. Nevertheless, it may be important to test the potential for such benefits as this syndrome pattern may have some continuity with the negative symptom and social impairment component of the schizophrenic syndrome pattern. Effecting this positively may decrease risk for this constellation of symptoms or give better skills to manage it, should it be a consequence in terms of avoidant phenomena of the more disruptive, psychotic symptoms of the illness. Similarly, any early cognitive difficulties/impairments as they affect school performance may usefully be targeted to build cognitive competence when and if this is possible. These interventions may ‘do good’ for mental health generally and may contribute to decreased vulnerability to schizophrenia; however, there is no evidence to establish this, and to gain such evidence would be methodologically difficult in terms of the population attributable risks associated with these vulnerabilities or preschizophrenic anlages or predisposing factors. There are a range of other generic interventions that show promise for reducing the risks for the development of schizophrenia, including high quality perinatal and childbirth programs; protection by immunisation for influenza of women contemplating pregnancy in the near future; and protection from other toxic influences including substances such as marijuana in the years of developmental risk in adolescence.
Schizophrenia: the illness and prevention
Thus, there are limitations to universal and selective approaches to the prevention of schizophrenia syndromes in the present state of knowledge. Nevertheless, the growing body of research points to the possibility of environmental interventions to influence this vulnerability in the stress-diathesis model.
Recent research has, however, shown substantial opportunities for prevention with respect to indicated interventions or early case finding and effective treatment. The National Mental Health Promotion, Prevention and Early Intervention Working Group has agreed that early intervention covers the components of the spectrum from indicated interventions for those with early symptoms or prodrome, but who do not meet full criteria for disorder, to early case finding and effective treatment at this early first-episode stage. To date, this is the most fruitful area for a prevention paradigm for schizophrenia, as amply demonstrated by the work of McGorry and colleagues in Australia [46] as well as by a number of international studies.
It is beyond the scope of this overview to detail this research, but prevention capabilities in terms of lessening risk of onset and altering duration and course in more positive directions are presently being tested. Outcomes are both positive and hopeful and should be the first line targeted on the intervention spectrum.
Also extremely relevant in terms of chronicity of the illness for many, are targeted programs for relapse prevention to lessen the likelihood of negative trajectories. Optimising recovery in every domain of functioning and symptoms, as well as quality of life and life trajectory, are important prevention goals as is also preventing disability, chronicity and impairment, and promoting living optimally with this chronic illness.
A prevention approach to schizophrenic syndromes as they affect individuals and families is also essential. This should include education for the affected person and support and education for carers about the illness and factors which may influence it and its management. This should always be in collaborative partnership with the affected person. A positive, hopeful attitude from mental health and other health professionals is also likely to be helpful, as is the nature of the health-care system response and interventions. Keeping in mind the multiple levels of comorbidity including anxiety, depression, posttraumatic stress disorder, substance use disorders and physical health problems, it is critical that overall mental health and health issues are also addressed preventively. Suicide prevention should also be part of this. A mental health promoting system of care for people at risk, or experiencing, schizophrenic disorders is critical. The cycle of research and evaluation should continually feed into prevention and care for people with schizophrenia so that a spectrum of approaches may mitigate all of the adverse impacts and improve individual and population outcomes. There can be little doubt that health promoting mental health care is a highly desirable goal for this illness, which may so adversely affect individuals and their families as well as impacting on the broader community.