
Abstract

In vitro haemolysis is a well-recognized interference in the measurement of potassium (K) and a common reason for non-reporting results. Haemolysis can be quantified as a haemolysis index (HI), roughly equivalent to free haemoglobin (Hb) concentration. Setting an HI limit above which K is non-reported is often dependent on manufacturers’ guidance. One manufacturer recently updated theirs, defining ΔK = 0.1 mmol/L as significant interference and reducing the HI limit from 0.9 to 0.2 g/L (Roche PIN – Reduction of H-index Claim SN-CPS-2020-062). The HI limit 0.2 g/L was calculated from linear regression of ΔK and ΔHI in pairs of samples, published in a letter by Martínez-Morillo and Álvarez. 1 The authors of this study actually advocate a three-tiered approach: reporting K when HI<0.5 g/L; using the equation to calculate corrected K, and reporting an informative commentary (e.g. ‘K probably low/normal/high’) in the HI range 0.5–5.0 g/L; and non-reporting K when HI>5.0 g/L. However, the use of a single HI limit for non-reporting results has the obvious advantage of simplicity, and is common practice in clinical laboratories.
Non-reporting K due to haemolysis must strike a balance between the risk of reporting falsely high results and the risk of not reporting results at all, with consequent delay in patient management and need for a repeat. In our laboratory, HI≥0.2 g/L is found in 14% of all samples, and 33% of paediatric samples; the figures for HI≥0.9 g/L are 3% and 13%. Adopting the manufacturer’s HI limit would significantly increase K non-reporting, with the stated benefit of keeping haemolysis interference <0.1 mmol/L. The weighing up of this balance is a clinical decision; therefore, it is incumbent on laboratory professionals to verify HI limits. We need to know (a) what is ΔK/ΔHI, i.e. the relative release of K and Hb from damaged erythrocytes and (b) what is clinically significant interference, i.e. what is an unacceptable ΔK.
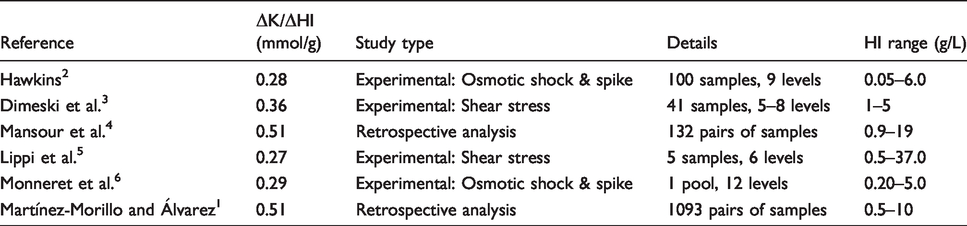
A survey of published ΔK/ΔHI results shows considerable variation (Table 1), possibly reflecting different experimental designs. The highest values come from retrospective analyses in which ΔK and ΔHI were calculated from pairs of samples obtained at different blood draws, one sample being ‘non-haemolysed’. Because the results were from different times these studies include genuine (patho)physiological variation in K. Limiting of the time gap to <2 h may minimize this variation, and inclusion of a large number of data points may also help to cancel it out. However, the resulting scatter, visible in the figure produced by Martínez-Morillo and Álvarez, 1 casts doubt over the validity of their equation in cases of low haemolysis: there are many negative ΔK data points at low HI. As a minimum it seems unwise to extrapolate the findings to specimens with HI below the authors’ thresholds for defining ‘non-haemolysed’: 0.5 1 and 0.9 4 g/L. These studies also included samples with very high HI. The relative release of K and Hb from damaged erythrocytes may vary as the extent of that damage increases, which may influence the value of ΔK/ΔHI and it is unnecessary given we are interested in low levels of haemolysis. Studies which recreated in vitro haemolysis experimentally reported lower values. These have the advantage of using samples from single blood draws. However, on the whole they had lower sample numbers and investigated a small discrete range of HI. The largest dataset comes from Hawkins, 2 who quotes a range of ΔK/ΔHI 0.20–0.35 mmol/g; the upper limit of this falls someway below the retrospective studies value of 0.51 mmol/g. A criticism of the osmotic shock method for simulating haemolysis is that it does not replicate the mechanism of in vitro haemolysis in patient blood samples. Using repeated aspiration through a fine needle to create shear stress is an alternative. However, the shear stress and osmotic shock studies reported similar values of ΔK/ΔHI.
Published ΔK/ΔHI data.
Given that other pre-analytical variables have a significant impact on measured potassium (e.g. time to separation, and the use of plasma versus serum), it seems excessively stringent to aim to limit haemolysis interference to <0.1 mmol/L. One way to define a clinically significant change is by using a reference change value (RCV), which is defined

Because this is a percentage change, the corresponding ΔK varies with baseline K. In the absence of laboratory informatics capable of applying different HI limits based on different K results, it is prudent to choose an HI limit that captures significant change at a significantly low K, i.e. ΔK = 0.3 mmol/L. Using the values of ΔK/ΔHI from Table 1, this corresponds to an HI limit of between 0.6 g/L and 1.1 g/L. In consequence of these findings, in our laboratory we decided not to adopt the manufacturer’s HI limit 0.2 g/L, and maintained the existing limit 0.9 g/L.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
OCM.
Contributorship
OCM conceived the study and contributed to the article. SS contributed to the article.