
Abstract
Objectives
Reports have shown that the kynurenine pathway, one of the pathways by which tryptophan is metabolized, is activated in patients with diffuse large B-cell lymphoma (DLBCL). Activation of the kynurenine pathway triggers the production of various metabolites, such as kynurenine (Kyn), 3-hydroxykynurenine (3-HK), 3-hydroxyanthranilic acid (3-HAA), kynurenic acid (KA), and anthranilic acid (AA), which contribute to immune tolerance. The current study aimed to investigate the changes in metabolites of kynurenine pathway in DLBCL patients and evaluate their performance predicting DLBCL.
Methods
Changes in metabolites of kynurenine pathway were examined using high-performance liquid chromatography in 35 DLBCL patients (age 61.2 ± 13.5 years) and 44 healthy controls (age 58.5 ± 12.5 years).
Results
DLBCL patients had significantly higher levels of 3-HK, AA, and 3-HAA but lower levels of tryptophan (Trp) and KA compared to healthy controls. Given that the ratio of each metabolite represents the change in the Kyn pathway, the 3-HK/KA ratio was examined. Notably, DLBCL patients had a significantly higher 3-HK/KA ratio compared to healthy controls. In DLBCL, the area under the receiver operative characteristic (ROC) curve for 3-HK/KA (0.999) was higher than that for lactate dehydrogenase (0.885) and comparable to that for soluble interleukin-2 receptor (sIL-2R) (0.997). Based on ROC curve analysis, the 3-HK/KA ratio was found to be useful biomarker for the diagnosis of DLBCL.
Conclusion
Our results suggest that the 3-HK/KA ratio is a clinically useful biomarker of DLBCL. Moreover, its combination with existing markers, such as sIL-2R, can improve its effectiveness of diagnosing DLBCL.
Introduction
Over 37,000 new cases of lymphoma had been diagnosed in 2019, accounting for 5% of all new cancer cases in Japan. 1 Moreover, the number of patients with lymphoma has been increasing every year. Diffuse large B-cell lymphoma (DLBCL) is the most common type of lymphoma, accounting for approximately 30%–40% of all cases. 2 Clinically, DLBCL is the intermediate- and high-grade lymphoma, a heterogeneous group of diseases with diverse presentations, including cases that have evolved histologically from other low-grade B-cell lymphomas. 3 The current standard of care for DLBCL is R-CHOP therapy, a multidrug combination of rituximab + cyclophosphamide + doxorubicin + vincristine + prednisolone. 4 Recently, polatuzumab vedotin (Pola) with R-CHP therapy, in which vincristine was replaced with polatuzumab vedotin, has gained attention as a new standard of care in DLBCL.5,6
Evidence has shown that tryptophan (Trp) metabolism is closely related to tumour immunity and that lymphoma patients exhibit alterations in Trp metabolic pathways.5,6 Around 90% of Trp, one of the essential amino acids, is used for protein synthesis, whereas the remaining 10% is used for the synthesis of important bioactive substances, such as serotonin and kynurenine (Kyn) via the serotonin and Kyn pathways.
7
The rate-limiting enzymes responsible for the first step in the Kyn pathway are tryptophan 2,3-dioxygenase and indoleamine 2,3-dioxygenase 1 (IDO1).8,9 An overview of the Kyn pathway is depicted in Figure 1. Kyn plays a central role at the junction of three metabolic pathways on the Kyn pathway: (1) synthesis of 3-hydroxykynurenine (3-HK) and its downstream metabolites 3-hydroxyanthranilic acid (3-HAA) and quinolinic acid via kynurenine monooxygenase (KMO), (2) synthesis of kynurenic acid (KA) by kynurenine aminotransferase (KAT), and (3) synthesis of anthranilic acid (AA) by kynureninase.10,11 Diagram of the kynurenine (Kyn) pathway of tryptophan (Trp) metabolism.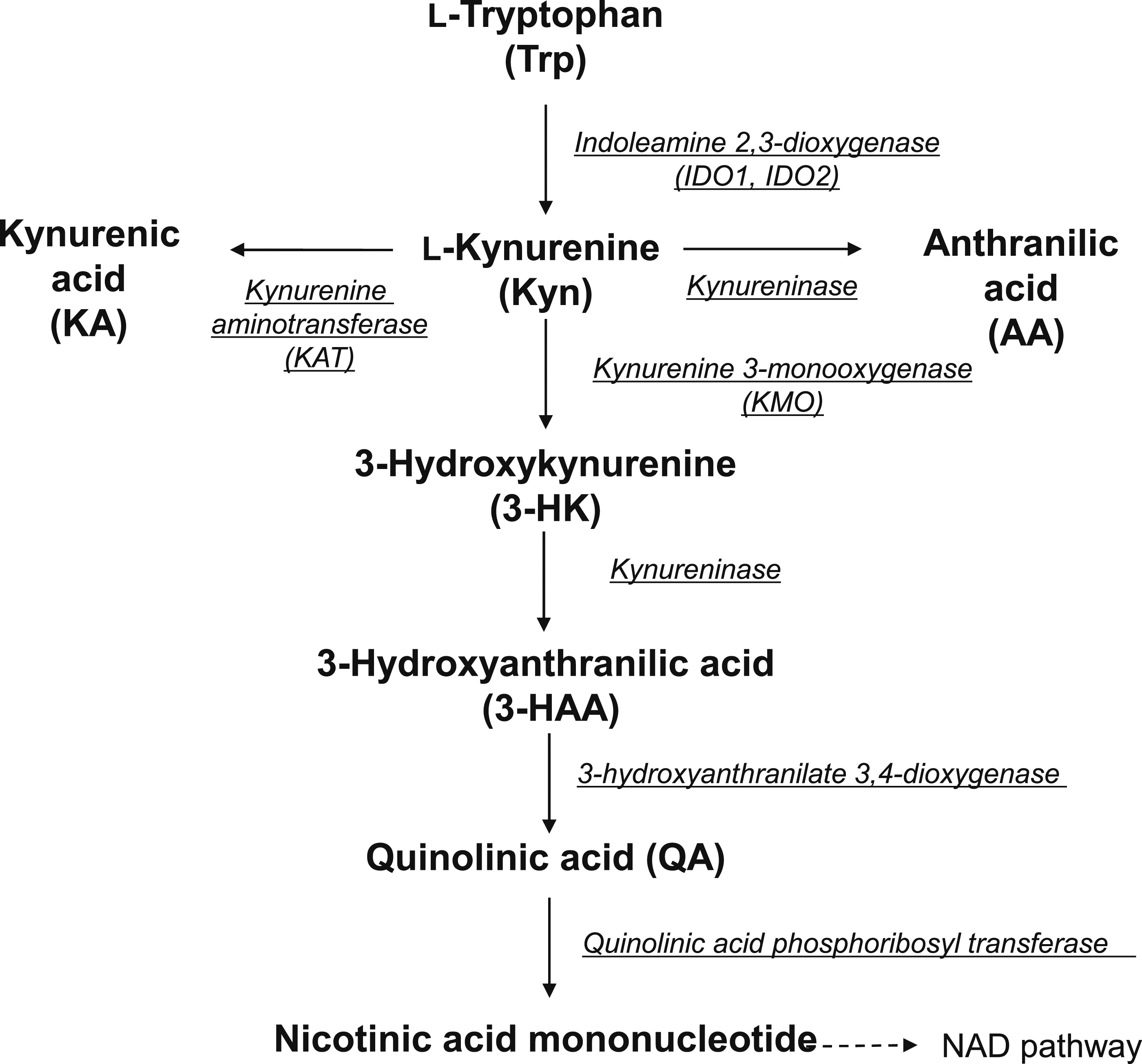
Evidence has shown that patients with myelodysplastic syndromes exhibit decreased blood concentrations of Trp and increased concentrations of its metabolite Kyn, which is known to be a biomarker for the diagnosis of myelodysplastic syndrome. 12 Previous studies have shown that IDO1 and Kyn levels are elevated in patients with DLBCL and have a poor prognosis. Serum Kyn levels have therefore been shown to be a potential new indicator of treatment outcome in DLBCL patients undergoing R-CHOP regimens.13,14
Although DLBCL patients have shown increased serum levels of Kyn, 15 the changes in tryptophan metabolites downstream of Kyn have not been fully understood. The present study therefore examined the serum levels of Trp metabolites in DLBCL patients to determine whether variations therein could be a biomarker for the detection of lymphoma.
Material and methods
Subjects
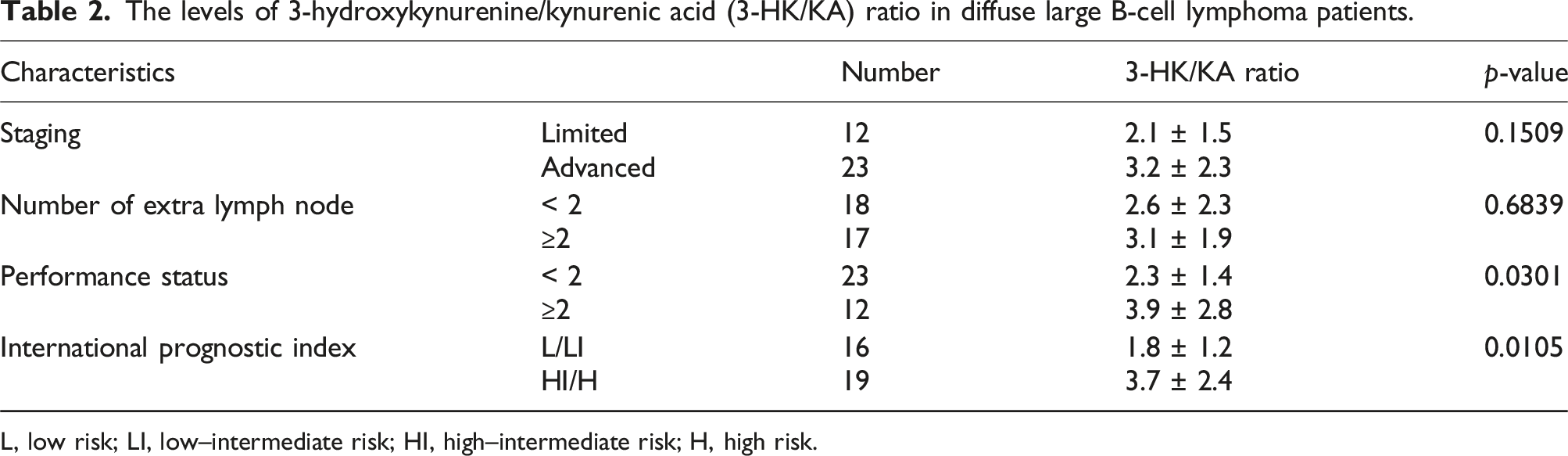
Characteristics of patients with diffuse large B-cell lymphoma.
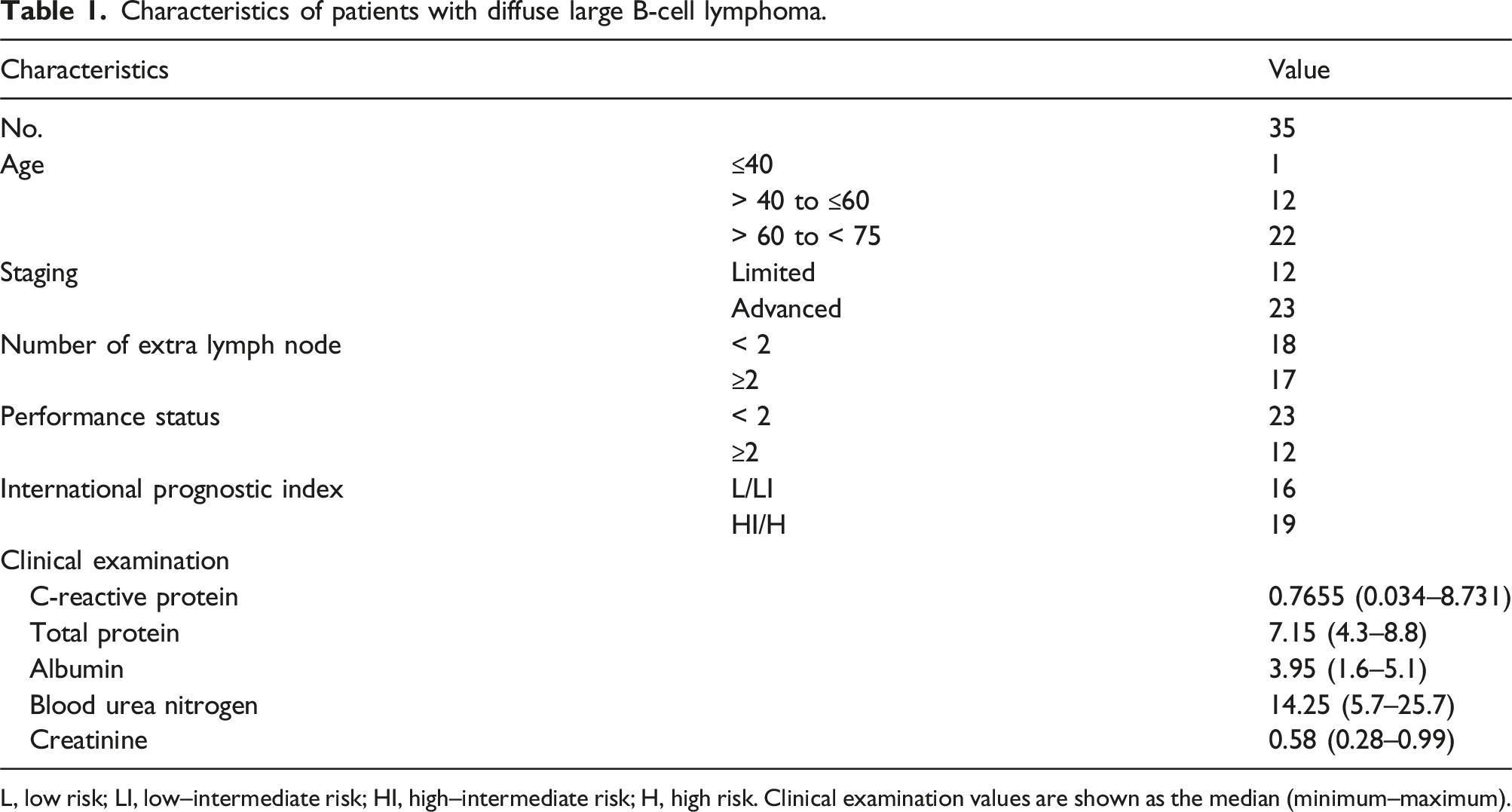
L, low risk; LI, low–intermediate risk; HI, high–intermediate risk; H, high risk. Clinical examination values are shown as the median (minimum–maximum).
All procedures involving human patients were approved by the Ethics Committees of Fujita Health University (Toyoake, Japan; approval no. HM20-446). This study was performed in accordance with the principles of the Declaration of Helsinki.
Measurement of Trp–Kyn pathway metabolites in sera
Trp metabolite levels were measured using a method reported previously. 16 Briefly, the levels of Trp, Kyn, AA, KA, and 3-HAA were quantified using high-performance liquid chromatography (HPLC) (SHIMADZU, Kyoto, Japan), whereas 3-HK levels were measured using HPLC through an ECD 300 electrochemical detector (Eicom, Kyoto, Japan) with an applied potential of 550 mV. After mixing sera with 10% perchloric acid (1:4), the mixture was centrifuged at 14,000 r/min for 10 min (4°C). Thereafter, 20 µL of the supernatant was injected into the HPLC instrument. The mobile phase consisted of 0.34 mM ethylenediaminetetraacetic acid, 14 mM sodium heptane sulfonate, 5% phosphoric acid, and 0.9% triethylamine containing 4% acetonitrile and was pumped at a flow rate of 0.5 mL/min. The column used was EICOMPAK 3.0 × 150 mm SC-5ODS (Eicom, Kyoto, Japan) with a particle size of 5 µm kept at 25°C.
Measurement of LDH and sIL-2R in sera
Levels of LDH and sIL-2R were examined the residual serum sample. Serum samples were stored at −80°C before use. Levels of LDH were measured using biochemical analyzer JCA-BM9130 (JEOL, Tokyo, Japan) in 35 DLBCL patients and 43 healthy controls. Levels of sIL-2R were detected by enzyme-linked immunosorbent assay (ELISA) using kits (human sIL-2R kit, Thermo Fisher Scientific, Inc., MA, USA) in 24 DLBCL patients and 31 healthy controls.
Statistical analysis
The obtained values were expressed as mean ± standard deviation (SD). Welch’s t test was used to compare the Trp–Kyn pathway metabolite data between the unpaired groups. To determine the correlations among the quantified parameters, Pearson’s product moment correlation coefficients and their statistical significance were calculated. Differences with P-values <0.05 were considered statistically significant.
Results
Measurement of Trp–Kyn pathway metabolites in sera of DLBCL patients
First, the amount of Trp metabolites in sera was examined in both healthy controls and DLBCL patients (Figure 2). Notably, serum levels of Trp and KA were significantly lower in DLBCL patients (Trp: 45.1 ± 12.7 μM, KA: 25.4 ± 12.2 nM) than in healthy controls (Trp: 53.5 ± 10.3 μM, KA: 40.3 ± 13.2 nM). However, 3-HK, 3-HAA and AA levels were higher in the DLBCL patients (3-HK: 59.9 ± 37.8 nM, 3-HAA: 23.6 ± 21.9 nM, AA: 22.9 ± 19.7 nM) compared to those of healthy controls (3-HK: 16.9 ± 5.7 nM, 3-HAA: 7.2 ± 4.3 nM, AA: 15.4 ± 7.1 nM) (Figure 2). These findings indicate that DLBCL patients have a more variable base axis of tryptophan metabolism compared to that of healthy controls. Serum tryptophan (Trp) metabolite levels in Kyn pathway of diffuse larger B-cell lymphoma (DLBCL) patients and healthy controls (HC). Differences in Trp metabolite levels between HC and DLBCL patients. Trp metabolites, such as kynurenine (Kyn), 3-hydroxyanthranilic acid (3-HAA), kynurenic acid (KA), 3-hydroxykynurenine (3-HK), and anthranilic acid (AA), were measured using high-performance liquid chromatography. The obtained values are expressed as mean ± standard deviation. *P < .05, ***P < .001, ****P < .0001; significant difference in values as determined using Welch’s t test.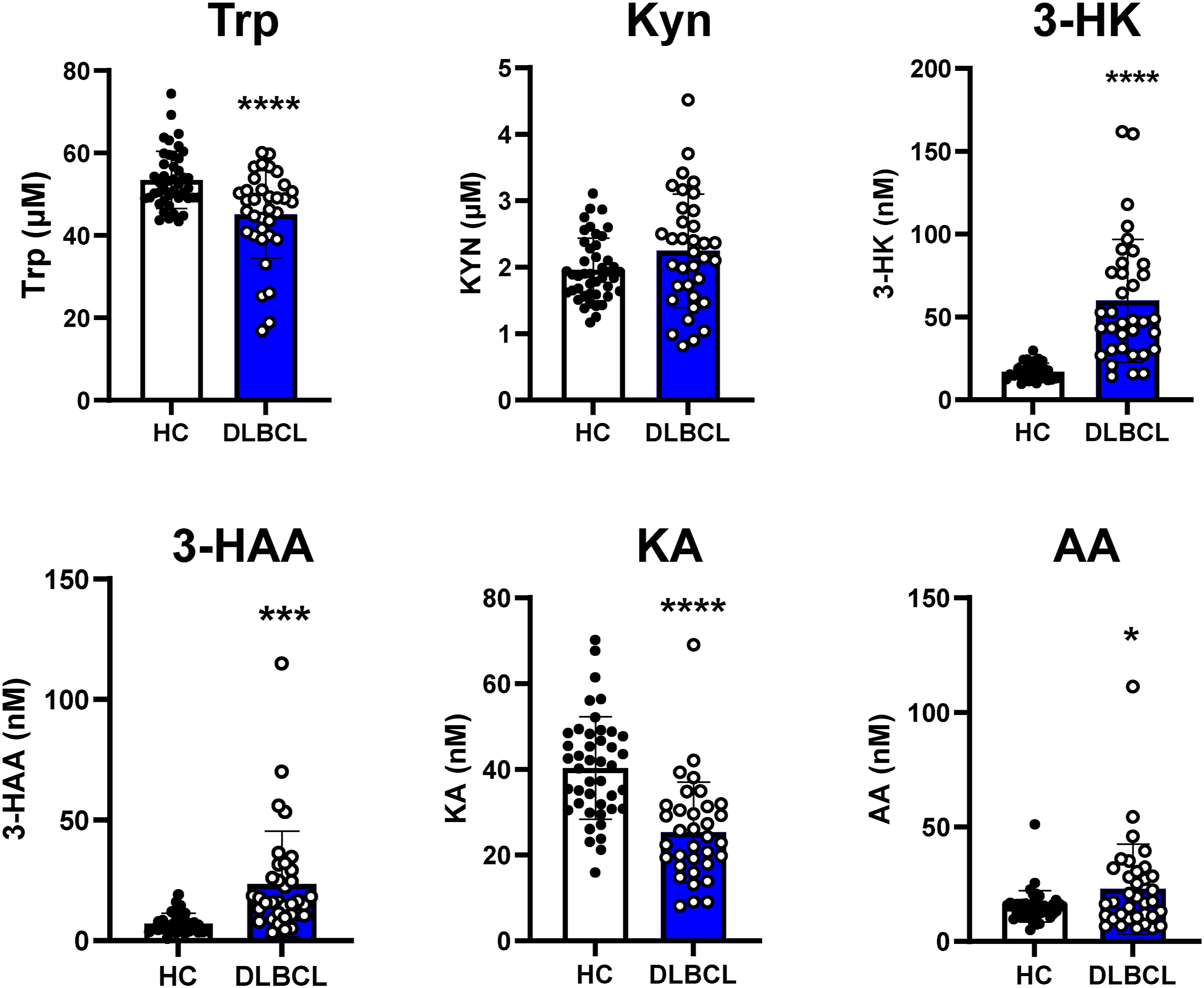
Significant increase in the 3-HK/KA ratio in DLBCL patients
Next, we evaluated the 3-HK/Trp and 3-HK/KA ratios, which are highly variable metabolites, as indicators of shift in the tryptophan metabolic pathway. The 3-HK/Trp and 3-HK/KA ratios were significantly greater in DLBCL patients than those in healthy controls (Figure 3). In DLBCL patients, the 3-HK/KA ratio showed a significantly greater difference in variability than that of the 3-HK/Trp ratio. To examine the predictive value of the 3-HK/KA ratio with respect to the clinical grade, comparisons were made for clinical indices. No significant differences were found between the low and high groups as regards the clinical stage and number of extranodal lymph nodes. However, the 3-HK/KA ratio was significantly higher in the high group than in the low group with respect to the performance status and international prognostic index (Table 2). Tryptophan (Trp) metabolite ratio in diffuse larger B-cell lymphoma (DLBCL) patients and healthy controls (HC). Differences in the ratios of 3-HK/Trp and 3-HK/KA between HC and DLBCL patients. The obtained values are expressed as mean ± standard deviation. ***P < .001, ****P < .0001; significant difference in values as determined using Welch’s t test. The levels of 3-hydroxykynurenine/kynurenic acid (3-HK/KA) ratio in diffuse large B-cell lymphoma patients. L, low risk; LI, low–intermediate risk; HI, high–intermediate risk; H, high risk.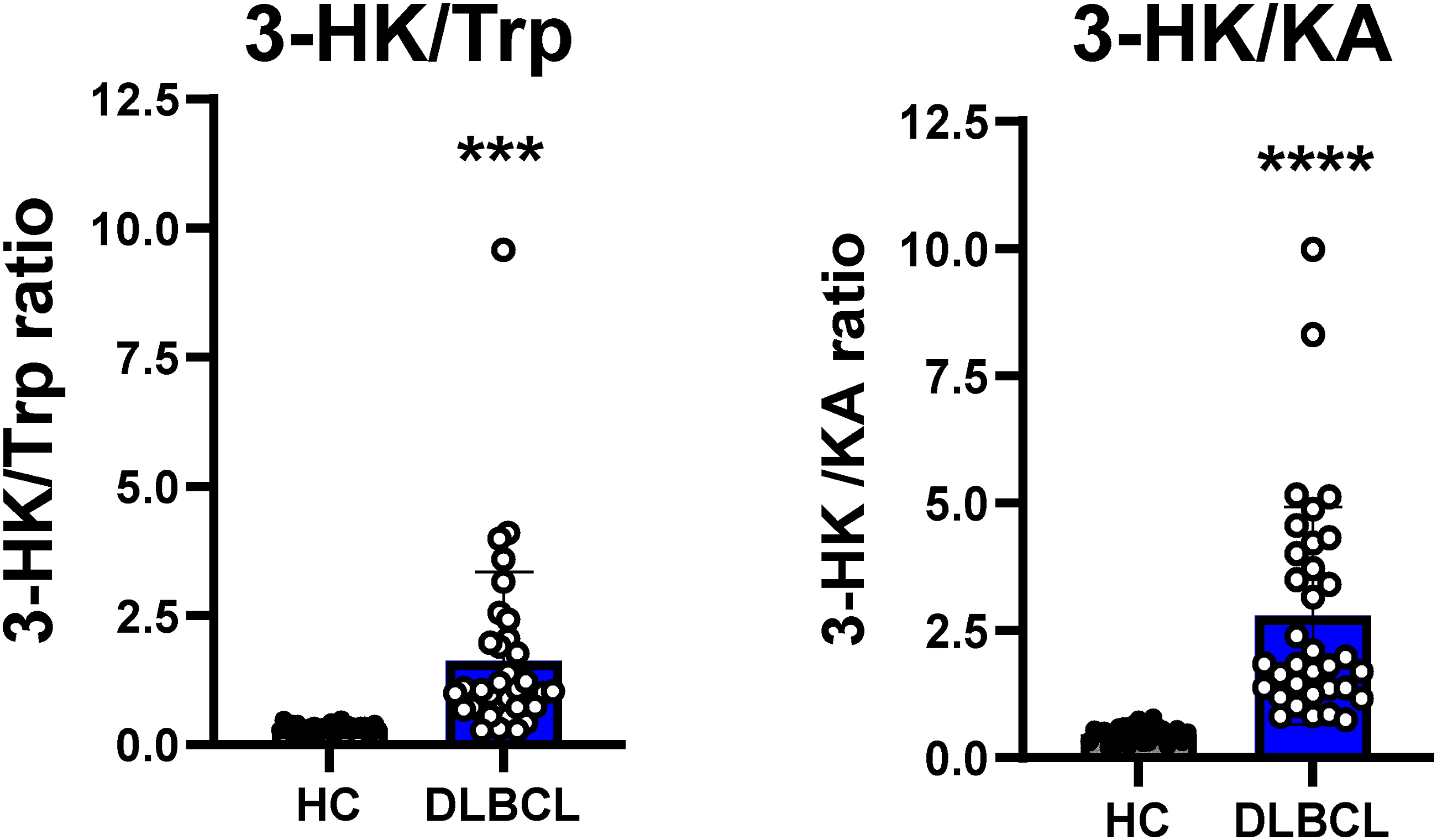
The association of the 3-HK/KA ratio with inflammatory status and renal function were also examined. The serum 3-HK/KA ratio did not correlate with serum blood urea nitrogen (BUN) and creatinine concentrations (r = −0.174; P = .3399, r = −0.118; P = .5190) but correlated with the serum C-reactive protein (CRP) levels (r = 0.476; P < .001) (Supplemental Figure 1).
Correlations between serum 3-HK/KA and serum biomarkers of DLBCL
DLBCL patients showed elevate level of 3-HK/KA ratio compared to healthy controls. Therefore, the utility of the 3-HK/KA ratio was compared to that of existing biomarker molecules, such as lactate dehydrogenase (LDH) and serum soluble interleukin-2 receptor (sIL-2R).17,18 Given that serum sIL-2R and LDH levels have been elevated in various lymphomas, both are well-known and frequently used as diagnostic and prognostic biomarkers for DLBCL. Serum levels of LDH and sIL-2R were significantly higher in patients with DLBCL (LDH, 472.2 ± 684.4U/L; sIL-2R, 15.7 ± 15.0 ng/mL) than in healthy controls (LDH, 168.5 ± 37.2 U/L; sIL-2R, 2.0 ± 0.5 ng/mL). Interestingly, we found that the serum 3-HK/KA ratio was not correlated with serum LDH concentrations (r = 0.256; P < .05) (Figure 4(a)) but correlated with serum sIL-2R levels (r = 0.738; P < .0001) (Figure 4(b)). These results show that 3-HK/KA could be a new sensitive biomarker for DLBCL. Correlation between serum 3-hydroxykynurenine/kynurenic acid (3-HK/KA) ratio and existing biomarkers in diffuse larger B-cell lymphoma (DLBCL) patients and healthy controls (HC). Pearson’s correlation coefficients were examined between 3-HK/KA ratio and lactate dehydrogenase (a) and soluble interleukin-2 receptor (b).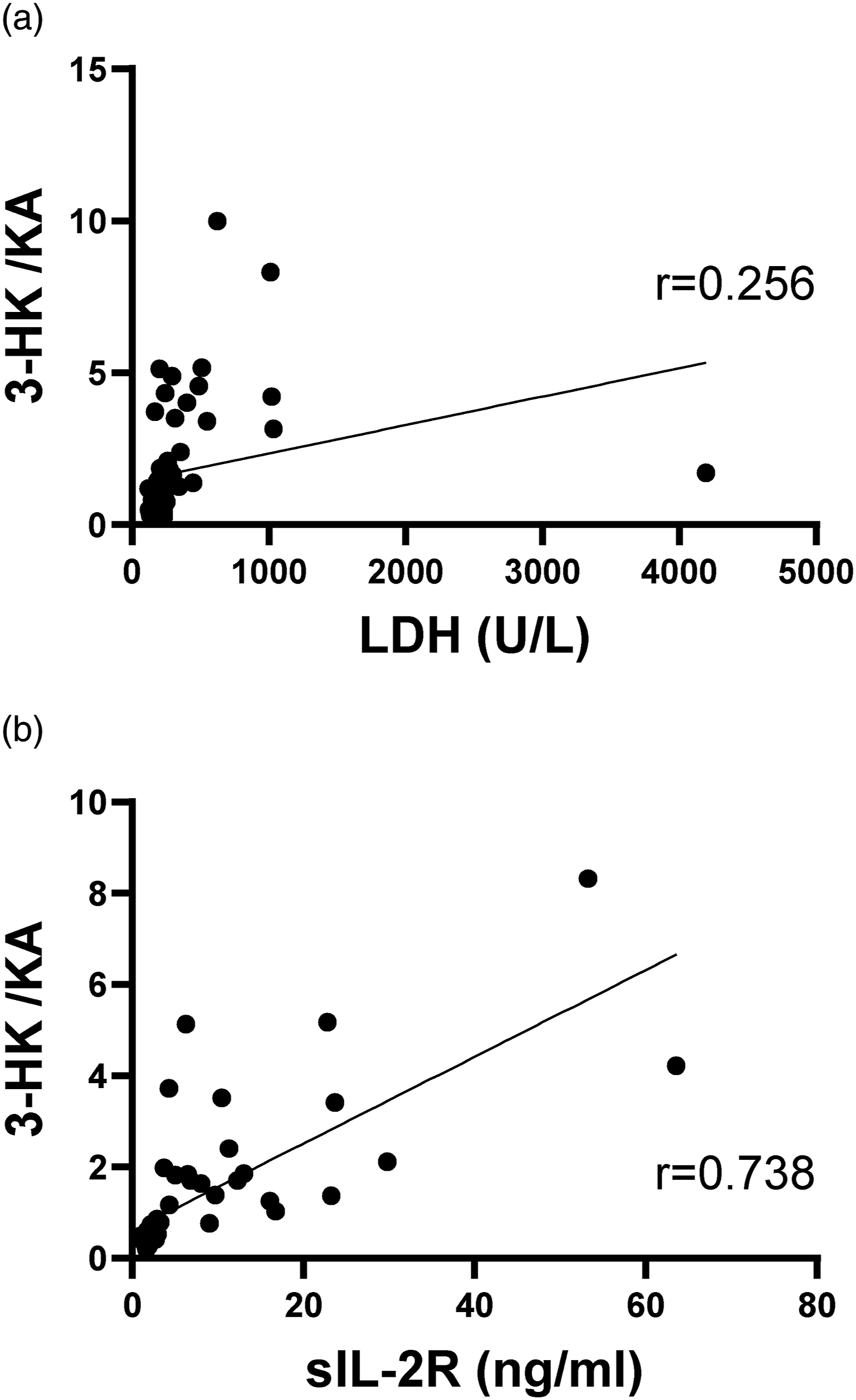
Receiver operative characteristic analysis of the 3-HK/KA ratio in DLBCL
Next, we evaluated the effectiveness of the 3-HK/KA ratio as a biomarker to detect DLBCL using area under the curve (AUC) analysis. As we expected, AUC analysis revealed an AUC of 0.999 for 3-HK/KA. In contrast, LDH and sIL-2R showed low AUC such as 0.885 (P < .05) and 0.997 (P = .688), respectively (Figure 5). The receiver operative characteristic curve strongly indicated that the 3-HK/KA ratio has excellent performance for diagnosis of DLBCL. Receiver operating characteristic (ROC) curves for the association between the 3-hydroxykynurenine/kynurenic acid (3-HK/KA) ratio and existing biomarkers in diffuse larger B-cell lymphoma (DLBCL) patients and healthy controls (HC). Receiver operating characteristic curve analysis for predicting DLBCL patients in LDH and 3-HK/KA (a), sIL-2R and 3-HK/KA (b).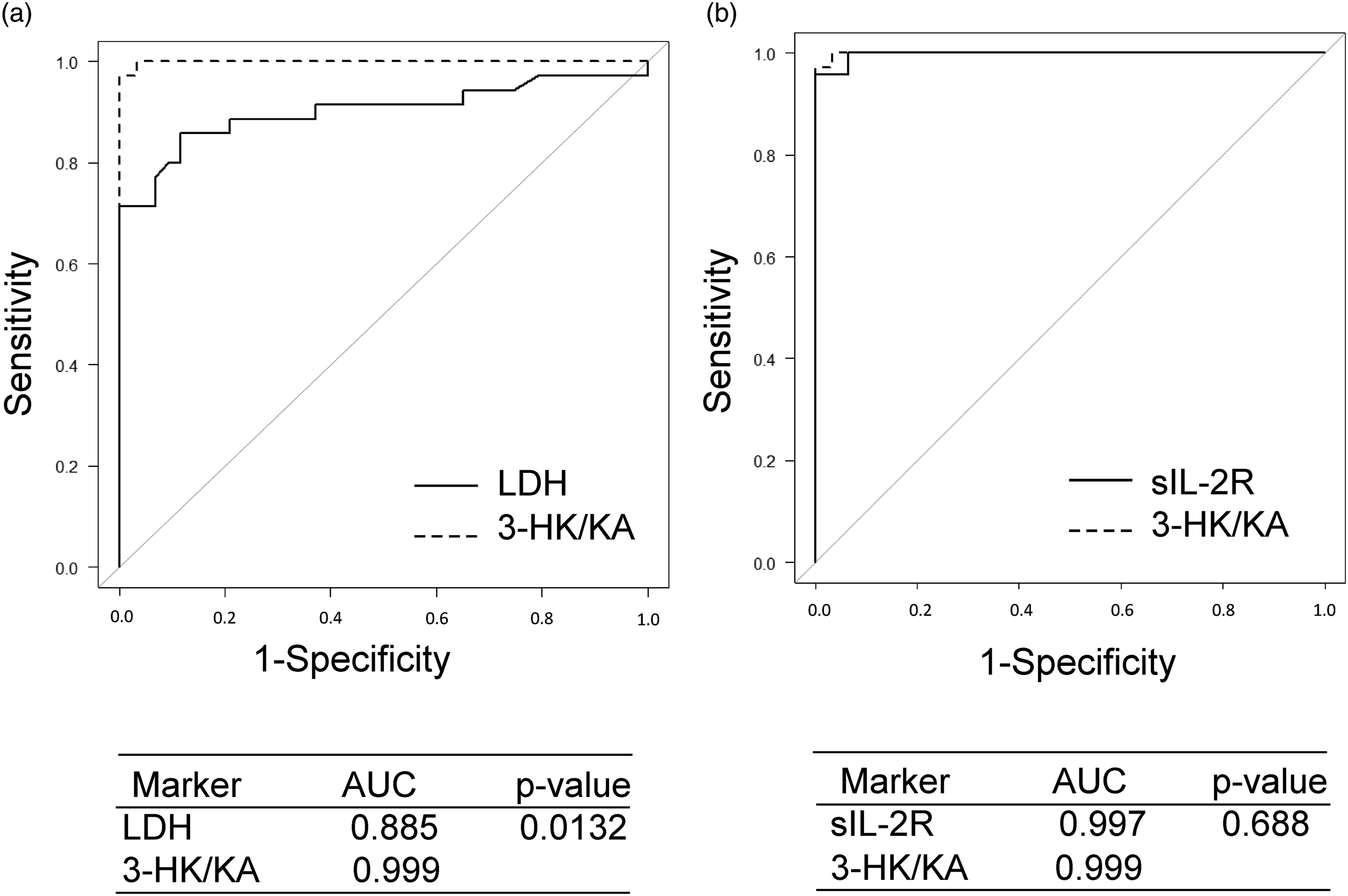
Discussion
Previous studies have reported that serum Kyn level increased by enhanced expression of indoleamine 2,3-dioxygenase 1 (IDO1) in various cancer cases.5,14,19 In DLBCL patients, Ninomiya et al. have suggest IDO1 expression predicts overall survival in those with treated with R-CHOP chemotherapy. 20 Furthermore, given that the Trp metabolism enzymes involved in DLBCL are associated with PD-L1 expression, combination of Trp-metabolizing enzyme inhibitors with anti-PD-L1 or other immunotherapeutic agents could be a potential strategy for the clinical treatment of DLBCL. 21
Further the production of 3-HK and KA by activation of the kynurenine pathway evades immune surveillance and is closely associated with tumour development, and changes in the expression of both KAT and KMO enzymes have been observed in a variety of cancers. First, several studies have focused on the KA level based on the enhancement of KAT activation in various types of cancer, which revealed some differences in KA levels between cancer and physiological conditions. 22 KA is elevated in the serum of patients with colon cancer and non-small cell lung cancer compared to healthy volunteers and correlates with prognosis. 23 Higher KA level in serum compared to healthy population is also observed in blood disorders, such as monoclonal gammopathy of undetermined significance (MGUS), representing premalignant conditions, multiple myeloma (MM), 24 and myelodysplastic syndrome (MDS). 12 In contrast, serum KA in glioblastoma patients or primary cervical cancer has been reported to be reduced compared to healthy controls. 25 These findings suggest that the inhibition of branching to KA production differs according to the type of carcinoma and requires further investigation.
Limited studies have been available on the molecular biological function of KMOs in cancer. The most recent study has demonstrated that serum 3-HK levels vary independent of Kyn levels in patients with DLBCL, that increases serum 3-HK levels and KMO activity serves as indicators of disease progression, and that the addition of KMO inhibitors or 3-HK could regulate the viability of DLBCL cells in vitro. 26
In the present study, the levels of 3-HK produced by KMO were significantly elevated. In the kynurenine pathway, Kyn is metabolized to AA or 3-HK-3-HAA or KA, but the amounts of downstream metabolites of Kyn are different for each metabolite. The levels of AA and 3-HK may increase with increasing Kyn levels. However, the levels of KA decreased despite the increase in Kyn.
Our data indicate an enhanced shift towards the 3-HK branch and suppression of the KA branch in DLBCL patients compared to healthy controls. 3-HK and KA are produced from Kyn by KMO and KAT, respectively. These results indicate that the tumour microenvironment affects the activity of KAT or KMO in kynurenine pathway.
Interestingly, our data showed an enhanced shift to the 3-HK branch and suppression of the KA branch in the Kyn pathway among DLBCL patients. Increased KA levels have been reported to suppress inflammation,27,28 which plays an important role in tumorigenesis and metastasis. Furthermore, the shift to the 3-HK branch may induce nicotinamide adenine dinucleotide synthesis, promoting energy production. Therefore, metabolic changes that decrease KA and increase 3-HK levels may be beneficial for increasing energy production in tumours. Nonetheless, further studies should perform to elucidate the mechanisms, by which changes in these metabolites contribute to tumour malignancy. However, changes in tryptophan metabolites may closely associate with immune function in the tumour environment.
Further, the present study evaluated not only the serum profiles of Trp–Kyn pathway metabolites, but also the ratios of these metabolites in DLBCL patients. Consequently, our findings showed that DLBCL patients had significantly lower serum Trp and KA levels, but markedly higher the Kyn, AA, 3-HAA, and 3-HK levels compared to healthy controls (Figure 2). The 3-HK/KA ratio was then examined whether the ratio of metabolites clearly shows changes in metabolism within the Kyn pathway. Notably, we found that the 3-HK/KA ratio was significantly increased in DLBCL patients (Figure 3). Furthermore, the 3-HK/KA ratio was significantly higher in the high group than in the low group with respect to performance status and international prognostic index (Table 2). These results indicate that DLBCL patients had a more variable Kyn pathway compared to healthy controls.
The kynurenine pathway is related to the inflammation because IDO1, the kynurenine pathway rate-limiting enzyme, is induced by inflammatory cytokines. The serum 3-HK/KA ratio was correlated with serum CRP levels (r = 0.476; P < .001). We have previously reported alterations in kynurenine pathway metabolites in psoriasis, an inflammatory skin disease. Although changes in metabolites were also detected in patients with psoriasis, 29 changes in patients with DLBCL were greater than in those with psoriasis.
In the diagnosis of lymphoma, numerous tests are performed to determine the type and stage of the disease, including lymph node biopsy, tumour biopsy, blood tests, X-rays, ultrasound, computed tomography, and others. Among these tests, blood tests are the easiest and least burdensome to perform and indeed play a crucial role in the diagnosis of cancer. LDH is one of the biomarkers commonly used in the diagnosis of lymphoma. In some cases, sIL-2R levels are also used as a tumour marker for malignant lymphoma. However, it is important to note that sIL-2R and LDH levels may not change in some cases of lymphoma and can even be altered due to causes other than lymphomas. Previous studies have shown that sIL-2R for lymphoma diagnosis had a maximum sensitivity of 35% and specificity of 87%.30,31 Therefore, some time, they show low values which prolongs the detection of tumours. For several cancers, a delay in treatment by even 1 month has often been associated with a 6%–13% increased risk of death. 29 Previous studies have reported that the time to diagnosis of various types of lymphoma falls between 2.5 months and 1 year.32,33 For some lymphomas, such as DLBCL, a delay in the diagnosis can negatively influence outcomes of therapy and shorten the duration of remission.
Further, prolonged delay in cancer diagnosis increases patient anxiety and reduces their quality-of-life. Therefore, rapid and accurately cancer diagnosis is important to detect cancer at an early stage. Our present AUC results show that 3-HK/KA ratio is a sensitive biomarker in DLBCL detection. However, the number of cases was small; thus, further studies are needed to determine the effectiveness of the 3-HK/KA ratio. Furthermore, the kynurenine pathway is also thought to be variable in other cancer types. Therefore, the metabolites in the kynurenine pathway may be a potential marker for other cancer types
Based on our findings, measurement of the 3-HK/KA ratio could be a valuable diagnostic tool for the prediction and diagnosis of DLBCL. We speculate that measurement of both sIL-2R and 3-HK/KA ratio could significantly improve the detection rate, which could be particularly helpful in cases facing delays in diagnosis.
Supplemental Material
Supplemental Material - Usefulness of the 3-hydroxykynurenine/kynurenic acid ratio as a diagnostic biomarker for diffuse larger B-cell lymphoma
Supplemental Material for Usefulness of the 3-hydroxykynurenine/kynurenic acid ratio as a diagnostic biomarker for diffuse larger B-cell lymphoma by Yasuko Yamamoto, Naoe Goto, Kengo Kambara, Suwako Fujigaki, Hidetsugu Fujigaki, Masao Takemura, Toshitaka Nabeshima, Akihiro Tomita, and Kuniaki Saito in Annals of Clinical Biochemistry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the FUJIFILM Corporation.
Ethical approval
Fujita Health University Research Ethics Board (HM20-446) approved this study.
Guarantor
KS.
Contributorship
YY, NG, KK, SF, and TM researched literature and conceived the study. YY gained ethical approval and wrote the first draft of the manuscript. YY, NG, KK, SF, HF, and TM involved in the investigation and data analysis. NG and AT involved in the supply of clinical laboratory data. TN, AT, and KS involved as supervision and project administration. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.