
Abstract
We introduce a 16-year-old female who presented with tender cervical lymphadenopathy, prolonged fever, and hypothyroidism. After excluding common causes of fever of unknown origin, a surgical biopsy of cervical lymph nodes revealed Kikuchi-Fujimoto disease. The patient showed improvement with a short-term course of NSAIDs. An increased titre of thyroperoxidase antibody led to a diagnosis of Hashimoto’s thyroiditis during stable condition. This report underscores the importance of considering Kikuchi-Fujimoto disease in the differential diagnosis of prolonged fever of unknown origin with lymphadenopathy and highlights the association with Hashimoto’s thyroiditis, advocating for vigilance regarding hypothyroidism in long-term follow-up after Kikuchi-Fujimoto disease recovery.
Keywords
Introduction
Necrotizing histiocytic lymphadenitis, also known as Kikuchi-Fujimoto disease (KFD), is a rare disorder characterized by necrotizing lymphadenitis predominantly in the cervical region and prolonged fever. Initially described by two Japanese pathologists Kikuchi and Fujimoto in 1972. KFD has a higher prevalence in the Asian population, although cases have been reported worldwide. 1 This condition most commonly affects children and adults under 30 years of age, with a modest female preponderance. 2 The exact cause of KFD remains to be elucidated, but infectious and autoimmune aetiologies have been proposed. 3 Patients typically present with cervical lymphadenopathy and fever. Other symptoms include erythematous rashes, arthritis and hepatosplenomegaly. 4 An excisional lymph node biopsy is essential for confirming definitive diagnosis although it is commonly performed after excluding other usual causes. KFD is a benign, self-limited disease that often resolves after several weeks to months. Fatality is rare, but fatal complications such as disseminated intravascular coagulopathy, hemophagocytic syndrome, severe infection, acute heart failure, pulmonary haemorrhage has been reported. 5 Some studies indicate the development of autoimmune disease several months to years after a KFD diagnosis, such as systemic lupus erythematosus (SLE), Sjögren’s syndrome or Hashimoto thyroiditis. 3 Herein we report a case of a patient with KFD co-occurring with Hashimoto thyroiditis.
Case presentation
A 16-year-old Vietnamese female patient presented to our department with prolonged fever of unknown origin (FUO). The patient reported episodic high-grade fever for 3 weeks, which was relieved by acetaminophen. On day 14, she noticed a thumb-sized, swollen, and painful mass in the left side of her neck. Associated symptoms included fatigue, anorexia, night sweats and a 4-kg-weight loss. Despite supportive treatment for 3 weeks, her symptoms did not improve. She was then admitted to our hospital. She denied any recent upper respiratory symptoms, vaccinations, or medications. Her medical and family history were unremarkable.
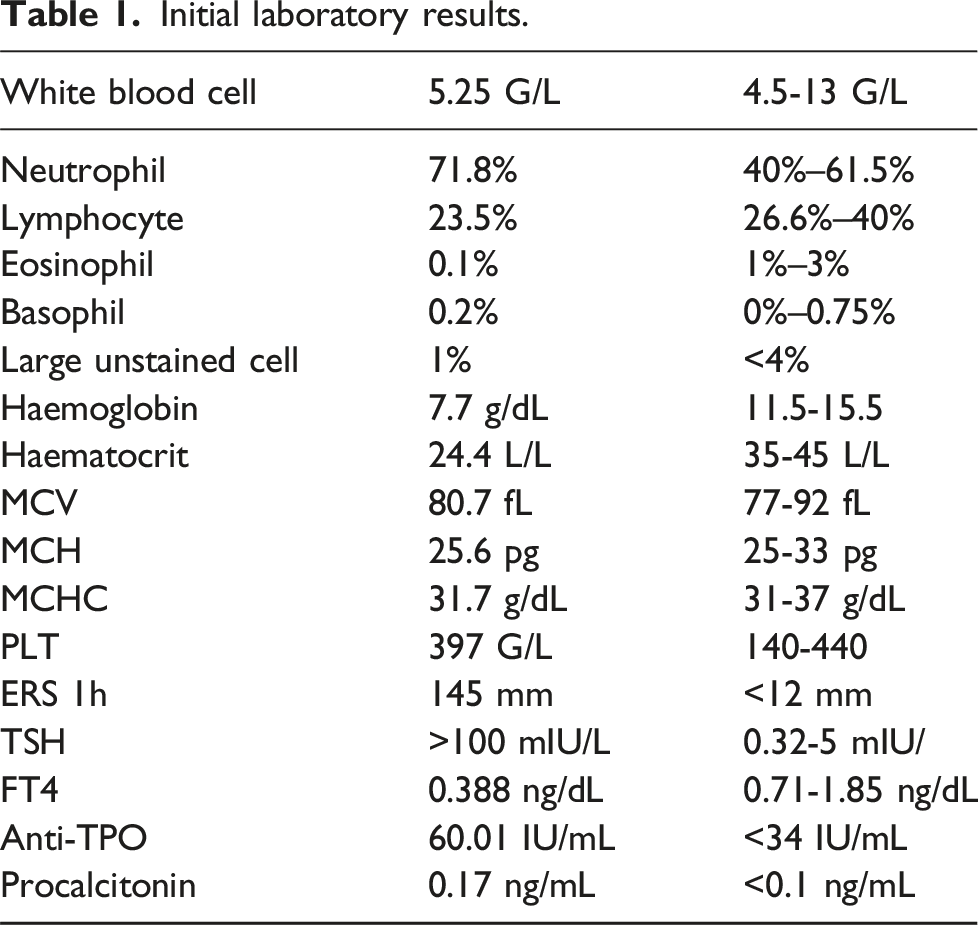
On physical examination, the patient appeared pale and febrile. Vital signs were otherwise normal. The neck examination showed an enlarged level IV lymph node, measuring 2 × 1 cm, well-demarcated, rubbery, mobile, and tender. She had multiple erythematous macules scattered on her trunk and extremities. Other regional examinations revealed no abnormalities. A presumptive diagnosis of purulent lymphadenitis was made. A neck ultrasound was then indicated, which revealed left cervical lymphadenopathy in level I, IV, VI with maximum dimension of 14 × 7 mm, hypoechogenicity, vertical axis, thin cortex, and preserved hilum structure (Figure 1). Concurrently, a diffusely hypoechoic and hyperperfusion thyroid was noted, consistent with thyroiditis. Initial laboratory results, as shown in Table 1, underscored marked normocytic anaemia and prolonged erythrocyte sedimentation rate. Thyroid function tests were also indicated due to thyroiditis, revealing low FT4 and markedly high thyroid stimulating hormone (TSH), consistent with primary hypothyroidism. On peripheral blood smear, a reduced number of erythrocyte and anisocytosis was noted, with absence of abnormal cells. Neck ultrasound revealed level IVc cervical lymphadenopathy. Initial laboratory results.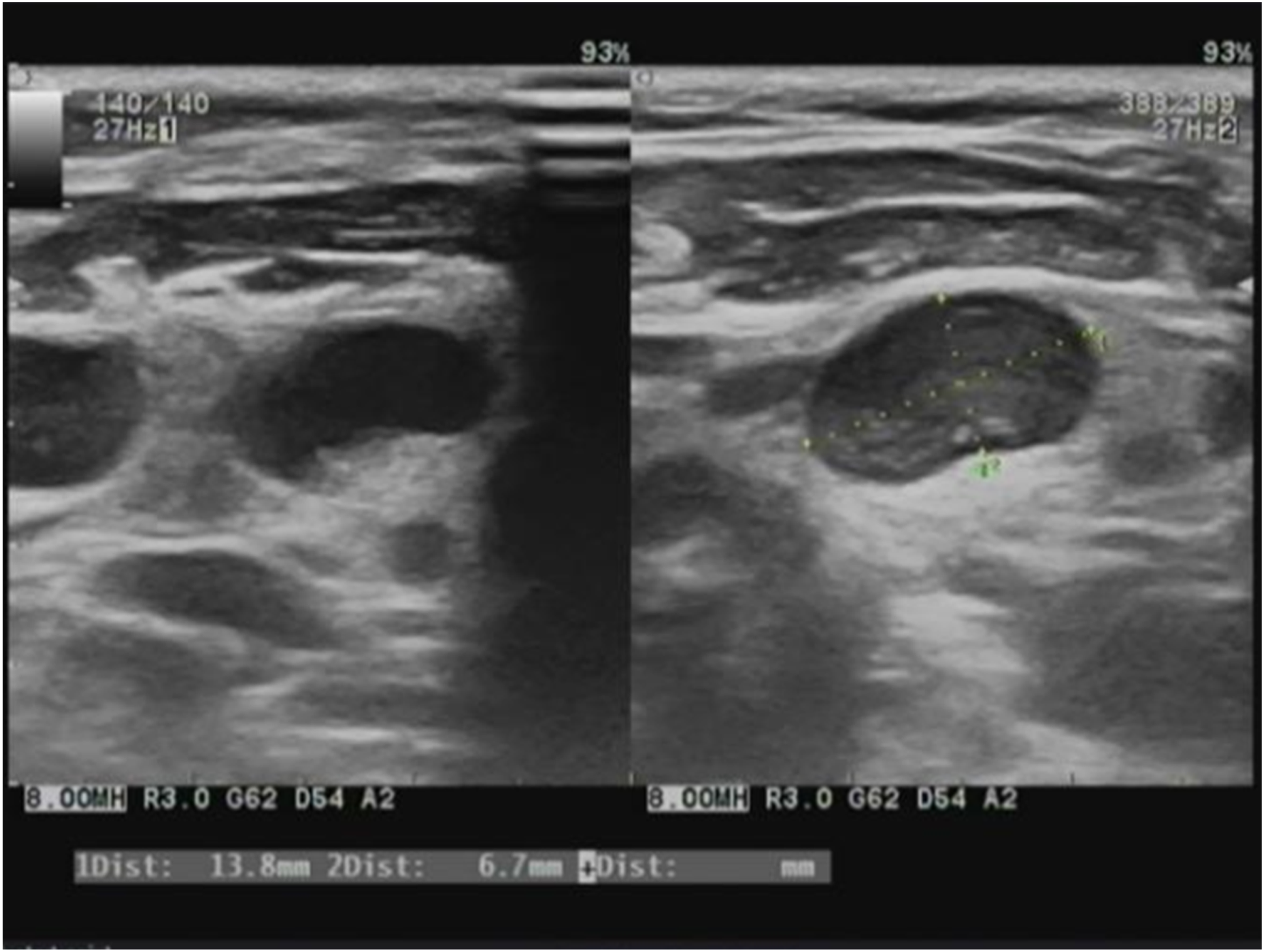
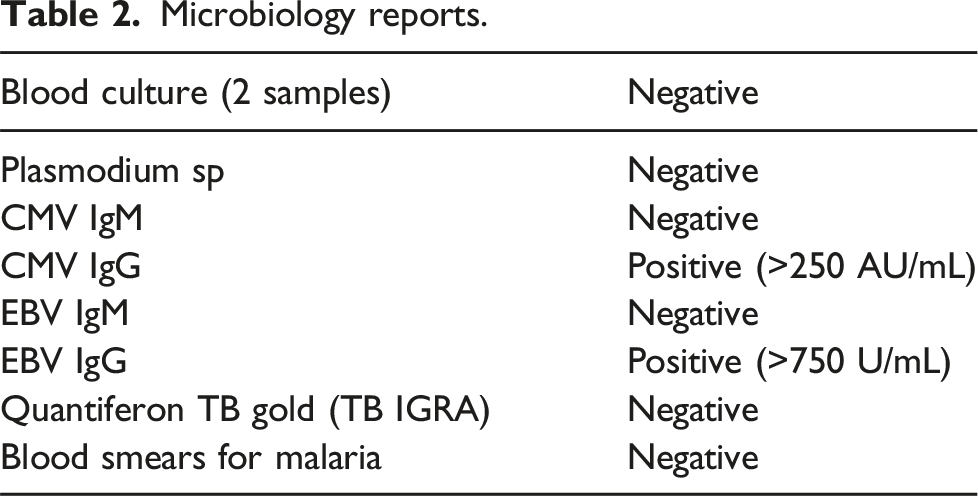
Microbiology reports.
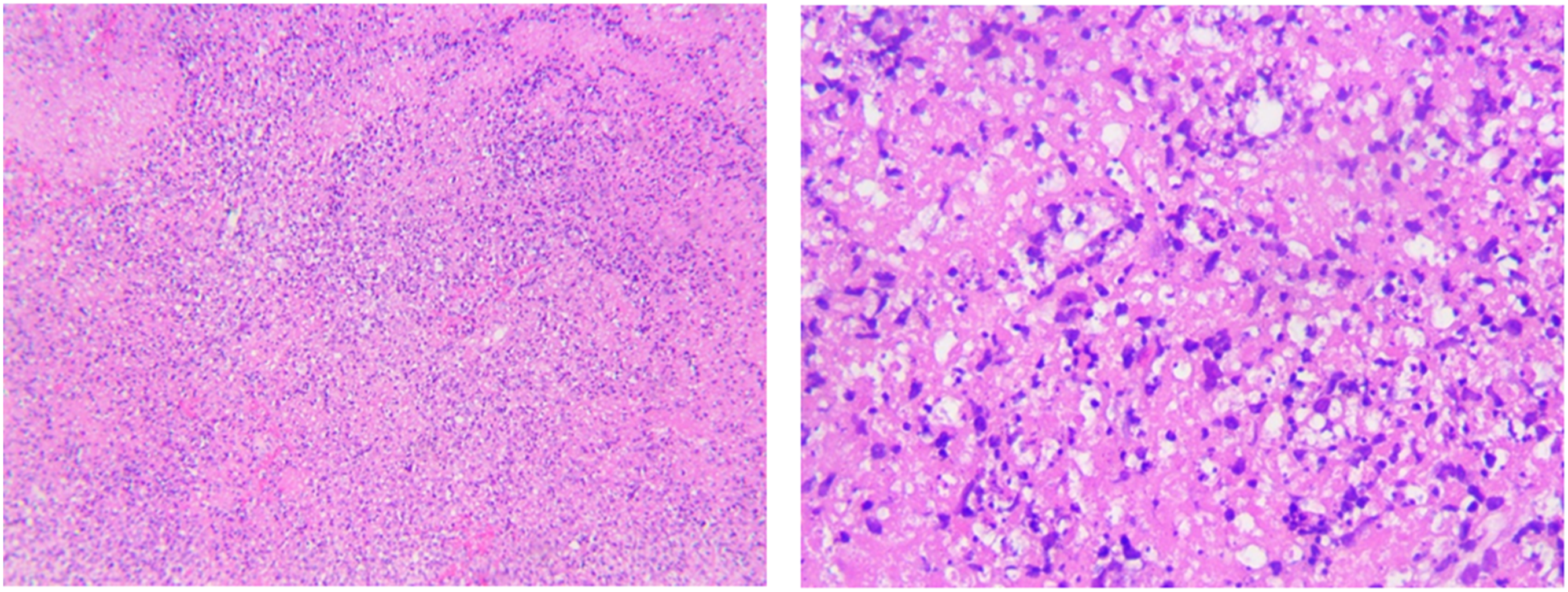
Microphotography of a paracortical area of a lymph node (H&E).
Antibiotics were then discontinued because there was no evidence of infection. We informed the patient of the typically benign course of KFD and prescribed a non-steroidal anti-inflammatory drug (NSAID) for supportive treatment. After 3 days, her fever was reduced, and she was discharged with etoricoxib and levothyroxine. At a follow-up visit 4 weeks after discharge, she appeared well, and her fever was resolved. Thyroid function tests were in the normal range with recent levothyroxine dose. Thyroperoxidase antibody (TPO-Ab) concentration was high (113 IU/mL, reference range: <34 IU/mL), consistent with Hashimoto thyroiditis.
Discussion
KFD, or necrotizing histiocytic lymphadenitis, remains an enigmatic clinical entity due to its elusive aetiology and variable presentation. It was first thought to predominantly affect young adults, but more paediatric cases have been reported in recent years. Compared to adults, children tend to have more tender lymphadenopathy, and present with fever and skin rash more commonly. 6 This case of a 16-year-old patient intriguingly illustrates the association of KFD with autoimmune conditions, specifically Hashimoto thyroiditis, prompting a discussion on the implications for diagnosis, management, and understanding of the disease’s pathophysiology.
KFD typically presents with lymphadenopathy and fever, as seen in our patient. The disease’s predilection for the cervical lymph nodes and its self-limiting nature are characteristic, albeit not specific, as these features and can be observed in several other diseases. Prolonged fever occurs in approximately one-third of paediatric patients and does not seem to be a prognostic factor. 7 The clinical presentation can mimic several other diseases including fatal conditions, necessitating a thorough diagnostic process. Our patient’s symptoms, while aligning with KFD, were initially confusing due to the overlapping features with other lymphadenopathies and thyroiditis. The excisional biopsy, which is the gold standard for diagnosis, was pivotal in confirming KFD in this instance.
The differential diagnosis for FUO in this patient was extensive. Lymphomas, infectious mononucleosis, and tuberculosis are prime considerations, all of which were methodically excluded through clinical and laboratory evaluations. The role of imaging, particularly ultrasound in our case, proved beneficial not only in supporting the suspicion of KFD but also in identifying concurrent thyroiditis. Ultrasonographic findings of KFD commonly include posterior cervical sites, conglomerated nodal distribution, preserved central nodal echogenic hilum, and perinodal fat swelling. 8 These characteristics are not unique to KFD but are also observed in other lymphadenopathies, necessitating careful interpretation within the clinical and laboratory context. The negative serologies for common infectious agents and the absence of malignancy markers on peripheral smear were informative in narrowing the diagnosis to KFD.
Management of KFD primarily involves symptomatic relief, with anti-inflammatory agents being the mainstay of treatment. A study reported that nearly half of the patients had symptom resolution within 1 week after surgical biopsy, suggesting the role of excision biopsy as a therapeutic intervention. 9 Antibiotics, as in our patient’s course, may be employed until bacterial infections are ruled out. The worsening of symptoms on antibiotics underscores the necessity to revisit the diagnosis in persistently febrile patients. Glucocorticoid may be beneficial in case of severe complications, associated autoimmune disorders, or severe and persistent symptoms despite NSAID treatment.10,11 The thyroid dysfunction was aptly addressed with levothyroxine, stabilizing the patient’s thyroid status. This approach underscores the need for individualized treatment strategies in KFD, especially when coexisting conditions such as thyroiditis are present.
While the prognosis of KFD is generally favourable, with symptom duration ranging from 1 to 4 months, the mortality rate is 2.1%, primarily associated with hemophagocytic syndrome or connective tissue disorders.4,12 Additionally, the rate of autoimmune development in children is 4%. 6 The potential for developing subsequent autoimmune conditions necessitates vigilance in the post-recovery period.
The concurrence of KFD with Hashimoto thyroiditis in our patient is notable. Literature suggests a possible autoimmune predisposition in KFD patients, with a subset developing diseases like SLE and Sjögren’s syndrome. 3 The high TPO-Ab concentration post-recovery suggests that our patient’s thyroiditis was not a transient inflammatory response but indicative of an underlying autoimmune process. The temporal association between KFD and the emergence of autoimmune conditions may imply a potential shared pathogenic mechanism, warranting further investigation into the immune dysregulation that might underpin both disorders.
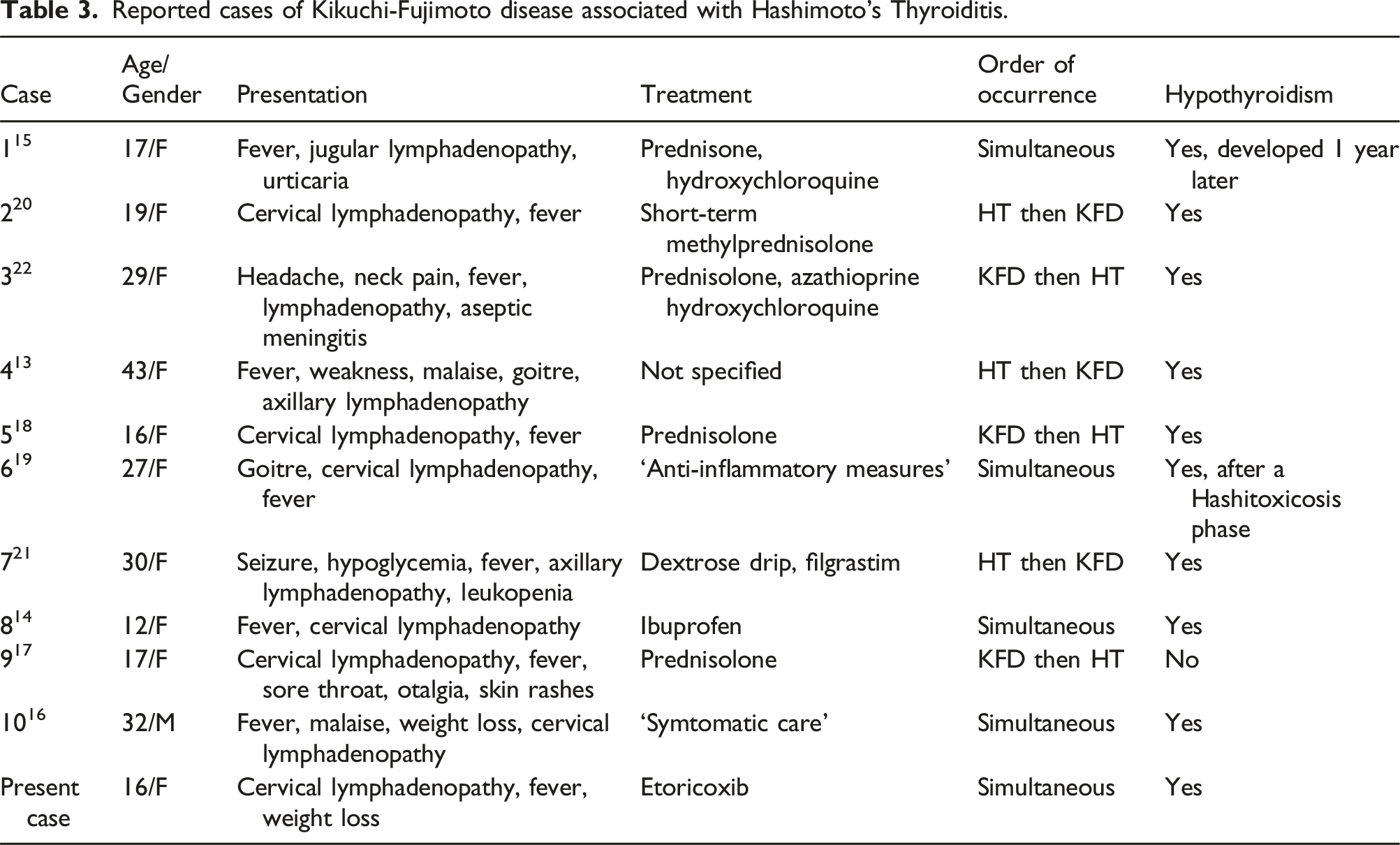
To the best of our knowledge, there have been 10 case reports of KFD associated with Hashimoto’s thyroiditis, with broad clinical spectrum, as shown in Table 3.13–22 Consistent with most previous cases, KFD occurred simultaneously with Hashimoto’s thyroiditis in our patient. The treatment approaches across the cases are mainly symptomatic relief, including the use of NSAIDs (such as etoricoxib in the present case), corticosteroids, and immunosuppressants (azathioprine in one case due to co-occurrence with systemic lupus erythematosus), reflecting a tailored approach based on the severity of symptoms and the presence of coexisting autoimmune diseases. Most cases, including the present one, report the development of hypothyroidism, necessitating ongoing thyroid hormone replacement therapy. This outcome highlights the importance of long-term follow-up for patients with KFD, given the potential for developing or unmasking underlying autoimmune thyroid disorders.
The presented case can indicate several critical clinical implications. Firstly, KFD should be considered in the differential diagnosis of lymphadenopathy, especially in young patients. This underscores the need for a thorough evaluation, including biopsy, when common infectious, autoimmune, and malignant causes are excluded. Secondly, the concurrent diagnosis of KFD and Hashimoto thyroiditis in this patient suggests a potential link between KFD and autoimmune conditions. Clinicians should be vigilant for signs of autoimmune diseases in patients diagnosed with KFD and consider monitoring for the development of conditions such as Hashimoto thyroiditis, SLE and Sjögren’s syndrome. Next, long-term follow-up is crucial for patients diagnosed with KFD due to the potential for developing autoimmune disorders post-recovery. Finally, understanding the typical presentation of KFD, including cervical lymphadenopathy and prolonged fever, can aid in early diagnosis and appropriate management. Recognizing the disease’s self-limiting nature can prevent unnecessary prolonged antibiotic use, as seen in this case where antibiotics were discontinued after the KFD diagnosis.
Reported cases of Kikuchi-Fujimoto disease associated with Hashimoto’s Thyroiditis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The participant provided informed consent for the study.
Guarantor
HCD.
Contributorship
All authors contributed to the content and approach of the paper. Hung Cao Dinh conducted the literature review, drafted the paper, and corrected the language. Dung Ngoc Doan, Si Luc Nguyen, and Trung The Tran conducted the literature review. Khanh Quang Tran wrote the paper. All authors have read and agreed to the manuscript as written.