
Abstract
Background
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system. Diagnosis is based on the 2017 revised McDonald criteria. Unmatched oligoclonal bands (OCB) within the CSF (i.e. positive OCB) can substitute for dissemination in time by magnetic resonance imaging (MRI). Simonsen et al. (2020) claimed a raised (>0.7) immunoglobulin G (IgG) index could replace OCB status. This study aimed to establish the diagnostic utility of IgG index for MS in the population served by The Walton Centre NHS Foundation Trust (WCFT) a neurology and neurosurgery hospital, and to derive a population-based IgG index reference interval.
Methods
OCB results from the laboratory information system (LIS) were collated from November 2018 to 2021. Final diagnosis and medication history was obtained from the electronic patient record. Exclusions were made based on age (<18 years) at the time of lumbar puncture (LP) disease-modifying treatment prior to LP, unknown IgG index and unclear OCB patterns.
Results
935 of 1101 results remained following exclusions. 226 (24.2%) had a diagnosis of MS, 212 (93.8%) were OCB positive and 165 (73.0%) had a raised IgG index. The diagnostic specificity of a raised IgG index was calculated at 90.3% compared to 86.9% for positive OCB. 386 results with negative OCB were used to establish the IgG index reference interval (0.36–0.68) at 95th percentiles.
Conclusion
This study provides evidence that IgG index should not replace OCB in the diagnosis of MS. >0.7 is an appropriate cut-off to define a raised IgG index for the patient population.
Introduction
Multiple sclerosis (MS) is a common cause of non-traumatic disability. UK prevalence in 2020 was reportedly 190 cases per 100,000. 1 The prevailing type of MS, relapsing remitting, typically presents in the 3rd decade of life. 2 Aetiology is unknown, risk factors include sex (females are affected twofold), vitamin D deficiency, smoking, obesity, extremes of latitude and affected relatives. 3 Demyelination results from the infiltration of B lymphocytes across the blood brain barrier which differentiate into plasma cells with autonomous immunoglobulin G (IgG) secretion. 3
The evidence required for diagnosis differs depending on clinical history and number of symptomatic episodes. Diagnosis is based on the 2017 revised McDonald criteria, which includes the use of positive IgG oligoclonal bands (OCB) as a substitute for dissemination in time by magnetic resonance imaging (MRI). 4 Positive OCB, that is, CSF bands unmatched within the serum, are suggestive (reported sensitivity 88%) but not specific for MS. 5 IgG index is reported alongside OCB and is calculated from serum and CSF concentrations of albumin and IgG, using the following equation: CSF IgG (g/L) x serum albumin (g/L)/serum IgG (g/L) x CSF albumin (g/L). A raised IgG index (>0.7) is suggestive of an inflammatory CNS condition, for example, MS, but it is not currently used diagnostically.
A retrospective study performed by Simonsen et al. reported that a raised IgG index had a positive predictive value (PPV) of >99% for positive OCBs. They concluded that ‘a positive IgG index can therefore replace OCB and thus lead to an earlier diagnosis’. 6 This study was driven by the 2/3-week turnaround time (TAT) for OCB, compared to 24 h for IgG index. Earlier diagnoses facilitate prompt initiation of disease-modifying therapies (DMTs), associated with improved patient outcomes including reduced disability accumulation.6–8
We performed a retrospective observational study to determine if the findings of Simonsen et al. correlated with the patient population of Walton Centre NHS Foundation Trust (WCFT), a neurology and neurosurgery hospital based in the North West of England serving 3.5 million individuals, and to verify 0.7 as a cut-off to define a raised IgG index.
Materials and methods
Data collection
OCB results were obtained from the laboratory information system (LIS), between 1 November 2018 and 26 November 2021. The final diagnosis and medication history were obtained from the electronic patient record. Patients were excluded if prior to lumbar puncture (LP) they were younger than 18 years of age or on DMTs. OCB results without paired CSF IgG index and unclear OCB patterns were also excluded. For patients with multiple OCB results only the baseline was included. The study was approved by the Clinical Audit committee of the WCFT. Written informed consent was not required as the study was observational, and the OCB and IgG index were requested as part of the routine diagnostic investigations.
Instruments and reagents
OCB were detected by an in-house isoelectric focusing with immunodetection method. 9 OCB status was recorded as a T1–T6 pattern. Positive OCB was defined as ≥ 2 unmatched CSF bands.
Serum and CSF IgG and CSF albumin were measured by immunonephelometry and immunoturbidimetry, respectively, with a semi-automated Siemens BN Prospec using Siemens reagents and calibrators. Serum albumin was measured by bromocresol green colourimentry with a Roche Cobas C 311 using Roche reagents and calibrators.
IgG index was automatically calculated by the LIS on paired serum and CSF. A raised IgG index was defined as >0.7.
Data analysis
Sensitivity, specificity, PPV and negative predictive value (NPV) were calculated using Microsoft Excel 2010. Independent paired t-test was performed to assess significant differences between median IgG values in separate populations.
Results
1101 OCB results were identified, 935 were included.
Immunoglobulin G index reference interval
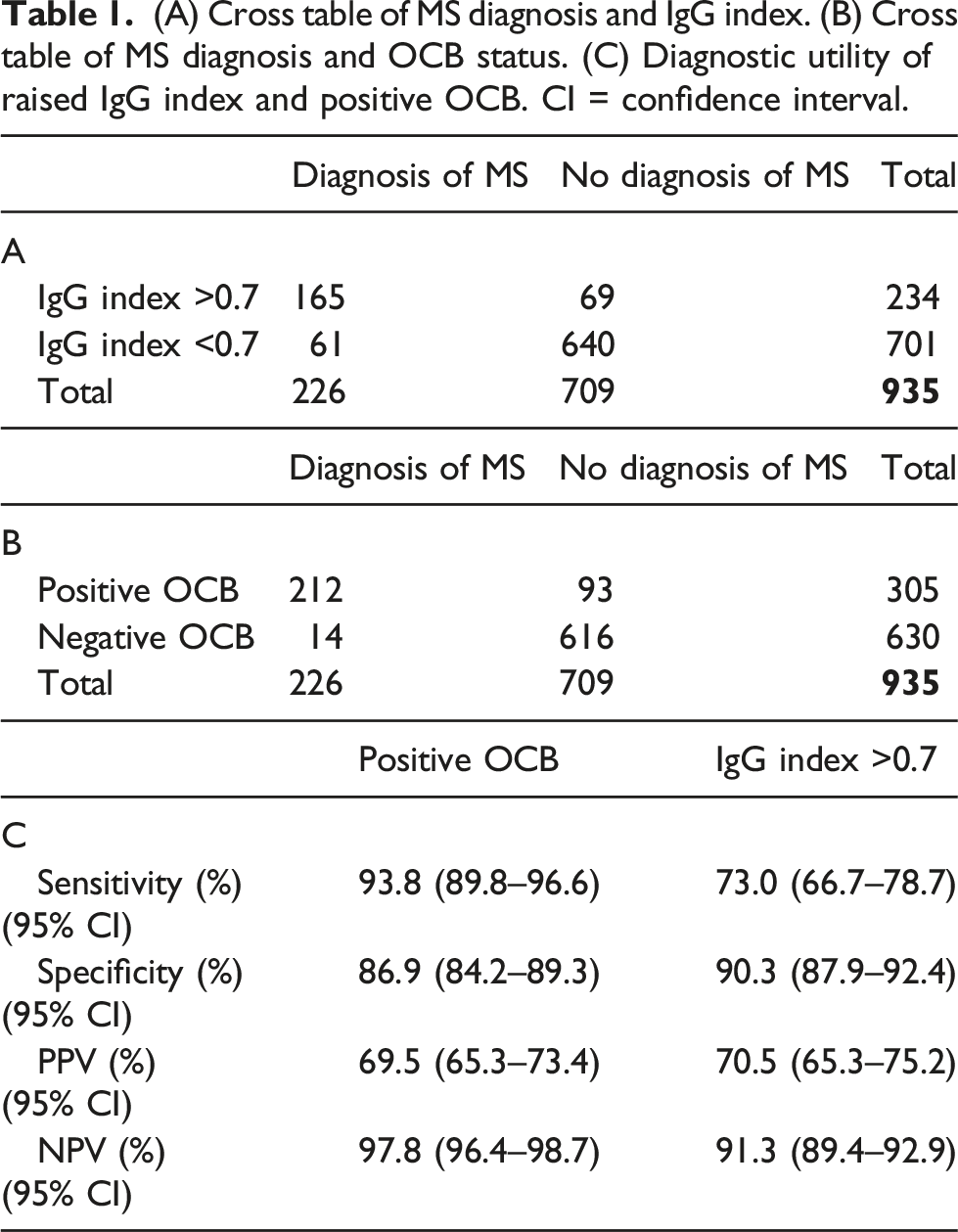
(A) Cross table of MS diagnosis and IgG index. (B) Cross table of MS diagnosis and OCB status. (C) Diagnostic utility of raised IgG index and positive OCB. CI = confidence interval.
Immunoglobulin G index diagnostic utility
226 (24.2%) patients had a diagnosis of MS, of these 212 (93.81%) were OCB positive. The ratio of F to M was 2.21:1. The median IgG index was raised: 0.99 (F), 0.74 (M). The sensitivity, specificity, PPV and NPV of IgG Index >0.7 and positive OCB was calculated (Table 1). Of the 14 patients with MS and negative OCB only one patient had IgG index >0.7.
Discussion
The calculated diagnostic sensitivity of positive OCB (93.8%) was consistent with reports in the literature. The sensitivity of raised IgG index was lower (73.0%) and would miss approximately 20% of diagnoses in comparison to OCB. The calculated diagnostic specificity for both markers was >85%, reinforcing the importance of interpreting these results alongside other investigations.
The calculated PPV for raised IgG index was significantly lower than reported by Simonsen et al., we also calculated a higher NPV. PPV and NPV are affected by disease prevalence. The study performed by Simonsen et al. had a MS prevalence of 100%, in comparison to our study where the prevalence was 24%. The PPV and NPV calculated by Simonsen et al. were therefore skewed and not representative for the use of the test in the general population. Furthermore, TAT of OCB at WCFT is 5 days, far quicker than reported in Norway. Initiation of DMTs would not be delayed by waiting for OCB results.
Limitations of this study include the data collection. Medication history relied upon accurate EPR information. In some instances limited information was available, patients may have been on medications warranting exclusion but no record was apparent.
In conclusion, 0.7 is an appropriate cut-off to define an elevated IgG index for the WCNN patient population. Positive OCB has a superior diagnostic sensitivity and NPV for MS in comparison to raised IgG index for the general population as such IgG index should not replace OCB analysis. Furthermore, IgG index does not provide diagnostic evidence of MS in patients who are OCB negative. We conclude calculation of IgG index is not diagnostically useful for the investigation of MS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Clinical Audit committee of the WCFT.
Guarantor
FS.
Contributorship
CC conceived the study. FS collected and interpreted the data. FS wrote the draft article. CC and FS revised the draft article for submission.