
Abstract
Higher levels of serum alkaline phosphatase (ALP) as a novel risk factor was recently found associated with mortality in different population, whereas, the relationship remains unknown in hypertrophic cardiomyopathy (HCM) population. In this study, we hypothesized that increased ALP could predict all-cause mortality in the adult HCM population. In this cohort study, retrospective data from 538 HCM patients consecutively recruited in West China Hospital were collected. Patients were divided into two groups by baseline ALP with 80 IU/L as the cutoff. All-cause mortality was set as the endpoint. Subgroup analysis was conducted in patients with normal liver function. In total, 461 adult HCM patients were included. After a median follow-up of 4.7 years, 91 patients died. Alkaline phosphatase was an independent predictor of all-cause mortality since patients in the higher ALP group had an increased risk (adjusted HR 2.0, 95% CI: 1.3–3.3, P < 0.01) compared with those in the lower ALP group. In subgroup analysis, the relationship was consistent with the overall (adjusted HR: 3.0, 95% CI: 1.7–5.3, P < 0.01 for the higher ALP group). In the Chinese cohort study of HCM patients, serum ALP is independently associated with all-cause mortality. Patients with a measured value above 80 IU/L had an increased risk of all-cause mortality and this cutoff might help with risk stratification in HCM population.
Introduction
Hypertrophic cardiomyopathy (HCM) is defined by the presence of increased left ventricular wall thickness that is not solely explained by abnormal loading conditions. 1 It is inherited as an autosomal dominant genetic trait and is a common genetic disorder of the myocardium, with a population prevalence ratio of approximately 1:500.1,2 Hypertrophic cardiomyopathy is extremely heterogeneous concerning clinical onset and manifestation, phenotype, as well as clinical course. 3 Historically, a highly unfavourable and generally poor prognosis due to sudden cardiac death (SCD) and complications of heart failure was thought associated with HCM,4,5 while contemporary studies showed that the prognosis for most HCM individuals has improved, particularly when it is managed in line with current clinical practice guidelines. 5 Even so, some of them are also faced with profound exercise limitations, recurrent arrhythmias and premature death in the progression of the disease.4,6 A recent study revealed that HCM conveyed excess mortality when compared with the general population through the life course. 7
Alkaline phosphatases (ALPs) are a family of enzymes that catalyze the hydrolysis of organic phosphate esters in an alkaline environment. 8 Four genes encode ALP isozymes in humans, including the tissue-specific intestinal, placental, germ cell ALPs, and tissue-nonspecific isozyme existing in several tissues such as bone, liver and kidney. 9 Recently, higher levels of ALP were found to be associated with an increased risk of all-cause mortality in the general population,10,11 survivors of myocardial infarction, 11 stroke survivors 12 and patients with chronic kidney disease.13,14 However, there is a lack of study on the relationship in the HCM population. Therefore, this study aimed to explore whether ALP could be useful in predicting mortality in patients with HCM in a retrospective cohort of hospitalized patients.
Materials and methods
Study population
This cohort was from a retrospective, single-centre, longitudinal study. A total of 538 unrelated HCM patients were consecutively collected in the inpatient department of cardiology, West China Hospital of Sichuan University (Chengdu, China), between December 2008 and March 2018 (Figure 1). Patients with myocardial hypertrophy secondary to other diseases were not included. Study flow diagram. Five hundred and thirty-eight patients were diagnosed with HCM from December 2008 to March 2018. After excluding those with invalid data (n = 29) and those under 18 years old (n = 5), the remaining 504 patients were enrolled in the study. Due to 43 patients lost to follow-up, eventually, 461 patients with complete information were included in the present analysis. HCM: hypertrophic cardiomyopathy.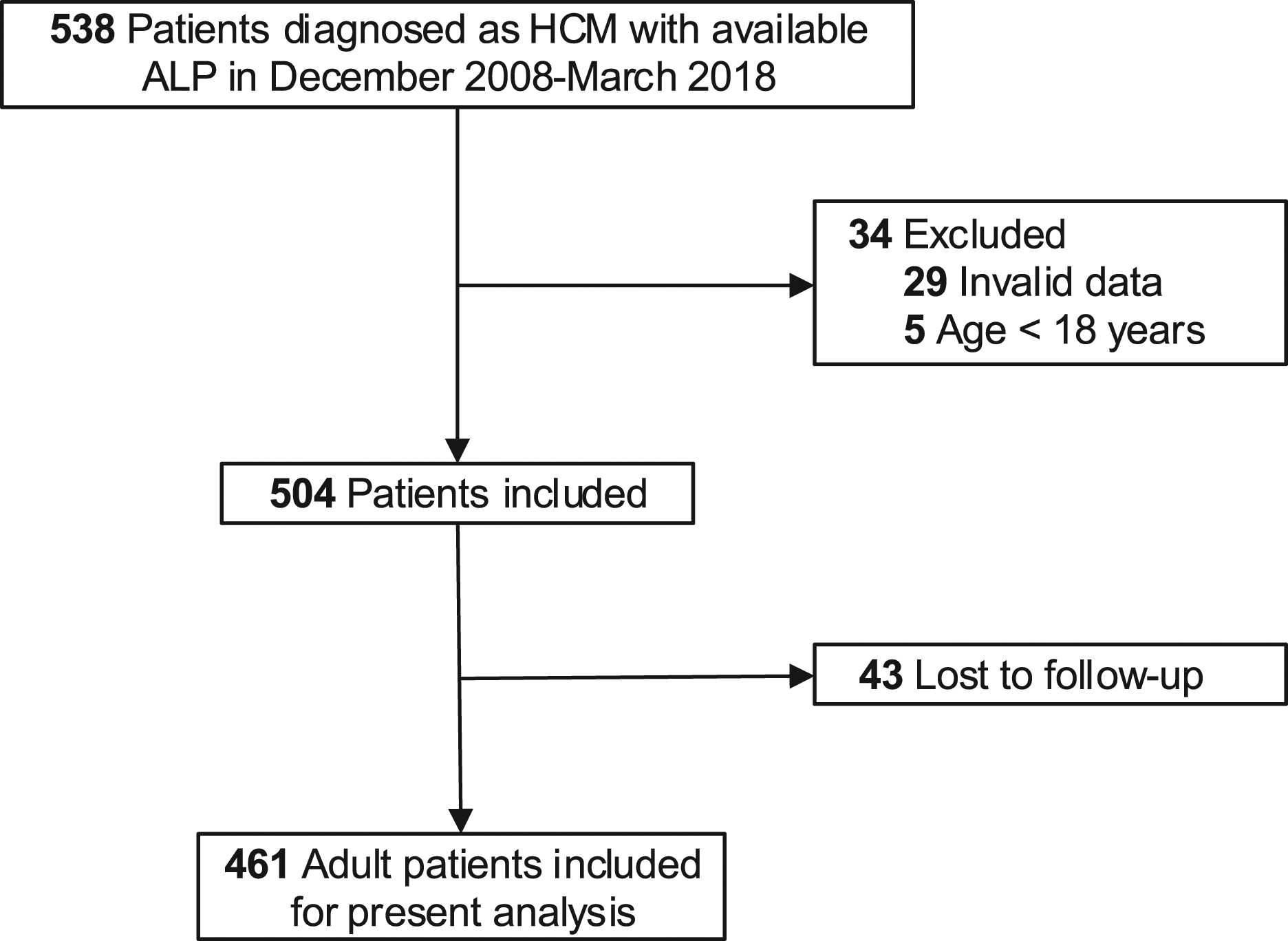
Inclusion criteria were based on the 2014 guidelines of the European Society of Cardiology that HCM was defined as a wall thickness ≥ 15 mm (or ≥13 mm for patients with a family history of HCM) in any left ventricle myocardial segments, as measured by echocardiography or cardiac magnetic resonance imaging (MRI), and that was not solely explained by abnormal loading conditions. 1 Patients under 18 years old (n = 5) or with invalid baseline data (n = 29) were excluded. Due to loss to follow-up, 43 patients (8.53%) were excluded from the final analysis (Figure 1). We compared the baseline characteristics between the patients lost to follow-up and those included in the final analysis, and no statistical difference was found (data not !their admission to the inpatient department, all the patients received medical history collection and systematic examinations, including physical examination, 12-lead electrocardiogram, ultrasonic cardiogram, and laboratory examinations. Complying with the principles of the Declaration of Helsinki, the study was approved by the Biomedical Research Ethics Committee, West China Hospital of Sichuan University (approval number: 2019–1147), and registered with www.chictr.org.cn (registration ID: ChiCTR2000029352). Due to the retrospective nature of the study, individual patient consent was not required. Other detailed information about those patients could be accessed elsewhere.15–17
Data collection and measurement
Experienced physicians collected all baseline characteristics from medical records in twice-entry method. When the values of the two entries were consistent, the data would enter the database otherwise be checked.
At baseline, the whole cohort underwent a standard two-dimensional transthoracic echocardiography following the recommendations of the American Society of Echocardiography -European Association of Echocardiography. 18
Blood specimens for ALP values at the time of hospital admission were performed utilizing a Cobas 8000, and the normal range in this system is 51–160 IU/L. Patients were divided into two groups according to their baseline ALP with 80 IU/L as the cutoff. A previous study 11 focusing on the prognostic significance of ALP found that ALP ≥ 80 IU/L was associated with a higher risk of adverse outcomes in participants with a previous myocardial infarction. Similarly, increased mortality was also found in patients with ALP ≥ 80 IU/L in the chronic kidney disease population. 14
Endpoint events and follow-up
The primary endpoint was set as all-cause mortality. Follow-up was performed by clinical consultations, medical records, and telephone interviews, and it extended from the first evaluation until the date of an endpoint or the administrative censoring date, set on February 7, 2020. All data were corroborated with hospital records.
Statistical analysis
Data are presented as mean (±SD) for normally distributed variables or median (IQR) for skewed variables, and number (n) and percentage (%) for categorical variables. Differences in baseline characteristics between groups were tested by independent two-sample t-tests for normally distributed variables or by Wilcoxon rank-sums tests for skewed variables. Interactions between categorical variables were evaluated with the chi-square or Fisher’s exact test as appropriate. Spearman correlation or Pearson correlation was used to determine the correlations between ALP and other variables.
A Kaplan–Meier analysis with a log-rank test was used for the univariable analysis. In light of the relatively small sample and limited cases, variables for inclusion were carefully chosen to ensure parsimony of the multivariable models. Age and gender were forced into the multivariable models, and other variables that showed a univariable relationship (p < 0.1) were chosen into multivariable models to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) to explore the association between ALP level and risk of death. Six multivariable models were constructed: (1) Model 1, the basic model, adjusted for age and gender; (2) Model 2 adjusted for Model 1, medical history including chronic obstructive pulmonary disease, prior thromboembolism events, New York Heart Association III/IV and atrial fibrillation; (3) Model 3 adjusted for Model 1 and treatment including warfarin, beta-blockers and diuretics; (4) Model 4 adjusted for Model 1 and laboratory values including direct bilirubin (DBil), aspartate aminotransferase (AST), urea nitrogen, creatinine, cystatin C, uric acid, triglyceride, cholesterol, and low density lipoprotein cholesterol (LDL-C); (5) Model 5 adjusted for Model 1 and echocardiographic data including left atrium (LA), left ventricular end-diastolic dimension (LVEDD), left ventricular posterior wall and ejection fraction (EF). For the final Model 6, the predictors were sought using a forward stepwise modelling approach (p = 0.05 for inclusion, p = 0.10 for exclusion) including all variables from Model 1–5.
After fitting a Cox proportional hazard regression model, time-varying coefficients were identified in case of the rejection of the null hypothesis by testing the proportional hazards assumption with the help of the cox.zph() function shipped with the survival package or Schoenfeld’s global test in R-program. Time-dependent multivariable adjusted Cox proportional hazards models were constructed in situations when the effect of the covariate is time-varying with the proportional hazards assumption of the Cox regression model not holding. 19
Restricted cubic spline curves with 4 knots at the 5th, 35th, 65th, 95th percentiles of ALP were used to visualize the relationship between ALP and all-cause mortality on a continuous scale based on aforementioned Model 6. 20
Elevated serum ALP usually reflects some hepatic disease in clinical practice. Mild to moderate elevation of ALP can be seen in all types of liver disorder. 21 To eliminate the confounding effects caused by abnormal liver function as much as possible, we excluded 64 patients with abnormal DBil, indirect bilirubin (IBil), AST or alanine aminotransferase (ALT) to conduct subgroup analysis in the remaining 397 patients.
R version 3.6.3 was used for statistical analysis. All reported P values are two-sided and differences were considered statistically significant at P ≤ 0.05.
Results
Baseline characteristics
Baseline characteristics of patients with hypertrophic cardiomyopathy between ALP groups.
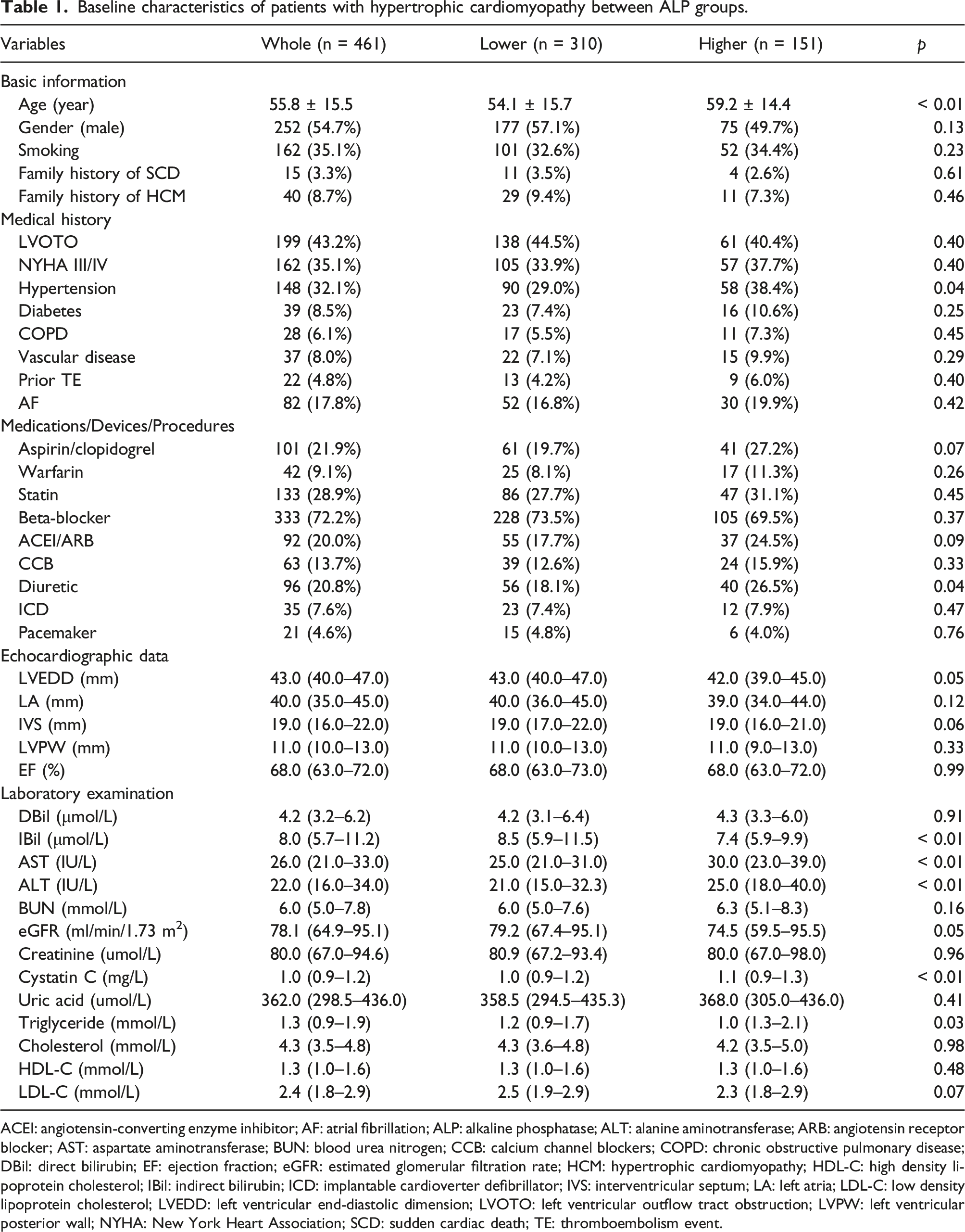
ACEI: angiotensin-converting enzyme inhibitor; AF: atrial fibrillation; ALP: alkaline phosphatase; ALT: alanine aminotransferase; ARB: angiotensin receptor blocker; AST: aspartate aminotransferase; BUN: blood urea nitrogen; CCB: calcium channel blockers; COPD: chronic obstructive pulmonary disease; DBil: direct bilirubin; EF: ejection fraction; eGFR: estimated glomerular filtration rate; HCM: hypertrophic cardiomyopathy; HDL-C: high density lipoprotein cholesterol; IBil: indirect bilirubin; ICD: implantable cardioverter defibrillator; IVS: interventricular septum; LA: left atria; LDL-C: low density lipoprotein cholesterol; LVEDD: left ventricular end-diastolic dimension; LVOTO: left ventricular outflow tract obstruction; LVPW: left ventricular posterior wall; NYHA: New York Heart Association; SCD: sudden cardiac death; TE: thromboembolism event.
Endpoints and survival analysis
After a median follow-up of 4.7 years (ranging: 0.1–10.8) and observation of 2156 person-years, 91 patients (19.8%) died, 46 of them were in higher ALP group. Compared with the rate of mortality in lower ALP group (3.0 per 100 person-years, 95% CI: 2.1–3.9), it was greater in higher ALP group (7.1 per 100 person-years, 95% CI: 5.1–9.0, p < 0.01). The causes of death consisted of heart failure (n = 26), SCD (n = 24), stroke (n = 12), myocardial infarction (n = 2), perioperative death (n = 2), cancer (n = 9), bleeding (n = 2), accidents (n = 4), and others (n = 12) including pulmonary disease, renal disfunction, diabetes, injury and peripheral neuropathy.
Kaplan–Meier curves show gradually increased cumulative incidence of all-cause mortality (log-rank p < 0.01) in higher ALP group during the follow-up (Figure 2). Univariable analyses of all-cause mortality are shown in Supplemental Table 1. Cumulative incidences of all-cause mortality between ALP groups during follow-up in HCM patients. Kaplan–Meier curves show patients with ALP ≥ 80 IU/L had significantly higher cumulative incidence of all-cause mortality during follow-up than those with ALP < 80 IU/L. HCM: hypertrophic cardiomyopathy; ALP: alkaline phosphatase.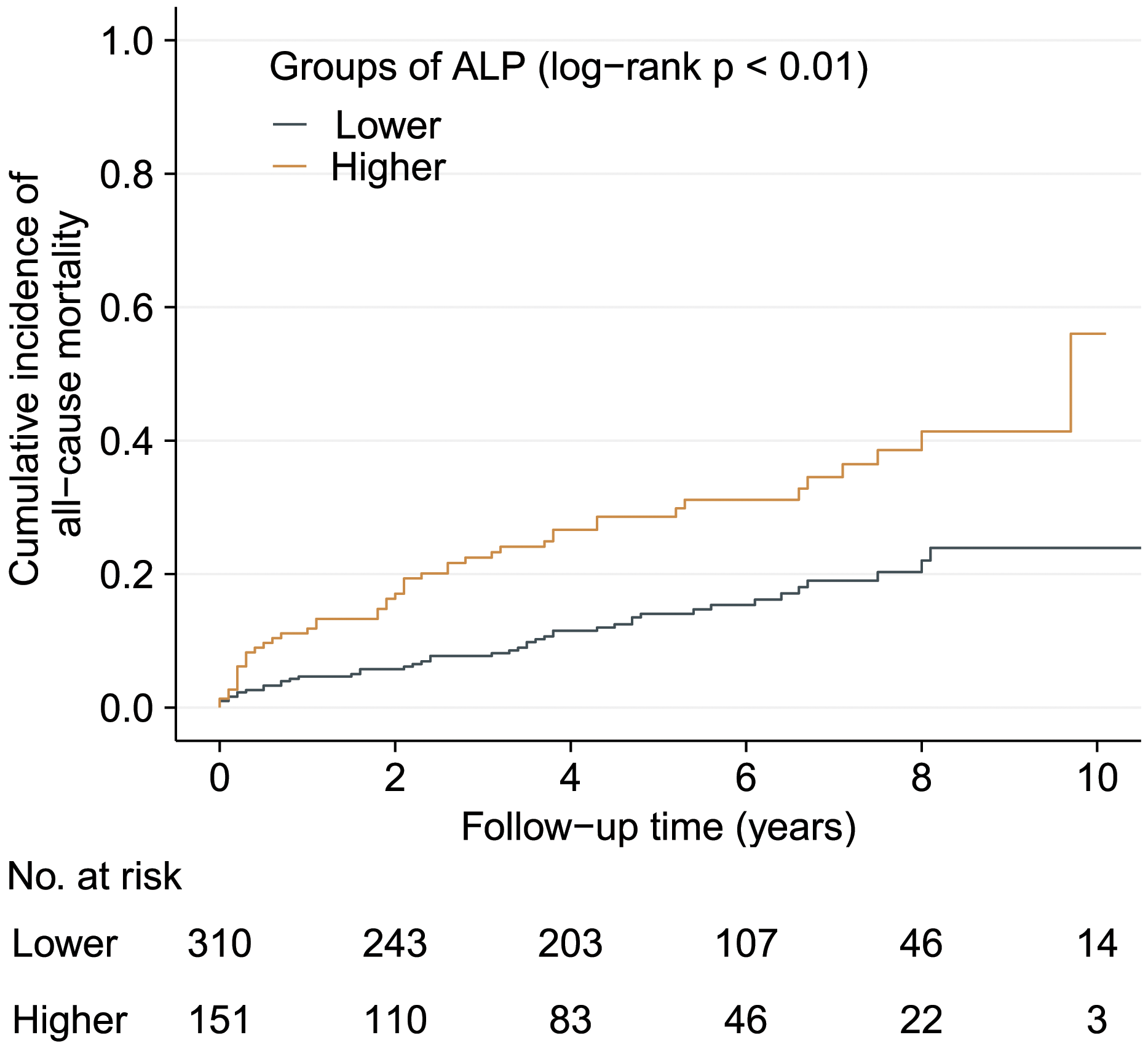
Associations of ALP with all-cause mortality.
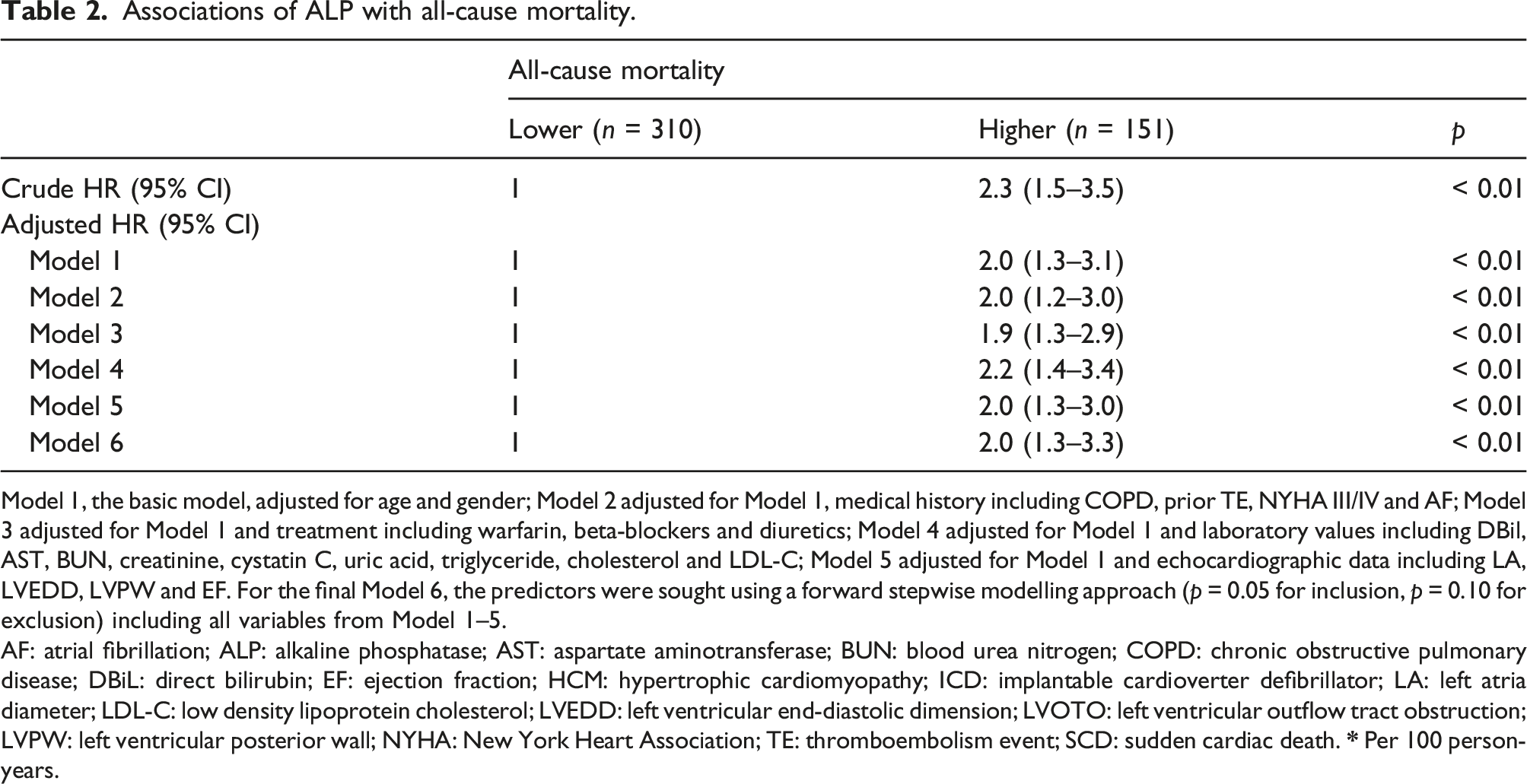
Model 1, the basic model, adjusted for age and gender; Model 2 adjusted for Model 1, medical history including COPD, prior TE, NYHA III/IV and AF; Model 3 adjusted for Model 1 and treatment including warfarin, beta-blockers and diuretics; Model 4 adjusted for Model 1 and laboratory values including DBil, AST, BUN, creatinine, cystatin C, uric acid, triglyceride, cholesterol and LDL-C; Model 5 adjusted for Model 1 and echocardiographic data including LA, LVEDD, LVPW and EF. For the final Model 6, the predictors were sought using a forward stepwise modelling approach (p = 0.05 for inclusion, p = 0.10 for exclusion) including all variables from Model 1–5.
AF: atrial fibrillation; ALP: alkaline phosphatase; AST: aspartate aminotransferase; BUN: blood urea nitrogen; COPD: chronic obstructive pulmonary disease; DBiL: direct bilirubin; EF: ejection fraction; HCM: hypertrophic cardiomyopathy; ICD: implantable cardioverter defibrillator; LA: left atria diameter; LDL-C: low density lipoprotein cholesterol; LVEDD: left ventricular end-diastolic dimension; LVOTO: left ventricular outflow tract obstruction; LVPW: left ventricular posterior wall; NYHA: New York Heart Association; TE: thromboembolism event; SCD: sudden cardiac death.
In Figure 3, with the cutoff of ALP at 80 IU/L as the reference, there was an overall positive association (p for nonlinearity: 0.11) between measured ALP values and all-cause mortality after adjusting potential covariates in Model 6: below 80 IU/L, the risk of all-cause mortality increased remarkably with ALP value rising, while above 80 IU/L, the risk increased moderately and then inclined to stable. Visual associations between ALP and all-cause mortality. Restricted cubic spline analysis was used to visualize the relationship between ALP and all-cause mortality after adjustment for covariates. Reference point was the cutoff at 80 IU/L. Dotted line represents HR at 1. ALP: alkaline phosphatase.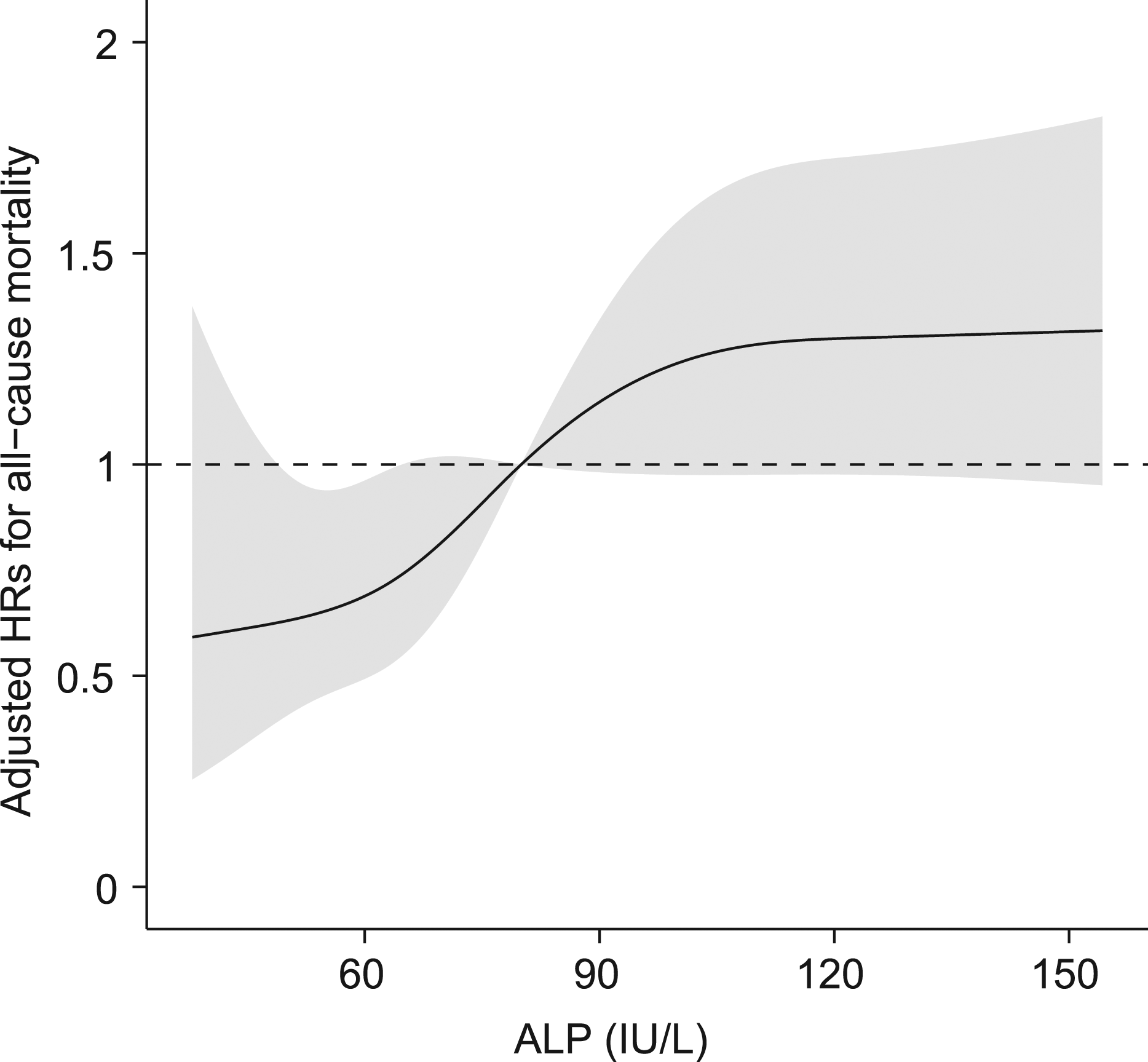
Subgroup analysis
In the patients with DBil, IBil, AST and ALT measured in normal ranges, the results turned out to be similar to the whole. Sixty nine out of 397 patients died. All-cause mortality rates were 2.8 (95% CI: 1.9–3.7) and 5.9 (95% CI: 3.9–7.9) per 100 person-years in lower ALP group and higher ALP group, respectively (p < 0.01). Kaplan–Meier curves demonstrate significantly different cumulative incidences of all-cause mortality between groups (log-rank p < 0.01, Supplemental Figure 1), with the higher ALP group remaining to be associated with increased risk. Multivariable analysis shows that after adjusting covariates, the patients in higher ALP group had a 3-fold risk (adjusted HR: 3.0, 95% CI: 1.7–5.3, p < 0.01) of all-cause mortality (data not shown).
Discussion
This is the first study to assess the prognostic significance of ALP in adult HCM patients. The main finding of the present study was that ALP was associated with all-cause mortality in HCM patients. The patients with measured ALP above 80 IU/L were at greater risk of all-cause mortality than those with ALP below 80. Furthermore, subgroup analysis excluding patients with abnormal liver function came to the robust results.
In clinical settings, elevated serum ALP is routinely related to bony or hepatic disease or cancer. Recently, the focus on ALP as an emerging risk factor for mortality is novel in the general population, dialysis patients, survivors of myocardial infarction and patients suffering from stroke.10–14,22 Our findings kept in line with the previous studies, indicating possible pathophysiological insights and useful prognostic significance of ALP in HCM patients.
In those HCM deaths, it turned out that there were extensive areas of ischemic myocardial damage, including a chronic post-necrotic replacement-type fibrosis. 23 Fibrosis is an integral component of most cardiac pathological conditions and can be associated with cardiomyocyte death, pressure or volume overload, and HCM. 24 In the fibrotic heart, tissue-nonspecific ALP was found upregulated, and it could be depressed by insulin-like peptide 6, indicating a role in fibrosis.25,26 Additionally, lung ALP has also emerged as a marker of fibrosis in chronic interstitial disorders. 27 Given that, it can explain the increase in some HCM patients and the subsequent poor outcomes.
ALP is one of the most widely used calcification markers in the physiological and pathological fields. 28 Physiological mineralization occurs in hard tissues, whereas pathological calcification occurs at several sites in the cardiovascular system, including the intima and media of vessels and cardiac valves. 29 It was reported that mitral annular calcification was present in 12 of 42 (29%) HCM patients, 30 accounting for a not small proportion. We assumed that there was a certain relationship between ALP and mitral annular calcification. A previous study demonstrated mitral annular calcification was more common in elderly HCM patients, with a presence of 13 in 17 (76%). 31 In our study, patients in higher ALP group were more likely to be older and suffer from comorbidity, which might partly contribute to higher mortality. Furthermore, calcifications of mitral annulus were found in 20% of HCM patients who were involved in a single pathogenic mutation in β-myosin heavy chain (MYH7). 32 Mitral valve abnormalities in MYH7 gene mutation, including mitral annulus calcifications, result in a worse phenotype expression versus that of MYBPC3 gene mutations. 32
Alkaline phosphatase was also found in white blood cells including neutrophils, eosinophils and basophils. The potential mechanism may represent confounding by another characteristic, such as inflammation. For instance, in an epidemiological study in Hong Kong Chinese, serum levels of ALP and C-reactive protein (CRP) were significantly correlated. 33 Another study of the US general population found that, after statistical adjustment for CRP, higher levels of serum ALP remained to be an independent predictor of mortality. In our study, however, baseline data on CRP were not obtained, and this relationship is speculative. Thus, the possibility that higher ALP is a marker for an underlying inflammatory state cannot be excluded.
Alkaline phosphatase was found related to several traditional cardiovascular risk factors such as abdominal obesity, increased systolic blood pressure, and plasma triglyceride, and smoking. 33 The potential mechanisms for the observation between ALP and mortality remain unclear. It could be beyond the mechanisms related to liver function, fibrosis, calcification and inflammation mentioned above. Further studies in different population, including HCM patients, measuring specific ALPs and exploring better characterizations of the pathophysiology that links higher ALP with excess mortality are needed.
There are some things important to say. In the present study, 32.1% of the whole HCM cohort had hypertension, consisting of a larger proportion than those previously reported. China faces a substantial amount of hypertensive people. To be more specific, a recent study containing 1 738 886 Chinese adults aged 35–75 years reported that nearly half had hypertension. 34 Last but not least, we did not include cardiac MRI data at baseline for the consideration that not everyone was examined, and then the MRI data were not completed. Even so, we thought it was more conform to reality. The exam price of cardiac MRI for some patients is too expensive to afford, they may prefer echocardiography since its role in diagnosing HCM is still indispensable. In addition, cardiac MRI has not been equipped widely but in a few tertiary hospitals. Besides, cardiac MRI is an advanced imaging technique, whereas there is a lack of proficient and experienced doctors to conduct, read and interpret, which is in line with the situation of most non-top hospitals.
The present study had certain limitations. Firstly, this is a retrospectively observational study, where causal relationships between ALP and prognosis cannot be as fully inferred as the prospective studies. Secondly, the sample might not reflect a real spectrum of distribution of disease severity. For example, in the present study, 91 out of 461 patients (19.8%) died during a median follow-up of 4.7 years (ranging: 0.1–10.8), however, a study based on 2 HCM centres reported 82 (8%) died over 7.2 ± 5.2 years of follow-up. 5 The present study was conducted in West China Hospital, one of the top tertiary referral centres in China, which might potentially resulted in Berkson bias for West China Hospital usually admitted critically ill patients. Thus, attention should be paid when the findings are extrapolated. Thirdly, some important covariates such as troponin and B-type natriuretic peptide (BNP)/N-terminal-proBNP (NT-proBNP) which were revealed to be associated with the disease severity and prognosis in HCM patients were not included in our cohort due to the incompleteness of the baseline data in several patients. Since this is the first study to explore the role of ALP in HCM patients, no evidence of relationship between ALP and the aforementioned markers could be found in this population. A study enrolling 10 patients with systemic amyloidosis found Pearson correlation coefficient between serum ALP and NT-proBNP was 0.13 (P value not significant). 35 Therefore, our preliminary conclusions on the independent predictive effect of ALP may be meaningful, and future studies should add BNP/NT-proBNP or troponin in the univariable and multivariable analysis to further explore its predictive value for all-cause mortality.
Conclusion
In a Chinese cohort study of adult HCM patients, our study demonstrates that serum ALP is an independent predictor of all-cause mortality. Alkaline phosphatase above 80 IU/L is associated with an excessive risk of all-cause mortality and might be helpful with risk stratification in HCM population. Exploration of biological mechanisms and causal possibility for that association may prove clinically useful for further confirmation of ALP as a risk marker in HCM population.
Supplemental Material
Supplemental Material – Prognostic significance of Serum Alkaline Phosphatase for All-cause Mortality in Patients with Hypertrophic Cardiomyopathy: a cohort of the hospitalized population
Supplemental Material for Prognostic significance of Serum Alkaline Phosphatase for All-cause Mortality in Patients with Hypertrophic Cardiomyopathy: a cohort of the hospitalized population by Lu Liu, Ying Xu, Shanshan Jia, Xiaoping Chen and Sen He in Annals of Clinical Biochemistry
Footnotes
Acknowledgement
We thank all staff members for data collection, data entry and monitoring as part of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Sichuan Science and Technology Program, China (Grant No. 2022YFS0186), and the National Natural Science Foundation of China (Grant No. 81600299), Key R&D Projects (Major Science and Technology Projects, grant Number: 22ZDYF1527) and Technological innovation R & D project of Chengdu Science and Technology Department (Grant No. 2020-YF05-00290-SN).
Ethical approval
Biomedical Research Ethics Committee, West China Hospital of Sichuan University (approval number: 2019–1147).
Guarantor
Xiaoping Chen and Sen He.
Contributorship
LL, YX and SSJ contributed to data collection, data entry, the conception of the work, the analysis and interpretation of data, and drafting the manuscript. XPC and SH contributed to the conception of the work, revising the draft for important intellectual content. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.