
Abstract

The reference method for measuring low density lipoprotein cholesterol (LDL-C) is beta quantification, which requires ultracentrifugation of plasma to fractionate lipoprotein classes. This requires specialist equipment and expertise that is not available in most routine laboratories and so is not widely used in practice. Automated homogenous assays for the direct measurement of LDL-C are also available, but the use of a calculation to estimate LDL-C concentrations remains standard practice in most clinical laboratories. Historically, the most widely used equation for the calculation of LDL-C is the Friedewald equation. This equation was established in 1972 1 and estimates LDL-C using total cholesterol (TC), high density lipoprotein cholesterol (HDL-C) and triglycerides (TG). While the original study suggested that Friedewald LDL-C generally agrees well with beta quantification LDL-C, Friedewald has significant limitations. The equation assumes that the ratio of total TG to very low density lipoprotein cholesterol (VLDL-C) is the same in all subjects (molar ratio of 2.2:1) and also that the amount of cholesterol and TG in chylomicrons is negligible. This means that the use of Friedewald is not recommended in non-fasting samples or where TG is greater than 4.5 mmol/L (400 mg/dL) as these assumptions are less likely to be valid. Some reports have suggested that the Friedewald equation may have limited accuracy even in samples satisfying these conditions, particularly at lower LDL-C concentrations. 2 Widely used cardiovascular risk calculations include non-HDL cholesterol (NHDL-C) rather than LDL-C (e.g JBS3, QRISK3), but LDL-C estimations remain important in some situations. For example, NICE guidance on the prescription of injectable PCSK9 inhibitors in patients with sub-optimal control of hypercholesterolaemia using traditional lipid-lowering therapy recommends criteria that include LDL-C thresholds to determine eligibility for treatment. 3 In our centre we have experienced an increased demand for direct measurements of LDL-C in potential candidates for PCSK9 inhibitor therapy, either because the patient has raised TG or there is concern that inaccuracy of Friedewald LDL-C may be influencing the decision whether to treat. Our laboratory is one of the few in the UK with access to a beta quantification method allowing direct measurement of LDL-C, but this method is time-consuming, relatively expensive and low-throughput. Automated homogenous LDL-C methods are an alternative, but these assays also come with an additional cost compared to calculation of LDL-C.
Several alternative equations for the calculation of LDL-C, that appear to offer improved accuracy relative to Friedewald have been described in the literature such as those established by Anandaraja et al.,
4
Chen at al
5
and de Cordova et al.
6
Two of the most prominent, widely discussed equations are those published by Martin et al.
7
and Sampson et al.
8
Both equations attempt to improve the estimation of LDL-C compared to the Friedewald equation by varying the assumed TG to VLDL-C ratio according to the TG and NHDL-C concentration, rather than applying a constant ratio regardless of TG or NHDL-C. The Martin equation was derived from a large dataset (n=900,605) using an ultracentrifugation method as a reference. The equation derived by Martin et al. applies a TG to VLDL-C ratio that varies according to TG and NHDL-C (it is based on mass units)

A factor from a 180-cell table is applied, which is selected based on 180 possible combinations of TG and NHDL-C concentrations. For example, a lower TG to VLDL-C ratio is assumed when NHDL-C is elevated and TG low, compared to when NHDL-C is low and TG elevated. The original study suggested that the Martin equation provides a more accurate estimate of LDL-C than the Friedewald equation at lower LDL-C concentrations, particularly when TG is greater than 1.7 mmol/L. A disadvantage of the Martin equation, however, is that it may not be straightforward to incorporate into a LIMS due to its reliance on the selection of the appropriate TG to VLDL-C ratio. The equation would have to be adjusted to produce values in molar units. In this issue of the Annals of Clinical Biochemistry, Ishida et al. present a validation study comparing LDL-C calculated using the Martin equation to LDL-C measured using a direct, homogenous LDL-C assay. 9 The authors have also derived a simpler, ‘modified Martin’ equation, which reduces the number of factors for the TG to VLDL-C ratio from 180 to only 12 factors for different combinations of TG and NHDL-C. The aim of deriving this simpler formula was to develop an equation that would be more suitable for routine use in a clinical LIMS while maintaining the advantage of improved accuracy relative to Friedewald. Ishida et al. found that the Martin equation provided improved correlation with direct LDL-C measurements compared to Friedewald, with Friedewald underestimating LDL-C in a larger proportion of patients. The modified Martin equation derived by the authors also appeared to offer improved agreement with direct LDL-C compared to Friedewald when TG is <4.5 mmol/L (400 mg/dL). However, with TG greater than 4.5 mmol/L, agreement with direct LDL-C was poorer for all three equations, although Martin and modified Martin equations fared better than Friedewald.
The Sampson equation differs from the Martin equation in that it is a single equation rather than an equation with a variable factor, which might make this equation simpler to implement in routine practice
6
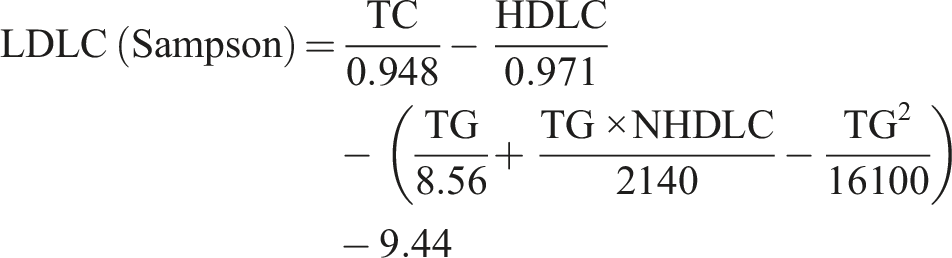
Like the Martin equation, this is based on mass units so requires adjustment if it is to be used with lipid values in molar units. The Sampson equation was derived using beta quantification LDL-C values in 8656 patients using multiple least squares regression analysis and validated with a large external beta quantification data set of 27,646 samples. An advantage of the Sampson equation over the Friedewald and Martin equations is that agreement with beta quantification LDL-C remained strong at TG concentrations up to 9 mmol/L (the mean absolute difference between calculated and measured LDL-C was significantly lower for Sampson than Martin and Friedewald when TG concentrations were over 4.5 mmol/L). Several independent studies comparing the Martin and Sampson equations to direct LDL-C measurements have also concluded that the Martin and Sampson equations are more accurate than Friedewald in patients with normal or elevated triglycerides.10-12
The Friedewald equation has been in use for decades, yet its limitations are well known. Given the significant amount of evidence for improved accuracy of LDL-C estimates using alternative equations it may seem surprising that Friedewald has remained the standard equation for estimating LDL-C for so long. One of the major reasons for the persistence of the Friedewald equation may be that Friedewald has been used in many large clinical trials of lipid lowering therapies leading to its inclusion in the resulting guidelines. Newer formulae such as the Martin and Sampson equations perform better then the Friedewald equation according to a number of independent studies. 50 years on from the original Friedewald et al. paper, perhaps it is time to seriously consider introducing a more reliable equation for calculation of LDL-C into routine practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
CB.
Contributorship
CB and AL wrote the article.